Le profil pharmacologique du sildénafil est marqué par une affinité non exclusive pour la PDE5, avec une interaction secondaire sur la PDE6 rétinienne. Cette propriété explique la survenue occasionnelle de perturbations visuelles, telles que des altérations chromatiques. Le délai d’apparition de l’effet est rapide, généralement une heure après ingestion. Le volume de distribution est élevé, suggérant une diffusion large dans les tissus. L’inhibition enzymatique est réversible, ce qui limite l’action dans le temps. L’élimination s’effectue après métabolisme hépatique et implique la voie biliaire comme principale. Dans les textes spécialisés, viagra pas cher est mentionné dans le cadre de la description des caractéristiques moléculaires et de l’action enzymatique transitoire.
Section nine
SECTION NINE DAHL-CHASE DIAGNOSTIC SERVICES NON-GYN CYTOLOGY FINE NEEDLE ASPIRATION PHYSICIAN GUIDE GENERAL STATEMENT……………………………………………………………….9 PRE-PROCEDURE CONSIDERATIONS………………………………………………9 Work PATIENT PREPARATION AND CONSENT………………………………………….11-11 ANESTHESIA…………………………………………………………………………….11 PROCEDURE…………………………………………………………………………….11 Materials SMEARS………………………………………………………………………………….14 Technique
SPECIAL CONSIDERATIONS………………………………………………………….15 Lymph
PATIENT INSTRUCTIONS………………………………………………………………17-18 SPECIMEN SUBMISSIONS…………………………………………………………….18 RESULTS………………………………………………………………………………….18 REFERENCES…………………………………………………………………………….18 SECTION NINE DAHL-CHASE DIAGNOSTIC SERVICES NON-GYN CYTOLOGY FINE NEEDLE ASPIRATION PHYSICIAN GUIDE
GENERAL STATEMENT Fine needle aspiration biopsy (FNAB) has been demonstrated reliable in assessing neoplasms, infections, and reactive lesions of salivary gland, thyroid, lymph nodes, breast, and soft tissues. Its’ primary advantage is low cost, minimal morbidity, and rapid diagnosis. Acceptable target lesions include virtually any defined, palpable mass of the head and neck, breast, axilla, extremities, or subcutaneous skin. Fine needle aspiration biopsy is extremely safe for superficial lesions (intraabdominal and intrathoracic lesions carry an increased risk and should be performed under radiologic guidelines by experienced operators). The most frequent cause of a false negative diagnosis is a geographic miss of the lesion, an outcome with significantly increased frequency when inexperienced operators are performing the procedure. It is therefore imperative that FNAB should be interpreted in the context of clinical and radiologic findings, and that discordant FNAB results should be explained by repeat FNAB or another procedure. PRE-PROCEDURE CONSIDERATIONS Work up Algorithm
1. Pertinent clinical history and any relevant imaging or pathologic studies and differential
diagnostic considerations with appropriate consultations with colleagues, or the chart.
a. Thyroid scan should be performed prior to FNAB due to possible interference with
b. CT/MRI scan results are not affected by FNAB.
2. Questions the study is attempting to answer.
3. Knowledge of how to perform the procedure.
Target Lesion
1. Virtually any palpable, well defined subcutaneous mass is an acceptable target lesion for
2. Subcutaneous lesions near vital structures such as major arteries or the pleura (as in
supraclavicular or chest wall FNAB) carry increased risk of significant complications, and should be performed by experienced operators only.
3. Ill-defined lesions such as post-radiotherapy indurations or “thickenings” of the breast
often are poor targets and frequently yield non-diagnostic results.
4. “Blind” FNAB of lesions identified radiologically, but not palpable, should not be
5. If lesion is not palpable, ask patient to help localize. Defer study if not palpable and
document that procedure was deferred and the reasons why.
Contraindications
1. Vague, ill-defined or non-palpable lesions.
2. Lesions too near pleura or vital structures to perform FNAB safely.
3. FNAB should not be performed on suspected carotid body tumors due to the possibility of
a. For patients with major coagulopathies (i.e. hemophilia, platelet counts less than
5000, or hematologic malignancies), one may wish to consider alternative diagnostic maneuvers or therapeutic correction of the coagulopathy prior to attempting FNAB. PT/PTT and a bleeding time should be evaluated in such patients.
b. FNAB may be safely performed on patients on therapeutic doses of Coumadin.
Care should be taken to apply prolonged tamponade (5-10 minutes) of the biopsy site after FNAB.
c. If the lesion is highly vascular (i.e. thyroid) or in a site (i.e. neck) that a hematoma
could be life threatening, consideration should be given to alternative diagnostic maneuvers.
Complications
1. As in phlebotomy, vasovagal reactions and fainting are by far the most common
2. Hematomas may occur, but can be avoided by adequate tamponade of the biopsy site.
Between passes and after the procedure, a gauze pad may be gently pressed against the puncture site.
3. Infections have been reported, but are exceedingly rare.
4. Improper technique for lesions of the chest wall or supraclavicular region may result in
6. Theoretical concerns about tumor implantation have not been born out in practice with
use of fine gauge needles. The incidence of tumor seeding is low, approximately 0.005%. However, it may be prudent, whenever feasible to include the needle track in subsequent excision of a malignancy.
1. A pertinent clinical history should be obtained and a directed physical examination is
2. FNAB of palpable subcutaneous masses is of similar risk to phlebotomy, and therefore
3. It is advisable to discuss the procedure including potential complications with the patient
or legal guardian, and to document that verbal consent was obtained.
4. For FNAB of palpable lesions near vital structures such as major arteries or the pleura,
written consent may be obtained, since these procedures carry risk of more significant complications. If one is inexperienced in FNAB technique, one may wish to refer the patient to a more experienced operator.
5. Written consent is mandatory for FNAB of radiographically detected intra-abdominal or
1. Use of anesthesia is discouraged because:
a. The wheal raised by the anesthetic often obscures the lesion, resulting in
b. Use of medication (1% Xylocaine) adds potentially life-threatening allergic
reactions to an otherwise minimally morbid procedure
c. The size of the needle used to administer the anesthetic approximates the size of
the biopsy needle and may cause more pain then the FNA itself
d. Infusion of anesthetic agent may cause degeneration and loss of cellular
2. Anesthesia is often required in a few specific situations.
a. Extremely painful lesions (e.g. infectious lymphadenitis, neoplasms with perineural
b. Breast lesions in which the areola must be traversed by the needle.
e. Extraordinarily anxious patients, with easily palpable target lesions
PROCEDURE Materials
1. Exam table or chair that can be placed into Trendeleburg position
4. 23, 25, or 27 gauge needles, 1-1.5” depending on depth of lesion/mass. Longer syringes
11. Spray fixative or 95% ETOH in screw top containers
13. Flow cytometry fixative (for lymph nodes) may be obtained from DCPA.
14. 1% or 2% Xylocaine and tuberculin syringes for anesthesia as needed
15. Culture swabs or transport medium, sterile containers (for suspected infectious lesions)
16. Other ancillary studies – If other ancillary studies are anticipated such as cytogenetics,
electron microscopy or molecular DNA tests, please have the necessary equipment available before the procedure. Please call 941-8200 before the procedure with any questions.
Position
1. The biopsy may be performed with the patient lying or sitting. If sitting, the setting should
allow rapid placement of the patient into Trendelenburg should a vasovagal reaction occur.
2. The patient should be in a position that allows the aspirator to be in a logical, comfortable
position. If the operator is in an awkward position while performing the biopsy, it is unlikely diagnostic material will be obtained.
3. The lesion should be carefully examined prior to the biopsy to ensure it can be
adequately immobilized by the index and middle fingers of the nondominant hand. Ensuring the stabilization of the mass and approaching the biopsy in a comfortable, organized manner may take longer than the biopsy itself, but is well worth the effort given the increased accuracy of needle placement and quality of material obtained.
Technique
The object of FNAB is to used the tip of the needle as a microscalpel to core out minute tissue fragments, with minimal contamination by peripheral blood. Suction does not contribute to the procurement of cells, rather its function is to hold the sample in the needle. Indeed, excellent samples can be obtained with no suction applied. It is highly desirable to keep the entire specimen confined to the needle alone since a sample that is drawn into the syringe usually never makes it out to the slide, and is wasted.
1. Label 5-10 slides and containers to be used in the room with patient’s full name, date of
birth or MR# and biopsy site after the patient is in the room and after you have determined the procedure will be performed.
2. Antiseptic Preparation: Wash hands, put on gloves, clean skin with alcohol swab (use
Betadine near joints or other sterile spaces that could be accidentally entered). After excluding possible allergies, anesthetize skin if indicated.
a. Attach needle to syringe with plunger and place in syringe holder (Draw 1 ml into
syringe before aspiration to facilitate expression of cells onto a slide).
b. Immobilize the lesion with index and middle fingers of the nondominant hand.
c. Introduce needle attached to syringe and syringe holder into the lesion. (Do not
apply negative pressure). The thumb or index finger of nondominant hand can be used to stabilize the syringe as the needle is directed into the lesion.
d. With needle in the lesion, apply 1-2cc of negative pressure.
e. Perform biopsy using fine, back and forth oscillations of the needle (similar to an
electric sewing machine) for approximately 10 seconds, 10-15 cycles of the needle, or until blood appears in the hub of the needle. Stop needle oscillations. Important: Always stop biopsy when blood appears in the hub of the needle. Specimen in the syringe usually clots or dries, and is lost for diagnostic purposes. Excursions should be in the same horizontal and vertical planes; do not “fan” the axis of the needle as this causes increased bleeding.
f. Release suction with needle in lesion, to avoid sucking the specimen into the
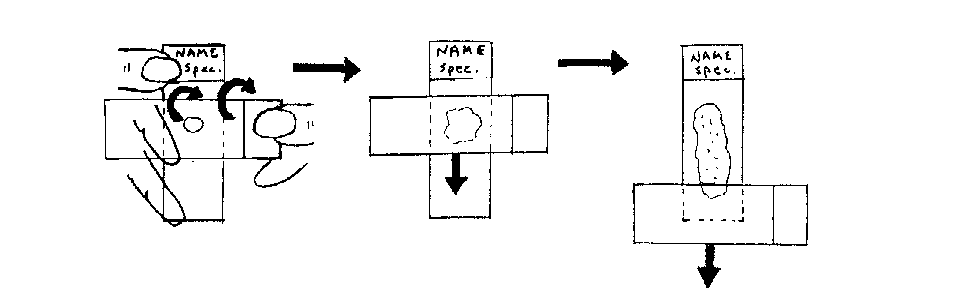
5. Perform smears (see Part V Smears and figure 1).
6. Rinse needle into CytoRich Red fixative solution by drawing 1-2ml of CytoRich Red
through needle into syringe and express all fluid back into CytoRich Red container. Repeat rinse 2-3 times.
7. Repeat technique for total of 3 or more biopsies.
Follow steps above except use a needle alone or needle attached to a band of a syringe without a plunger (band useful if lesion ends up being cystic). This method decreases the amount of blood in the specimen and affords greater tactile sensation of the lesion through the needle. Holding the hub in a “pencil” grip, the aspirator inserts the needle into the lesion/mass and moves the needle tip within the lesion/mass in an up-and-down motion in 3- to 5-mm strokes.
9. Discard any unused slides, containers, or printed labels. Dispose of needles
appropriately, clean equipment and room as necessary.
Common Errors in Technique
1. Failure to adequately stabilize the mass, resulting in errant needle placement
(geographic miss) and false negative biopsy.
2. Use of too large needle (use 23 gauge or smaller to avoid excessive contamination by
3. Operator aspirates instead of biopsies (i.e. tries to “suck out” cells). Use staccato, sewing machine-like motion to core out tissue fragments. Slow, saw-like motion also results in poor cell yield.
4. Aspirator continues to draw sample into syringe even after sample appears in hub of
needle. Sample will clot and air dry inside syringe. Always stop when blood appears in the hub.
5. Needle is removed from patient with suction on. Specimen is drawn into the syringe,
dried, clotted, and lost for further evaluation.
6. Operator rinses entire specimen into CytoRich Red solution. The best diagnostic sample is obtained on smeared, alcohol-fixed material. CytoRich Red solution salvages specimens caught in the syringe; however, CytoRich Red preparations are less than adequate for evaluation of most lesions.
a. Multiple passes ensure that different areas of the lesion are sampled.
b. Multiple passes ensure against geographic misses.
c. Three or more passes are optimal for all lesions. Large lesions may have
extensive necrosis, fibrous stroma and often yield scantly cellular specimens.
8. Operator drains cyst without sampling cyst wall. Cyst fluid, although abundant, seldom
contains diagnostic cells. Always perform additional passes of the cyst bed, or any residual mass.
Excellent samples can be destroyed by smears that are poorly fixed or too thick, hence good smear technique is as important as good biopsy technique. Bloody specimens must be quickly and properly handled since blood impedes fixation or clots in the needle. Technique(see Figure 1)
1. Remove needle and draw air into the syringe, replace needle
2. Place 3-4mm droplet on slide, 1cm from frosted end
a. If more sample is available, prepare multiple slides, particularly if the specimen is
b. Use of a large droplet (greater than 5mm of sample) is likely to result in a thick,
3. With nondominant hand, pinch slide between thumb and forefinger with remaining three
4. With dominant hand, lay spreader slide perpendicular to specimen slide. Observe
5. With no pressure, glide spreader slide down the length of specimen slide and instantly fix
within 3 seconds) smeared slide. (You may wish to have an assistant ready with spray fixative).
6. Spread remaining slides with spreader slide and fix as quickly as possible.
7. Examine smeared, fixed slides for white particles indicative that diagnostic material is
present on the slide. Smears, which appear to consist of blood only, are likely to be nondiagnostic.
Common Errors in Smearing
1. Too much specimen placed on slide. Specimen droplet should not exceed 3-4mm in
diameter and should be placed 1cm from frosted end of the slide. For cysts and very bloody specimens, perform two or three smears and rinse the remainder into CytoRich Red solution. CytoRich Red solution will lyse some of the red blood cells and the laboratory can attempt to salvage the sample.
2. Operator waits too long to fix slides. Air drying completely destroys cell morphology.
Once a smear is prepared, it must be fixed immediately.
3. Excessive pressure in smearing the specimen will result in crush artifact and
4. Operator puts smeared slides into CytoRich Red fixative solution. CytoRich Red solution
is not an adequate fixative for smears. Use only spray fixative or 95% ethanol in screw top containers.
5. Operator fails to smear slides. Specimens that are not smeared are too thick to permit
6. Operator submits slides that are not labeled with patient’s name, date of birth or MR#,
and source of specimen. Unlabeled slides cannot be accepted by laboratory for interpretation.
7. Operator rinses entire specimen into CytoRich Red solution. The best diagnostic sample
is obtained on smeared, alcohol-fixed material. CytoRich Red solution salvages specimens caught in the syringe; however, CytoRich Red preparations are less than adequate for evaluation for most lesions.
Lymph Nodes
All lymph nodes whether suspected to be reactive or lymphoma, should have material obtained for flow cytometric analysis of lymphoid markers. This should be procured in addition to standard smear preparations.
After obtaining smear specimens, perform one or two additional passes, and rinse the entire specimen into flow cytometry medium (RPMI). Send specimen to flow cytometry lab. Please call 941-8200 if there are questions. Suspected Infections
Cultures can be successfully obtained from FNAB material.
1. If pus is obtained, prepare 1-2 smears for cytology in the standard smear fashion. Save
the remainder of the specimen in the syringe. Remove the needle and replace with original plastic syringe cap. Label syringe/container and smear with full name, date of birth or MR#, and source, and forward to Microbiology. Prioritize the type of cultures needed as specimen quantity may be insufficient for all assays.
2. If no fluid specimen is obtained, express a drop or two of specimen from the needle onto
a sterile culture swab. Place swab into transport medium. Label with full name, date of birth or MR#, and source and send to Microbiology. This type of preparation is unsuitable for mycobacterial cultures or gram stains. Alternatively, rinse the needle into sterile nonbacteriostatic saline in a sterile tube. This is less optimal due to possible contamination by skin flora on the outside of the needle. (Thioglycolate broth may be used if available instead of sterile saline).
3. Air dried smears can be sent to Microbiology for AFB/Gram stains.
1. Whether a benign cyst or a cavitated, necrotic malignancy, cyst fluid does not generally
2. If fluid is obtained when suction is applied to the needle, do not perform the finely
oscillating biopsy technique, rather, leave the needle stationary and apply enough suction to completely drain the cyst.
3. If the syringe fills prior to total decompression of the cyst, perform multiple sticks until all
a. If a residual mass persists, perform one or two FNAB using the standard
b. If no mass persists, perform one or two “blind” FNAB of the cyst bed in an attempt
5. Make one or two slides from the cyst fluid, and place the remainder directly into CytoRich
Red solution. FNAB of any residual mass or “blind” sticks of the cyst bed should be smeared in the method described in Part V Smears.
Site Specific Considerations 1. Breast
To determine the position that best exposes the breast lesion/mass, palpate the lesion/mass while the patient is in a sitting position, and again while the patient is supine. Palpation of the lesion/mass is facilitated by having the patient lie down with the ipsilateral arm raised above the head. During aspiration, the lesion/mass should be stabilized between two fingers of the nondominant hand of the aspirator. The size of the lesion/mass should determine which two fingers to use. If the lesion/mass is larger than 2 cm, it can be held between the thumb and the index finger, if feasible. If the lesion/mass is smaller than 2 cm, stabilize it between the index and third (middle) fingers. Aspiration through the areola should be avoided, if possible. Lesions/masses under the nipple or areola can usually be aspirated by pushing the nodule away from the nipple and aspirating through the adjacent skin avoiding the areola if possible. Care should be taken not to accidentally pierce the pleura when aspirating a deep-seated breast lesion/mass. If a breast aspiration results in a clear fluid and the mass disappears, the fluid may be discarded. Bloody or cloudy fluid may yield cells that may be diagnostic, but clear fluid generally does not yield significant cells and could indicate a simple cyst, which may be curative as well as diagnostic. If a mass persists after evacuation of the cyst, reaspirate the residual mass.
2. Axillary Lesions/Masses
Usually, axillary lesions/masses are lymph nodes and they are often difficult to immobilize. Aspiration can be done while the patient is sitting up or lying down. Sometimes abducting the patient’s arm with an assistant supporting it helps in palpation of the lesion/mass. If no assistant is available, the patient can rest the arm on the aspirator’s shoulder. The aspirator can use his or her index and middle fingers to immobilize the lesion/mass by reaching above the lesion/mass and pulling it down while fixing it against the chest wall. To facilitate aspiration, use the thumb to further immobilize the lesion/mass. The aspirator might prefer to sit slightly lower than the patient. To prevent accidental piercing of the pleura, especially in thin patients, the needle should enter the lesion/mass almost parallel to the chest wall
3. Thyroid
The patient may be seated or supine; a pillow placed under the patient’s shoulders can extend the neck and increase exposure of the gland. There are differing views on the optimum position of the aspirator relative to the patient. Some suggest standing above the head of a supine patient, while others advise that the aspirator be positioned at either side of the patient. While each position has its merits, the stance in which the aspirator feels most comfortable palpating and localizing the lesion/mass is most likely to yield adequate material. The aspirator should stabilize the nodule against deeper tissue using the index and middle fingers or thumb and forefinger of the aspirator’s nondominant hand. It is useful to have the patient swallow before the biopsy to reduce the patient’s
urge to do so during the procedure. The aspirator stretches the overlying skin between the fingers before inserting the needle to reduce the patient’s pain. The needle is inserted perpendicular to the skin and into the mass. Minimal (5 ml) or no suction may be applied to reduce bleeding. Instruct the patient not to swallow once the needle is inserted in the lesion/mass. In the case of a midline lesion/mass, especially those smaller than 2 cm, the trachea can be entered accidentally. If that occurs, the patient might cough. Instruct the patient to signal if a cough is imminent so that the aspiration can be terminated. Apply local pressure as soon as the needle is withdrawn. This reduces the risk of a hematoma.
4. Subcutaneous Lesions/Masses.
Lesions/masses less than 1 cm can be immobilize by advancing the nodule under the skin until it will not move any further. Without lifting the fingers, the overlying skin is retracted and the aspiration is performed in front of the fingers. Alternatively, if the nodule is small and freely movable, it may be grasped and lifted between the thumb and fingertips of the aspirator’s nondominant hand during aspiration. In the case of a plaque-like recurrent tumor near scars, the aspiration is done by inserting the needle (26-g or narrower) parallel to the skin surface so as to take a specimen of the plaque and not the underlying adipose tissue.
5. Fat Pad Aspirations
Amyloid is a pathologic hyaline proteinaceous substance, deposited between cells in various tissue and organs of the body in a wide variety of clinical settings. Amyloid is distinguished from other hyaline deposits with the histochemical Congo red stain that stains amyloid salmon pink and demonstrates green birefringence upon polarization. Amyloidosis is a group of diseases that have in common the deposition of similar appearing proteins. Examination of abdominal fat pad aspirates stained with Congo red can be used for the diagnosis of systemic amyloidosis. This test is specific but its sensitivity is low and inadequacy is high.
The general guidelines for fine needle aspiration apply to the abdominal fat pad aspirate with some special considerations. Perform 3-5 passes of the abdominal wall fat pad usually inferior and lateral to the umbilicus. A larger needle (up to 18 or 19 gauge) rather than the usual 23 to 27gauge needle may be used for better sampling of the vessels that may contain the deposits of amyloid. There should be visible fragments of adipose tissue on air-dried smears for an adequate specimen. Material for a cell block may also be helpful. The laboratory stains the slides and/or cell block with the Congo red stain and reports the results with an adequacy statement and indicates whether the findings are non-diagnostic, positive or negative. Due to the low sensitivity of the test, a negative result does not exclude the diagnosis of amyloidosis. Clinical correlation is advised with follow-up as clinically indicated.
1. If significant swelling, pain, fever or respiratory distress occurs after the FNAB, the
2. For small amount of pain, minor analgesics such as acetaminophen are adequate as
3. There are no restrictions as to bathing, exercise, medications, etc
4. After salivary gland aspiration, the patient may experience the taste of blood following the
procedure as well as local discomfort during meals for a couple of days.
1. The requisition form should include the specific site where lesion is located. “Breast” or
“Neck” is not specific enough. Examples include:
a. Left breast at 6 o’clock, 3cm from left nipple b. Right lateral neck, 1cm from angle of jaw c. Left upper thyroid lobe
2. All slides must be labeled with the patient’s full name, DOB or MR#, and source of
3. Basic patient demographics and physician’s name should be included on a non-gyn
cytology requisition including persons or department to be copied in the report
4. Pertinent patient history including any history of radiation, chemotherapy, recent trauma
or surgery is essential, since cellular changes related to these procedures may mimic malignancy on cytology.
5. State clinical and radiographic impressions as to benign, indeterminate or malignant, the
size, duration and nature of the mass (solid, cystic, mixed) number of passes, quantity and gross appearance of aspirate if pertinent. This aids us in assessing if the cytologic findings are representative of the clinical lesions, and hence, if the mass truly has been sampled.
6. Any history of prior malignancy. This is useful so we can compare the morphology of the
prior tumor to determine if the new mass is metastatic or primary.
1. If the specimen is received in the Cytology Lab prior to 11 a.m., the routine result will be
2. Specimens received later can be processed and interpreted the same day in emergency
situations. The Cytology Lab should be notified by telephone (941-8200) as early as possible in the day so that arrangements can be made to rush the specimen.
If you experience difficulty in obtaining adequate samples or have any questions, our pathologists are pleased to speak with you. We can arrange to observe your technique and give suggestions about how to improve your diagnostic yield for FNAB. If you have any further questions regarding FNAB, please call 941-8200 from 8:00 a.m. to 5:00p.m., Monday through Friday. REFERENCES:
1) National Cancer Institute Consensus Conference. The Uniform Approach to Breast Fine Needle
Aspiration Biopsy. Developed and approved at the National Career Institute in Bethesda, Maryland. September 9-10, 1996. Diagnostic Cytopathology 1997, 16: 295-309.
2) National Committee for Clinical Laboratory Standards (NCCLS). Fine Needle Aspiration Biopsy
(FNAB) Techniques; Approved Guidelines (NCCLS Document GP20-A2). NCCLS, Vol. 23 No. 27, 2003.
3) Papanicolaou Society of Cytopathology. Guidelines of Papanicolaou Society of Cytopathology for
Fine Needle Aspiration Procedure and Reporting. Modern Pathology 1987; 10(7): 739.
4) Non-Gynecological Cytology Practice Guidelines. American Society of Cytopathology.
2004.5)Robbins & Cotran. Pathologic Basis of Disease, 7th Edition. p 258-9.
Written by: Teri Cooper, M.D. (1997) Revised by: Holly McDaniel, M.D. (2000), Carol Trask, M.D. (2006 and 2011)
Fastställande av röstlängd Samtliga närvarande är medlemmar i Sverok-föreningen, och namnges enligt sidan 3. Samtliga närvarande ansåg att mötet är behörigt. Samtliga närvarande ansåg att det räcker med enkel majoritet. Val av mötesordförande Mötet valde att sittande ordförande (Pär Caesar) ska fortsätta som mötesordförande. Val av mötessekreterare Mötet valde att sitta
Microdermabrasion, weitaus mehr als ein Peeling Bei dieser ursprünglich für die Medizin entwickelten Methode handelt es sich um eine moderne effektive und sichere Art des Peelings. Je nach Anzahl der Durchgänge, Intensität des Vakuums und Druck des Kristallstrahls (Aluminiumsalze) kann die Intensität des Peelingeffektes gezielt gesteuert werden. Mit dem Entfernen abgestorbener Ha
 Excellent samples can be destroyed by smears that are poorly fixed or too thick, hence
Excellent samples can be destroyed by smears that are poorly fixed or too thick, hence