Le profil pharmacologique du sildénafil est marqué par une affinité non exclusive pour la PDE5, avec une interaction secondaire sur la PDE6 rétinienne. Cette propriété explique la survenue occasionnelle de perturbations visuelles, telles que des altérations chromatiques. Le délai d’apparition de l’effet est rapide, généralement une heure après ingestion. Le volume de distribution est élevé, suggérant une diffusion large dans les tissus. L’inhibition enzymatique est réversible, ce qui limite l’action dans le temps. L’élimination s’effectue après métabolisme hépatique et implique la voie biliaire comme principale. Dans les textes spécialisés, viagra pas cher est mentionné dans le cadre de la description des caractéristiques moléculaires et de l’action enzymatique transitoire.
Cocukenfeksiyon.org
Nonsurgical Treatment of Adenoidal Hypertrophy with Cefuroxime Axetil and Intranasal Mometasone Furoate Combination Adenoidal Hipertirofinin Sefuroksim Aksetil ve Mometazon Furoat ile Cerrahi D›fl› Tedavisi
Semanur Kuyucu1, Necdet Kuyucu2, Selma Unal2, Demir Apayd›n3
Mersin University, Faculty of Medicine Department of Pediatrics, Pediatric Allergy Unit1,
Pediatric Infectious Diseases Unit, 2Department of Pediatrics and 3Department of Radiology, Mersin, Turkey
Aim: Adenoidal hypertrophy causes substantial mor-
Amaç: Adenoidal hipertrofi çocukluk ça¤›nda önemli
bidity in childhood. This prospective randomized
bir morbidite nedenidir. Bu prospektif, randomize ça-
open-label trial was conducted in order to evaluate
l›flma semptomatik adenoidal hipertrofili olgularda se-
the efficacy of cefuroxime axetil (CEF) and mometa-
furoksim aksetil (CEF) ve mometason furoat nazal
sone furoate nasal spray (MFNS) combination treat-
sprey (MFNS) kombinasyon tedavisinin, her iki tekli te-
ment in symptomatic adenoidal hypertrophy, in com-
davi ve kontrollere göre etkinli¤ini belirlemek üzere yü-
parison to either treatment alone, or controls (CON). Material and Methods: Three to 14 years old 128 Gereç ve Yöntem: Semptomatik adenoidal hipertrofi-
children with symptomatic adenoidal hypertrophy
si olan 3-14 yafl grubundan 128 çocu¤a randomize
were randomized to receive a 4 week-course of CEF
olarak 4 hafta süreyle CEF (30 mg/kg/g bölünmüfl 2
(30 mg/kg in 2 divided doses daily, po), MFNS
dozda, po), MFNS (100 mg günde 1 kez), CEF art›
(100 mg once daily), CEF plus MFNS (in same doses),
MFNS (ayn› dozlarda) veya control (CON) olarak nor-
or normal saline as control (CON). After cessation of
mal serum fizyolojik verilmifltir. Tedavinin kesilmesin-den sonra hastalar 2 ay süreyle takip edilmifltir. Temel
therapy, they were followed-up for 2 months. Main
sonuç ölçütleri olarak 4. hafta ve 12. hafta kontrollerin-
outcome measures were changes from baseline in
de total semptom skorunda bazale göre de¤ifliklik ve
total symptom score, and air column/soft palate
yan boyun grafisinde nazofarenks hava kolonu/yumu-
(AC/SP) ratio on lateral neck radiograph on the 4th
flak damak (AC/SP) oran› kullan›lm›flt›r.
Bulgular: Dördüncü haftada ortalama semptom sko- Results: The improvement in mean symptom score
runda bazale göre düzelme CEF + MFNS grubunda
of CEF plus MFNS group was significantly (p= 0.017)
kontrol grubuna göre anlaml› olarak yüksek bulunmufl-
higher than CON group at the end of 4th week. Incre-
tur (p=0.017). Kombine tedavi alan grupta 12. haftada
ase in mean AC/SP ratio from baseline to 12th week
ortalama AC/SP oran›nda bazale göre art›fl di¤er grup-
in CEF plus MFNS group was significantly greater
lara göre anlaml› olarak yüksek bulunmufltur
than CON group and other two groups (p= 0.03). Ne-
(p= 0.03). Tek bafl›na CEF veya MFNS tedavileri hiçbir
ither CEF, nor MFNS alone was better than CON on
kontrol tarihinde skor veya radyolojik olarak CON gru-
any visit. The changes in symptom scores or radiog-
bundan üstün bulunmam›flt›r. Atopik ve nonatopik has-
raphic measurements were not different between
talarda semptom skoru veya radyolojik ölçümdeki de-
Yaz›flma Adresi
¤ifliklikler farkl› bulunmam›flt›r.
Correspondence Address
Conclusion: Oral CEF plus MFNS combination thera-
Sonuç: Sonuç olarak, bir ay süreli oral sefuroksim ve
py of one month’s duration may delay, or substitute,
nazal mometason furoat sprey kombine tedavisinin ha-
surgical intervention in some pediatric outpatients
fif-orta derecede adenoid hipertrofisi olan çocuklarda
with mild to moderate adenoidal hypertrophy.
semptomatik ve radyolojik düzelme sa¤layarak cerrahi
tedaviyi geciktirebilece¤i veya engelleyebilece¤i tespit
Key words: Adenoidal hypertrophy, adenoids, topi-
edilmifltir. (Çocuk Enf Derg 2007; 1: 6-12)
Tel: +90 324 337 43 00/1623Fax: +90 324 337 29 25
cal steroids, cefuroxime axetil, mometasone furoate
Anahtar kelimeler: Adenoid hipertrofisi, adenoidler,
topikal steroidler, sefuroksim aksetil, mometazon
Nonsurgical Treatment of Adenoidal Hypertrophy
Introduction Study Design This was an open-labelled, controlled study. Eligible pa-
Adenoidal hypertrophy and recurrent adenotonsillitis are
tients were randomized to one of the following treatment
common disorders which cause substantial morbidity in
groups for 4 weeks: cefuroxime axetil (CEF), 30 mg/kg/day
pediatric age group (1). Severe adenoidal upper airway
per os in 2 doses (Group 1); mometasone furoate nasal
obstruction causing obstructive sleep apnea (OSAS) and
spray (MFNS), 50 mg into each nostril (100 mg total) once
cardiorespiratory syndrome may necessitate urgent surgi-
daily (Group 2); MFNS plus CEF, in the same doses (Group
cal removal of the adenoid (2,3). Lesser degrees of adeno-
3); or normal saline as control (CON) (Group 4). At entry the
idal hypertrophy complicated by chronic sinusitis, recur-
patients in group 2 and 3 were instructed in the proper
rent/chronic serous otitis media and/or significant obstruc-
technique of nasal spray application. At the end of the fo-
tive symptoms are among other indications for surgical in-
urth week study medications were stopped and patients
tervention (4). Although regarded as a generally safe proce-
were reevaluated after 8 weeks. Informed consent was ob-
dure, adenoidectomy and/or tonsillectomy can be compli-
tained from the parents of study participants. The study
cated by reactions such as bleeding, adverse anesthetic
was approved by the Ethical Committee of Mersin Univer-
events, dehydration, pain, and even death (5). Hence, effec-
tive medical treatment alternatives to surgery for relief of
Evaluations and Outcome Measures
adenoidal obstruction may be very valuable, especially
Study subjects had a thorough clinical and radiological
when surgery is not clearly indicated, or possible.
assessment at baseline and on the 4th and 12th weeks af-
Nonsurgical treatment modalities for adenoidal hypert-
rophy are limited. A prolonged course of beta-lactamase
resistant antibiotic therapy resulted in both the reduction of
Initial evaluation of the subjects included history and
symptoms and the need for surgery in chronic adenotonsil-
physical examination, symptom scoring, lateral neck and
lar hypertrophy (6). It has been shown that nasal topical
sinus roentgenograms, total IgE levels, specific IgE levels,
corticosteroids can significantly ameliorate obstructive in-
skin prick test (SPT) with inhalant and food allergens (38 al-
dexes in children with adenoidal hypertrophy (7), or OSAS
lergens), complete blood count, serum C-reactive protein,
associated with adenotonsillar hypertrophy (8).
liver function tests, blood urea nitrogen, urinanalysis, immu-
The aim of this study was to evaluate the efficacy of int-
noglobulin levels and throat cultures. Initial historical evalu-
ranasal corticosteroid and prolonged beta-lactamase resis-
ation accomplished by face-to-face interview with parents
tant antibiotic combination treatment with either treatments
included the inclusion and exclusion criteria, frequency of
alone, and normal saline as control in reduction of adenoid
upper respiratory infection, tonsillitis, otitis media, sinusitis
size and nasal airway obstructive symptoms in pediatric
and lower respiratory infection, individual allergic symp-
toms and diagnoses, and family atopy.
The main outcome measures were the changes in total
symptom scores and adenoid size on lateral neck radiog-raphs from baseline to 4th and 12th weeks. The frequency
Study Population
of intervening illnesses and antibiotic usage were secon-
Three to fourteen years old children who were admitted
to the pediatric outpatient clinics with chronic nasal obst-
The symptom scoring system was a modification of the
ructive symptoms were recruited to this study. Inclusion
scores used in previous studies (6-8) and included the fol-
criteria were: (1) presence of any of the following signs and
lowing symptoms: snoring; mouth breathing awake; mouth
symptoms of nasal obstruction; snoring, mouth breathing
breathing asleep; nasal congestion; hyponasal voice; chro-
awake, mouthbreathing asleep, restless sleep or difficulty
nic nasal discharge; daytime drowsiness, or hyperactivitiy;
breathing while asleep, nasal congestion, chronic nasal
restless sleep; sleep apnea <15 sec; night cough; and po-
discharge, sleep apnea and hyponasal voice for at least 2
or oral intake/weight loss. Each symptom was scored as
months; and (2) adenoidal hypertrophy assessed on lateral
follows: none (0 point), rarely (1 point), frequently (2 points),
neck radiograph as an air column/soft palate ratio < 1 (9). Exclusion criteria were: (1) use of any nasal, inhaled or
constantly (3 points). Scores from eleven symptoms were
systemic corticosteroids within the past 6 months; (2) use
added together to provide a total symptom score of 33.
of antibiotics or any nasal medications within 1 month of
Lateral neck radiographs were taken and interpreted by
entering the study; (3) history of apnea lasting more than 15
the method of Cohen and Konak by a blinded radiologis (9).
seconds; (4) any craniofacial anomaly; (5) a history of
According to this method, the thickness of the soft palate
hypersensitivity to penicillin, cephalosporin or corticostero-
(SP) in its superior anterior part and the airway column (AC)
ids; (6) a history of immunodeficiency; (7) any history or la-
immediately posterior to it were measured and AC/SP ratio
boratory evidence of cardiac, hepatic, or renal disease; and
was calculated. The measurement was done about 1 cm
(8) a history of chronic epistaxis. Patients were enrolled bet-
below the upper end of the soft palate in children > 3 years
ween September 2001 and October 2002 in order to over-
of age and half a centimetre in younger children. A radiog-
raphic example of this method is demonstrated in Figure 1.
Nonsurgical Treatment of Adenoidal Hypertrophy
Degree of obstruction was graded as follows: AC/SP ≥ 1
ses and/or antibiotic usage over the changes in symptom
(grade 0 or no obstruction), AC/SP= 0.50-0.99 (grade 1 or
scores and radiographic adenoidal indexes from baseline
mild obstruction), AC/SP= 0.01-0.49 (grade 2 or severe
to 4th and 12th weeks. The relation between total symp-
obstruction), AC/SP= 0 (grade 3 or total obstruction).
tom score and AC/SP ratios at each week was determined
On the 4th and 12th week visits parents were intervi-
using regression and correlation analysis. Values were
ewed for any intervening illness (upper respiratory infection,
expressed in mean ± standard error, p<0.05 was conside-
tonsillopharyngitis, otitis media and sinusitis) and antibiotic
treatment since the last visit and these were recorded. Compliance with medications and side effects of the treat-
ments were also assessed by parental interview. Complian-ce with medications was described by the number of mis-
A total of 128 patients were included in the study. Num-
sing doses per month. Renal and hepatic function tests we-
ber of patients that completed the treatment period of four
weeks was 28 in group 1, 37 in group 2, 25 in group 3, and
Serum total IgE levels were measured by nephelometric
38 in group 4. One patient in group 2 was withdrawn from
method (Bade-Behring Inc., Germany). Skin prick tests we-
the study because of medication side effect (epistaxis). Ot-
re performed with 38 inhalant and food allergens (Allergop-
her patients were lost to follow-up which may be due to eit-
harma, Germany) of general and local relevance in a stan-
her treatment failure or success. Fourteen, 21, 12, and 20
dardized fashion. Any wheal reaction ≥ 3 mm when the ne-
patients completed through the 12 weeks of follow-up, in
gative control was substracted was considered as a positi-
the respective groups. Proportion of drop-outs among gro-
ve skin prick test reaction. Levels of IgE antibodies to inha-
ups was similar (50.0, 43.3, 52.0, and 47.4%, for group 1,
lant and food allergens were studied by fluoroenzymeim-
munoassay method (UniCAP, Pharmacia and Upjohn,
Comparison of admission characteristics of the patients
Sweden). Any allergen-specific IgE level ≥ 0.70 kU/L was
according to study groups are shown in Table 1. There we-
considered as positive. Atopy was defined as the presence
re no significant differences between age and gender dist-
of one or more positive skin test reactions and/or one or
ributions, frequency of previous (during the last 12 months)
more positive allergen-specific IgE examination.
upper and lower respiratory infections (tonsillitis, otitis me-
Statistical Analysis
dia, sinusitis, and bronchitis), family history of atopy and
Analysis of variance and chi-square tests were used to
personal history of atopic disease (physician-diagnosed
compare admission characteristics of the patients betwe-
asthma, allergic rhinitis, or atopic dermatitis) between the
en the study groups. Analysis of variance and paired t-test
study groups. Mean baseline white blood cell count of the
were used to interpret the changes in symptom scores and
patients was 8,450 ± 2,370 /mm3, with no significant diffe-
radiographic adenoidal indexes from baseline to 4th and
rences between the groups (p> 0.05). A clinical and radiolo-
12th weeks between study groups. Student t-test was
gical diagnosis of sinusitis was present in 48.0% of patients
used to evaluate the effects of gender, physician-diagno-
at entry and the frequency was not statistically different
sed atopic disease, family history of atopy, sinusitis, atopy
between the treatment arms. Thirty-four point one per cent
(SPT and/or specific IgE exam), and any intercurrent illnes-
of the whole study group was found to be atopic accordingto SPT and/or specific IgE levels. The most common aller-gens were mites, cockroach, pollens, and dog epithelium. The mean air column/soft palate (AC/SP) ratio on lateralneck radiographs and distribution of the degree of obstruc-tion at entry are shown in Table 1. There were no significantdifferences between these baseline values of nasopharyge-al airway patency, or baseline symptom scores among thetreatment groups (p>0.05).
Compliance with medications was assessed by paren-
tal interview at the end of the fourth week. Mean misseddoses per week were 0.16±0.4 for group 1, 0.25±0.50 forgroup 2, none for group 3 and 3.00±1.41 for group 4. Num-ber of missed doses was significantly higher for group 4when compared to other groups (p<0.01). Side effects as-sociated with medications included one case of epistaxisfrom group 2. One patient from group 1 and one patient
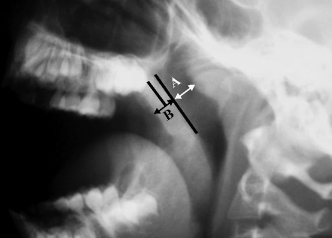
Figure 1. Radiographic evaluation of adenoid size by the method
from group 3 developed mild limited diarrhea not requiring
of Cohen and Konak (9). Thickness (mm) of “Airway column” (A)and “Soft palate” (B) is measured and A/B ratio is calculated in
cessation of therapy. No patient developed any hepatic or
order to evaluate nasopharyngial airway patency
renal function abnormalities during the treatment.
Nonsurgical Treatment of Adenoidal Hypertrophy
Table 2 shows the main outcome measures; changes in
were not significant. Age, gender, physician-diagnosed ato-
mean symptom scores and AC/SP ratios from baseline
pic disease, family history of atopy, sinusitis, total IgE levels,
through 12 weeks according to study groups. In all groups,
atopy (SPT and/or specific IgE exam), and any intercurrent
mean symptom scores showed a significant decline from
illnesses and/or antibiotic usage during the treatment period
baseline to 4th, and 12th weeks (p<0.001). When the groups
(0-4 wks) and on follow-up (4-12 wks) were not significantly
were compared with each other, the improvement in mean
related to the changes in symptom scores according to reg-
symptom score of group 3 was significantly (p= 0.017) hig-
her than that of group 4 at the end of the treatment period
All the groups showed a significant increase in mean
(0 to 4th week), and better, but not significant, than other
AC/SP ratios and decrease in grade values from baseline to
groups at the 12th week. Differences across other groups
4th and 12th weeks. When the groups were compared with
Table 1. Admission Characteristics of Study Groups Characteristic CEF-Group 1 MFNS-Group 2 CEF + MFNS –Group 3 CON-Group 4
PD- physician-diagnosed, CEF- cefuroxime axetil, MFNS- mometasone furoate nasal spray, CON- control (normal saline), AC/ SP- airway column/soft palate ratio on neck radiograph
Table 2. Changes in Symptom Scores and Radiographic Adenoidal Indexes from Baseline to 4th and 12th weeks Among Study Groups CEF-Group 1 MFNS-Group 2 CEF+MFNS-Group 3 CON-Group 4
Values are given as mean±SE* Significantly different from group 4, p=0.017. ** Significantly different from other groups, p=0.035
10 Nonsurgical Treatment of Adenoidal Hypertrophy
each other for the changes in nasal airway patency, the inc-
Studies have revealed that adenoidal hypertrophy is
rease in AC/SP ratio from baseline to 12th week was signi-
frequently accompanied by significant adenoidal bacterial
ficantly higher in group 3 than the other groups (p= 0.03).
infection and the importance of the adenoid as a reservoir
Also, the mean decrease in grade value of lateral radiog-
of pathologic bacteria associated with airway and ear di-
raphs showed a similar result of borderline significance
sease has been stressed (11,12) Streptococcus pyogenes,
(p= 0.06). There were no significant differences between
Haemophilus influenzae, Staphylococcus aureus, Mora-
the changes across other groups and other weeks. Age,
xella catarrhalis and Streptococcus pneumoniae are most
gender, physician-diagnosed atopic disease, family history
commonly found organisms in cultures of the adenoids
of atopy, presence of sinusitis, total IgE levels, atopy (SPT
(6,11,13). The proportion of beta-lactamase-producing or-
and/or specific IgE exam), and any intercurrent illnesses
ganisms (BLPOs) ranged from 22% to 83%, with signifi-
and/or antibiotic usage during the treatment period
cantly higher values in recurrent adenoiditis cases and
(0-4 wks) and on follow-up (4-12 wks) were not significantly
children with rhinosinusitis symptoms (6,13,14). These da-
related to the changes in AC/SP ratio according to regres-
ta provided the basis for selection of cefuroxime axetil,
which has a broad spectrum of activity against this bacte-
The mean number of intercurrent illnesses (rhinopharyn-
rial spectrum, as a prolonged course of eradicating anti-
gitis, tonsillitis, otitis media and sinusitis) during the treat-
microbial therapy in the present study. We did not have a
ment period (0-4 wks) and from 4th to 12th weeks were
bacteriological profile of our patients, since our study did
0.25±0.43, and 0.44±0.71, respectively for the whole study
not include surgically removed adenoid tissue cultures,
group. There were no significant differences between the
which is the optimal method of evaluating adenoidal bac-
treatment arms. The rate of antibiotic use for any intercur-
teriology. The emergence of resistant strains with a prolon-
rent illness was not significantly different among study gro-
ged course of broad-spectrum antibiotic may be a draw-
back to this kind of treatment. Sclafani et al. have shown
The correlation between total symptom score and
that a 30-day course of amoxicillin/clavulanate signifi-
AC/SP ratios at each week was evaluated by the Pearson
cantly reduced the need for adenoidectomy in obstructive
correlation coefficient. There was a significant negative li-
adenotonsillar hypertrophy in short- and long-term follow-
near correlation between symptom scores and AC/SP ratio
up and did not result in any increase in antibiotic-related
on the nasopharyngeal radiographs with a correlation coef-
sequelae (6). In the present study we could not show a sig-
ficient of – 0.256 (p= 0.004) for baseline, - 0.353 (p= 0.000)
nificant effect of cefuroxime axetil alone, an antimicrobial
for 4th week, and –0.403 (p= 0.000) for the 12th week.
with a similar spectrum of activity, on symptoms or adeno-id size when compared to controls. However, when com-
Discussion
bined with a topical nasal corticosteroid, MFNS, a signifi-cant amelioration of symptoms and a decrease in adenoid
The present study revealed that oral cefuroxime axetil
and intranasal mometasone furoate combination therapy of
It is currently accepted that adenoidal hypertrophy is
one month’s duration resulted in significant improvement in
caused by the antigen-stimulated increased activity of
symptom scores and, on the long-term, adenoidal size in
lymphocytes (15). Fujiyoshi et al. have demonstrated that
children with adenoidal hypertrophy, when compared to
hypertrophied adenoidal tissue showed evidence of immu-
controls and either treatment alone. Neither CEF, nor
nologic activation and chronic inflammation in patients un-
MFNS treatments were superior to normal saline, or to
dergone adenoidectomy surgery (16). Intranasal corticoste-
roids significantly affects the production and/or activity a
Adenoidal hypertrophy is a common disorder of pediat-
variety of proinflammatory mediators, including cytokines,
ric population frequently resulting in complications such as
adhesion molecules, mast cells, eosinophils and T
chronic sinusitis, otitis media and OSAS leading to impor-
lymhocytes, probably through local actions in the nasal mu-
tant morbidity and a high rate of outpatient admissions. Alt-
cosa (17). They also decrease vascular permeability and
hough adenoidectomy is the most effective treatment mo-
edema. Hence, these profound antiinflammatory effects
dality for relief of obstructive symptoms and related disor-
may help to decrease the immunologic activation shown in
ders it may not be desirable in many patients because of
hypertrophied adenoid tissue and reduce the adenoid size.
potential complications and parental reluctance about sur-
There have been contradictory reports about the effects
gery (4,5). Moreover, adenoidal tissue may regrow after sur-
of glucocorticoids in adenoidal hypertrophy and/or accom-
gical removal, as we have seen in two of the study patients
panying OSAS. A 5-day course of oral prednisone was fo-
(5). Some authors recommend a conservative treatment
und to be ineffective in improving OSAS and adenoidal
strategy until the child is 8 to 10 years old (10). Hence, a sa-
obstruction in 1 to 12 years old children (3). Brouilette et al.
fe non-surgical treatment option with sustained effects on
have shown a moderate improvement in pediatric OSAS,
airway obstruction may be preferable in adenoidal hypert-
but no significant changes in symptom scores or adenoidal
rophy except for cases needing urgent surgical removal (2).
size with a 6-week course of fluticasone nasal spray in 25
Nonsurgical Treatment of Adenoidal Hypertrophy
children with proven OSAS (8). An 8-week double-blind,
agnosed allergic rhinitis. Neither a physician diagnosed
placebo-controlled cross over study of standart-dose nasal
atopic disease, nor atopy predicted the degree of res-
beclamethasone revealed a significant reduction in adeno-
ponse to any kind of treatment in our study. Therefore,
idal size and obstructive symptoms in children with adeno-
the beneficial clinical and radiological effects of combina-
idal hypertrophy (7). The latter study also revealed a signifi-
tion therapy on adenoidal hypertrophy were independent
cant carryover effect of beclamethasone from 4 to 8 weeks.
of atopy, any atopic disease, or rhinosinusitis.
However, age effect over the response was not clear and
There has been controversy about the assessment met-
the sample size was relatively small.
hod of adenoidal size in clinical practice. Although endos-
Mometasone furoate 100 µg once daily was chosen
copy is the most accurate method of assessment, radiog-
as an appropriate and safe topical nasal corticosteroid
raphy is frequently used for adenoidal evaluation among pe-
regimen in our study. In children with perennial allergic
diatricians. Wormald et al. have compared the symptom
rhinitis no suppression of growth, or other adverse ef-
score and four different and commonly used radiological
fects was seen after one year of treatment with MFNS,
measurement methods to the endoscopically determined
100 µg QD (once daily) in 3 to 9 years old children (18). In
percentage obstruction of the post nasal space by the ade-
a dose-response relationship study of MFNS, 100 µg on-
noids (22). They found that the symptomatology score had
ce daily was found as the most appropriate, safe and ef-
the best correlation with endoscopy. Among the radiologi-
ficient therapeutic dosage in the treatment of SAR in 6 to
cal methods they evaluated, the method of Cohen and Ko-
11 years old children, but MFNS 200 µg provided no ad-
nak (9) provided the highest predictive value and best ove-
rall performance when compared to other methods (22).
There were no significant differences in markers of ade-
The importance of measuring the residual nasopharyngeal
noidal obstruction between MFNS and control groups in
airway rather than the adenoidal thickness has been stres-
the present study. However, prolonged oral antibiotic and
sed by other authors (23). Because of these, we have used
MFNS combination therapy of one month’s duration was
the radiological method of Cohen and Konak, which is ba-
significantly superior to controls both clinically and radiolo-
sed on the ratio of residual nasopharyngeal airway to soft
gically. This result may point out that chronic adenoidal
palate thickness. We did not employ endoscopic examina-
hypertrophy and/or adenoiditis should be regarded as a co-
tion since small children not suitable for cooperation were
existence of a chronic infectious and a chronic inflamma-
mostly included in the study. The discrepancy between
tory disorder. Hence, treatment modalities directed at only
symptom scores and radiological examination, which is a
one component may fail to be successful. Antibiotic and
drawback of this study, could be overcomed if endoscopy
MFNS combination resulted in significant amelioration of
airway obstruction not only at the end of treatment period
One of the limitations of this study was that about 50%
but also 2 months after discontinuation of therapy. This
of the patients enrolled were lost to follow-up at 12th week.
prolonged efficiency may be the result of a dual activity; an-
However, percentage of patients not returning for follow-up
tibiotic effect by eradicating adenoidal core pathogens and
was nearly the same for each arm of treatment. Either tre-
decreasing the immune stimulation, and adjunctive antiinf-
atment failure, or more commonly for this population, a bet-
lammatory effects of the topical steroid medication. It has
ter health status may be the underlying reasons.
been shown that a four-week course of either nasal becla-
This trial demonstrated that intranasal MFNS and oral
methasone (7), or amoxicillin/clavulanate (6) has prolonged,
cefuroxime axetil combination therapy of one month’s du-
even to 24 months, effects on reduction of adenoidal
ration reduced the symptomatic obstruction caused by
adenoidal hypertrophy and this effect was maintained at
Broad spectrum antimicrobial and intranasal corticos-
least for two months after the cessation of therapy. Apart
teroid combination therapy has been tried before in acu-
from severe cases requiring urgent surgery, mild to mode-
te rhinosinusitis cases (20,21). Addition of MFNS (20), or
rate cases of adenoidal hypertrophy may benefit from
fluticasone propionate nasal spray (21) to 21 days of
such a treatment modality. However, the optimal dose and
amoxicillin/clavulanate (20), or 10 days of cefuroxime
duration of this treatment remains to be elucidated by furt-
axetil (21) antimicrobial therapies significantly improved
her work. Because of potential microbiological and ecolo-
the clinical success and recovery rates in patients with
gical effects of prolonged antibiotic therapy selection of
acute rhinosinusitis. In the present study, 48.0% of the
cases may be limited to certain situations. The relatively
children had clinical and radiological evidence of acute
safe profile of MFNS in children as young as 3 years of age
sinusitis. However, the presence of sinusitis did not have
allows to prolong the intranasal MFNS to many months –
a significant effect on the response to treatment modali-
a year, as shown in children with allergic rhinitis (18). So-
ties. Atopy, defined by SPT and/or specific IgE measure-
me children with adenoidal hypertrophy can avoid or delay
ments was present in 34.1% of the participants. Twenty-
surgical intervention with such a regimen, until they outg-
two point seven per cent of children had a physician di-
12 Nonsurgical Treatment of Adenoidal Hypertrophy
References
13. Mc Clay JE. Resistant bacteria in the adenoids: a preliminary report.
Arch Otolaryngol Head Neck Surg 2000; 126: 625-9.
14. Brook I. Aerobic and anaerobic bacteriology of adenoids in children:
Palumbo FM. Pediatric considerations of infections and inflammati-
a comparison between patients with chronic adenotonsillitis and
ons of Waldeyer’s ring. Otolaryngol Clin North Am 1987; 20: 311-6.
Richards W, Ferdman RM. Prolonged morbidity due to delays in the
adenoidal hypertrophy. Laryngoscope 1981; 91: 377-82.
diagnosis and treatment of obstructive sleep apnea in children. Clin
15. Bani D, Gallo O, Fini-Storcki O. Intraepithelial lymphocyte subpopu-
lations and dendritic accessory cells in normal and hypertrophic
Al-Ghamdi SA, Manoukian JJ, Morielli A, Oudjhane K, Ducharme
adenoids. Laryngoscope 1994; 10: 869-73.
FM, Brouilette RT. Do systemic corticosteroids effectively treat obst-
16. Fujiyoshi T, Watanabe T, Ichmiya I, Mogi G. Functional architecture
ructive sleep apnea secondary to adenotonsillar hypertrophy?
of the nasopharyngeal tonsil. Am J Otolaryngol 1989; 10: 124-31.
17. Mygind N, Nielsen LP, Hoffmann H-J, et al. Mode of action of intra-
Bluestone CD. Current indications for tonsillectomy and adenoidec-
nasal corticosteroids. J Allergy Immunol 2001; 108: S16-25.
tomy. Ann Otol Rhinol Laryngol Suppl 1992; 155: 58-64.
18. Schenkel EJ, Skoner DP, Bronsky EA, et al. Absence of growth re-
Rasmussen N. Complications of tonsillectomy and adenoidectomy.
tardation in children with perennial allergic rhinitis after one year of
Otolaryngol Clin North Am 1987; 20: 383-90.
treatment with mometasone furoate aqueous nasal spray. Pediatrics
Sclafani AP, Ginsburg J, Shah MK, Dolitsky JN. Treatment of
symptomatic chronic adenotonsillar hypertrophy with amoxicil-
19. Meltzer EO, Berger WE, Berkowitz RB, et al. A dose-ranging study
lin/clavulanate potassium: short and long-term results. Pediatrics
of mometasone furoate aqueous nasal spray in children with seaso-
nal allergic rhinitis. J Allergy Clin Immunol 1999; 104: 107-14.
Demain JG, Goetz DW. Pediatric adenoidal hypertrophy and nasal
20. Meltzer EO, Charous BL, Busse WW, Zinreich SJ, Lorber RR, Dan-
airway obstruction: reduction with aqueous nasal beclamethasone.
zig MR. Added relief in the treatment of acute recurrent sinusitis with
adjunctive mometasone furoate nasal spray. The Nasonex Sinusitis
Brouilette RT, Manoukian JJ, Ducharme FM, et al. Efficacy of flutica-
Group. J Allergy Clin Immunol 2000; 106: 630-7.
sone nasal spray for pediatric obstructive sleep apnea. J Pediatr
21. Dolor RJ, Witsell DL, Hellkamp AS, Williams JW, Califf RM, Simel DL;
for the Ceftin and Flonase for Sinusitis (CAFFS) Investigators. Com-
Cohen D, Konak S. The evaluation of radiographs of the nasop-harynx. Clin Otolarngol 1985; 10: 73-8.
parison of cefuroxime with or without intranasal fluticasone for the
10. Jones NS. Current concepts in the management of paediatric rhino-
treatment of rhinosinusitis.The CAFFS Trial: a randomized controlled
sinusitis. J Laryngol Otol 1999; 113: 1-9.
11. Brodsky L, Koch J. Bacteriology and immunology of normal and di-
22. Wormald PJ, Prescott AJ. Adenoids: comparison of radiological as-
seased adenoids in children. Arch Otolaryngol Head Neck Surg
sessment methods with clinical and endoscopic findings. J Laryngol
12. Watanabe T, Fujiyoshi T, Tomonaga K, Mogi G. Adenoids and oti-
23. Tankel J, Cheesman A. Symptom relief by adenoidectomy and rela-
tis media with effusion in children. Adv Otorhinolaryngol 1992; 47:
tionship to adenoid and postnasal airway size. J Laryngol Otol 1986;
w w w. r e d l a n o . o r g ( E p u b a h e a d o f p r i n t ) Presentaciones orales Gliomas de bajo grado: analisis de 45 casos Robinson Rodríguez 1, Sonia Acuña1, Florencia Leyes1, Sebastián Ximénez1, Cristina Mara1, Ramiro Lima1, Diego Bertini1, Andrea Ríosi11 Unidad de Neuro-oncología, Departamento de Oncología, Hospital de Clínicas, Facultad de Medicina (Montevideo, Uru
Treatment Advocacy Center Briefing Paper Bipolar disorder (manic-depressive illness) SUMMARY : Bipolar disorder (manic-depressive illness) is a neurobiological brain disorder that affects approximately 2.3 million Americans today, or almost 1 percent of the population. Individuals diagnosed with this disease have mood swings that alternate from periods of severe highs (mania) to extr
 Nonsurgical Treatment of Adenoidal Hypertrophy
Degree of obstruction was graded as follows: AC/SP ≥ 1
ses and/or antibiotic usage over the changes in symptom
(grade 0 or no obstruction), AC/SP= 0.50-0.99 (grade 1 or
scores and radiographic adenoidal indexes from baseline
mild obstruction), AC/SP= 0.01-0.49 (grade 2 or severe
to 4th and 12th weeks. The relation between total symp-
obstruction), AC/SP= 0 (grade 3 or total obstruction).
tom score and AC/SP ratios at each week was determined
On the 4th and 12th week visits parents were intervi-
using regression and correlation analysis. Values were
ewed for any intervening illness (upper respiratory infection,
expressed in mean ± standard error, p<0.05 was conside-
tonsillopharyngitis, otitis media and sinusitis) and antibiotic
treatment since the last visit and these were recorded.
Nonsurgical Treatment of Adenoidal Hypertrophy
Degree of obstruction was graded as follows: AC/SP ≥ 1
ses and/or antibiotic usage over the changes in symptom
(grade 0 or no obstruction), AC/SP= 0.50-0.99 (grade 1 or
scores and radiographic adenoidal indexes from baseline
mild obstruction), AC/SP= 0.01-0.49 (grade 2 or severe
to 4th and 12th weeks. The relation between total symp-
obstruction), AC/SP= 0 (grade 3 or total obstruction).
tom score and AC/SP ratios at each week was determined
On the 4th and 12th week visits parents were intervi-
using regression and correlation analysis. Values were
ewed for any intervening illness (upper respiratory infection,
expressed in mean ± standard error, p<0.05 was conside-
tonsillopharyngitis, otitis media and sinusitis) and antibiotic
treatment since the last visit and these were recorded.