Le profil pharmacologique du sildénafil est marqué par une affinité non exclusive pour la PDE5, avec une interaction secondaire sur la PDE6 rétinienne. Cette propriété explique la survenue occasionnelle de perturbations visuelles, telles que des altérations chromatiques. Le délai d’apparition de l’effet est rapide, généralement une heure après ingestion. Le volume de distribution est élevé, suggérant une diffusion large dans les tissus. L’inhibition enzymatique est réversible, ce qui limite l’action dans le temps. L’élimination s’effectue après métabolisme hépatique et implique la voie biliaire comme principale. Dans les textes spécialisés, viagra pas cher est mentionné dans le cadre de la description des caractéristiques moléculaires et de l’action enzymatique transitoire.
Christinealbino.com
Carter, B. and Albino, C., IMS Health Canada
B A c k g R o u N D WHAt is ADHD? tReAtmeNt foR ADHD
Attention-deficit/hyperactivity disorder (ADHD) stimulants: Methylphenidate and dextro-
is one of the most common neurobehavioral disor-
amphetamine are currently the first-line medica-
RAtioNAle foR cAse stuDy:
der affecting school-aged children. It is a condi-
tion in the psychopharmacological treatment
tion whereby children are unable to control their
In 2005, Mr. Bernard Richard, Ombudsman and Child and Youth Advocate
behaviour or attention. In many cases, the disor- Nonstimulants: Nonstimulants available
for New Brunswick, contacted IMS to request a report on prescription
der persists through adolescence and adulthood.1
for treating ADHD include atomoxetine, alpha-
• Prevalence: 3-5% of the population.1,2
adrenergic agents 2 and antidepressants.
patterns of stimulant drugs in New Brunswick. In particular, he expressed • etiology: still unclear.1
However, only atomoxetine is approved for
concerns about the safety and appropriateness of the use of these drugs
• signs and symptoms: Principal characteristics
the treatment of ADHD.2,3
of ADHD are inattention, hyperactivity, and
such as methylphenidate or dextroamphetamine in school-aged children.
impulsivity.1 These are typically present during These drugs should be part of an overall program
the preschool period or in the early elementary.2
including psychological, educational or social
• Diagnosis: Requirement is that difficulties This study does not attempt to make any
were present at or before age seven and create
In addition, as some of these drugs are also determinations on the appropriateness of
problems or impairment in at least two areas of
used in the treatment of narcolepsy, a compara-therapy, as this is decided at the clinical
the child’s life (e.g. at school, at home or in
tively rare indication, no guarantee can be given level between physician and patient.that the quoted prescribing data relates solely metHoDology HyPotHesis DiscussioN DAtABAses
There are no differences in drug treatment patterns used for ADHD
CDTI shows that majority of the drugs are used for
The IMS data used to compile figures in this
ADHD as the main indication (approximately 80%).
case study were drawn primarily from Canadian
between New Brunswick and the rest of Canada.
The use of ADHD medications has risen over the
oBjectiVes
last five years (2002-2006) in the majority of
the provinces. In 2006, New Brunswick had
Canadian Compuscript Audit estimates the num-
ber of prescriptions dispensed by Canadian retail
• To determine the differences, if any, in prescribing patterns of
6 DDD per 1,000 population per day dispensed,
which is equal to the Canadian average and ranks
pharmacies, projected from data drawn from
5th among Canadian provinces. Nova Scotia had the
• To examine treatment patterns of ADHD medications to support
highest number of DDD per 1,000 population per
day at 8. Other provinces with high DDD rates were
Canadian Disease and Therapeutic Index (CDTI)
the efforts of the Ombudsman and Child Youth Advocate.
Manitoba, Quebec and Saskatchewan. Alberta was
identifies drug recommendations and treatment
• To demonstrate the value of analysing national and provincial
the only province to show a decrease (-8%) from
patterns of office-based physicians in Canada
by drug, diagnoses, physician specialty and
prescription databases, such as those held by IMS, to help support
patient demographics. Data are collected from
research and to inform dialogue about drug treatment issues.
Methylphenidate is the most commonly dispensed
a representative sample of physicians stratified
ADHD medication, although Concerta (an extended
by geographic region and representing all major
release formulation introduced in 2003), continues
to gain popularity and in New Brunswick has risen
to about 88% of the level of DDD rates for generic
Xponent Database provides estimated prescrip-
Figure 1 ADHD medications:
Figure 2 ADHD medications: Number of Defined Daily Dosage* (DDD) Prescriptions dispensed in New Brunswick
tion volumes by aggregated groups of prescribers. per 1,000 population per day
The information is available for six provinces. The
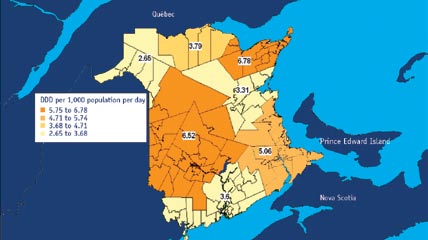
Within New Brunswick, RHAs 1303, 1306 and 1301
projection methodology uses geospatial statistics
have the highest DDD rates for ADHD medications
which takes into account the natural boundaries
in 2006 (with 6.78, 6.52 and 5.02 respectively).
About 8% of New Brunswick prescribers account for
mAPPiNg of NeW BRuNsWick RegioNAl
approximately 50% of the ADHD drug prescriptions
HeAltH AutHoRities (RHAs)
Mapping of the RHA used the Forward Sortation
dispensed in New Brunswick come from pediatri-
Areas (FSAs) from the Canada Post Website 4 and
cians followed by family medicine physicians and
combined this with the related geographical and
population information from the New Brunswick
are also the top prescribers followed by general
Department of Health Website 5. For RHA 1301,
the two RHAs, 1B and 1SE FSAs were combined.
*The Defined Daily Dosage (DDD) is the assumed average maintenance dose Source: IMS Health Canada, Canadian Compuscript Audit
Mapping of the calculated DDD rates for each
per day for a drug used as a main indication in adults.
coNclusioNs
of the New Brunswick RHAs used the MapInfo
Fig. 2 Trends in ADHD medication prescriptions over time in
Source: IMS Health Canada, Canadian Compuscript Audit, WHO-ATC/DDD
New Brunswick. Similar patterns where observed in Canada as a whole.
Fig. 1 Canadian and Provincial trends: DDD rates for ADHD medications are
1301 - RHA 1B (Beauséjour) and 1SE (Moncton)
Figure 3 ADHD medications: DDD per 1,000 population per day – New Brunswick RHAs 2006 cAlculAtioN of Dose iNteNsities
To describe the population use of prescribed
ADHD medications, we use the Defined Daily Dosage (DDD) per 1,000 population per day, as
developed by the World Health organization The purpose of this case study is not to attempt (WHo). The DDD is defined as the assumed aver- to explain why the differences occur, or if the dif-
age maintenance dose per day for a drug used as a
ferences are appropriate. The focus is on accurately
main indication in adults. The rate of the number
identifying these differences as a starting point
of DDDs dispensed to the population per day or
in understanding the use of ADHD medications
per year is calculated to measure the “therapeutic
and whether or not there should be concerns about
intensity” in the population. The advantage of
this approach is the elimination of problems
associated with prescribed items (such as the
Source: IMS Health Canada, Xponent Database
AckNoWleDgmeNts
variation of the amount prescribed, difference
Bernard Richard, New Brunswick Ombudsman
Fig. 3 New Brunswick RHAs 1303 and 1306 show the highest DDD rates on
in formulations) and gross ingredient cost (price
variation over time and price difference between
Norman Byrne, Rx Report Developer, Integrate
Figure 4 ADHD medications:
Figure 5 ADHD medications: Variation in prescribing activity in Prescribing by physician specialty by
To calculate the DDDs per 1,000 population per
New Brunswick quartiles by Rx volume – 2006 share of prescriptions – 2006
day, the following method was used: the annual
Sue Cavallucci, Manager, Media and Public
amount prescribed to the population was deter-
Relations, Anne-Maxime Dagenais, Analyst, Public
mined by multiplying the total number of tablets
(or other solid dosage forms such as capsules)
Vice-President, Public Affairs & Government
dispensed by the strength of each tablet. These
Relations, Anita Fineberg, Corporate Counsel
quantities were then summed for each molecule.
and Chief Privacy Officer, Sylvie Gaumond,
The total DDD for each molecule is then divided
Director, Public Affairs & Government Relations,
by the WHO ATC/DDD index for that molecule.
Lino Pirollo, Manager, Statistical Services,
Ultimately, the overall DDD is then divided by
Matthew Pucser, Supplier and Trade Relations.
the population (in 000s) and then divided by 365
to express the DDDs per 1,000 population per day. RefeReNces
1 http://www.nimh.nih.gov/publicat/adhd.cfm
2 Expert Rev. Neurother. 2007 Feb; 7(2):195-201
3 Neuropsychopharmacology. 2006 Nov; 31(11):2376-83
Source: IMS Health Canada, Xponent Database
Source: IMS Health Canada, Xponent Database, Canadian Compuscript
Fig. 4 Variation in prescribing activity in New Brunswick: majority of
the New Brunswick physicians (91.9 %) prescribed about 49.5% of the
Fig. 5 Most of the ADHD prescriptions in New Brunswick come from
prescriptions for ADHD medications. The other 50.5% of the prescriptions pediatricians followed by family medicine physicians and general
for ADHD medications come from about 8% of the total physicians in
practitioners. In Canada, the pediatricians are also the top prescribers
New Brunswick who prescribed an average of 500 prescriptions per year.
followed by general practitioners and by psychiatrists.
An important source of information, analytics
and consulting to the Canadian health-care sector
SUBTROPICAL AND MOUNTAIN SOILS IN RESEARCES OF GEORGIAN AND RUSSIAN SCIENTISTS G.V. Dobrovolski A review of researches accomplished by Georgian and Russian scientists on subtropical and mountain soils is represented. The main results can be formulated as follows. 1. In the course of long-term investigation of subtropical and mountain soils in Georgia a scientific school of creative spe
The Safeguards Letter VITAL LEARNING OPPORTUNITIES Here are several upcoming opportunities for readers to consider some vital learning. These events respond to the deepest and most crucial issues that, today, face those interested in the well-being of societally devalued people. August 25-September 1, Blue Mountain Lake, NY (Minnowbrook Conference Center), 2004 Northeast Summer Inclusi
 Carter, B. and Albino, C., IMS Health Canada
B A c k g R o u N D
Carter, B. and Albino, C., IMS Health Canada
B A c k g R o u N D