Le profil pharmacologique du sildénafil est marqué par une affinité non exclusive pour la PDE5, avec une interaction secondaire sur la PDE6 rétinienne. Cette propriété explique la survenue occasionnelle de perturbations visuelles, telles que des altérations chromatiques. Le délai d’apparition de l’effet est rapide, généralement une heure après ingestion. Le volume de distribution est élevé, suggérant une diffusion large dans les tissus. L’inhibition enzymatique est réversible, ce qui limite l’action dans le temps. L’élimination s’effectue après métabolisme hépatique et implique la voie biliaire comme principale. Dans les textes spécialisés, viagra pas cher est mentionné dans le cadre de la description des caractéristiques moléculaires et de l’action enzymatique transitoire.
Enjoi.com.hk
Intake of phenol-rich virgin olive oil improves the postprandialprothrombotic profile in hypercholesterolemic patients1–3
Juan Ruano, José Lo´pez-Miranda, Rafael de la Torre, Javier Delgado-Lista, Javier Ferna´ndez, Javier Caballero,María Isabel Covas, Yolanda Jiménez, Pablo Pérez-Martínez, Carmen Marín, Francisco Fuentes, andFrancisco Pérez-JiménezABSTRACT
concentrations have been linked to coronary heart disease (CHD)
Background: Oxidative stress associated with postprandial lipemia
(2), and both can be regulated, at least partly, by alimentary
contributes to endothelial dysfunction, which shifts hemostasis to a
lipemia (3). Attention is currently focusing on investigating
whether different components of the diet can regulate acute post-
Objective: We investigated whether a high concentration of phenols
prandial changes in coagulation and fibrinolysis.
in olive oil can partly reverse this phenomenon.
Factor VII coagulant (FVIIc) has been linked to postprandial
Design: Twenty-one hypercholesterolemic volunteers received 2
plasma triacylglycerol concentrations, which suggests an acute
breakfasts rich in olive oils with different phenolic contents (80 or
effect of triacylglycerol-rich lipoproteins (TRLs) on the activity
400 ppm) according to a randomized, sequential crossover design.
of FVII (FVIIa) (4). We previously reported that a Mediterranean
Plasma concentrations of lipid fractions, factor VII antigen
diet reduces fasting plasma concentrations of FVIIa in healthy
(FVIIag), activated factor VII (FVIIa), and plasminogen activator
men (5), a fact that might be related to the presence of olive oil in
inhibitor-1 (PAI-1) activity were measured at baseline and post-
this diet (6, 7). Williams (8) observed a reduction in postprandial
FVIIa and factor VII antigen (FVIIag) plasma concentrations
Results: Concentrations of FVIIa increased less (P ҃ 0.018) and
after the acute intake of an olive oil– based meal.
plasma PAI-1 activity decreased more (P ҃ 0.021) 2 h after the
On the other hand, it has been suggested that PAI-1 activity
high-phenol meal than after the low-phenol meal. FVIIa concentra-
declines after the intake of meals rich in oleic acid as part of a
tions 120 min after intake of the olive oil with a high phenol content
Mediterranean-type diet, in both the postprandial (9) and fasting
correlated positively with fasting plasma triacylglycerols (P ҃
states (10, 11). Virgin olive oil, which is the principal fat in this
0.001), area under the curve (AUC) of triacylglycerols (P ҃ 0.001),
dietary pattern (12), contains both oleic acid and a wide range of
and AUC of nonesterified fatty acids (P ҃ 0.024) and negatively
micronutrients, among which phenolic compounds have dis-
with hydroxytyrosol plasma concentrations at 60 min (P ҃ 0.039)
played anti-thrombotic effects in cell culture and in vitro studies
and fasting HDL-cholesterol concentrations (P ҃ 0.005). PAI-1
(13, 14). Studies in humans, however, are scarce, and more ev-
positively correlated with homeostasis model assessment of insulin
idence on these biological activities is needed (15). To further
resistance (P ҃ 0.005) and fasting triacylglycerols (P ҃ 0.025) and
investigate whether postprandial phenols from virgin olive oil
inversely with adiponectin (P ҃ 0.026). In a multivariate analysis,
affect hemostasis, we tested whether 2 breakfasts rich in this oil,
the AUCs of nonesterified fatty acids (R2 ҃ 0.467; : 0.787; SE:0.02; P 0.001) and adiponectin (R2 ҃ 0.232; : Ҁ1.594; SE:
1 From the Lipids and Atherosclerosis Research Unit, Reina Sofia Uni-
0.629; P 0.05) were the strongest predictors of plasma FVIIa and
versity Hospital, University of Cordoba, Ciber Fisiopatología Obesidad y
Nutricio´n (CB06/03), Instituto de Salud Carlos III, Spain (JR, JL-M, JD-L,
Conclusions: A virgin olive oil with a high content of phenolic
YJ, PP-M, CM, FF, and FP-J); the Pharmacology Research Unit (RdlT) and
compounds changes the postprandial hemostatic profile to a less
the Lipids and Epidemiology Cardiovascular Research Unit (MIC), Institut
Am J Clin Nutr 2007;86:341– 6.
Municipal d’Investigacio Medica (IMIM), Barcelona, Spain; the Departmentof Plant Biology, Faculty of Biology, University of Cordoba, Cordoba, Spain
KEY WORDS
Olive oil, polyphenols, postprandial lipemia,
(JF); and the Biochemical Laboratory, Reina Sofia University Hospital,
plasminogen activator inhibitor-1, PAI-1, activated factor VII,
Supported in part by research grants from the Spanish Plan for RѿD
(SAF 03/05770 to FP-J), Plan Andaluz de Investigacio´n (Consejeria deInnovacio´n, Proyectos de Investigacio´n de Excelencia AGR 05/00922 toFP-J), and the “Reina Sofía-Cajasur” Cultural Foundation. JR and JD-L are
INTRODUCTION
currently engaged in a Research Specialization Program for the Spanish
Endothelial dysfunction is one of the first steps in the devel-
3 Address reprint requests to F Pérez-Jiménez, Lipids and Atherosclerosis
opment of arteriosclerosis, and it is characterized by a thrombo-
Research Unit, Reina Sofia University Hospital, Avenue Menéndez Pidal,
genic state caused by an imbalance between procoagulant and
s/n, 14004 Cordoba, Spain. E-mail: [email protected].
profibrinolytic activity (1). Among the procoagulant factors,
plasminogen activator inhibitor-1 (PAI-1) and factor VII (FVII)
Accepted for publication April 4, 2007. Am J Clin Nutr 2007;86:341– 6. Printed in USA. 2007 American Society for Nutrition
but with different contents of phenolic compounds, had different
and were subsequently analyzed in a Jasco FP-920 spectroflu-
effects on hemostasis postprandially.
orometer (Jasco, Tokyo, Japan) at an excitation wavelength of294 nm and an emission wavelength of 340 nm. A spectropho-
SUBJECTS AND METHODS
tometer (UNICAM 5625, Cambridge, UK) was used to measuretotal carotenoid (670 nm) and chlorophyll (472 nm) contents. No
Subjects
significant differences in any of the micronutrient concentrations
Twenty-one hypercholesterolemic subjects (5 men and 16
were found, except for the polyphenol fraction.
women) aged 53 to 68 y and with a mean body mass index (in
Plasma samples
kg/m2) of 25.4 Ȁ 4.1 (range: 23.5–27.1) participated in the study. All were patients who were being followed up in the Lipids and
Samples from the fasting and postprandial states were col-
Atherosclerosis Unit at the Reina Sofía University Hospital in
lected in tubes containing 1 g EDTA/L or 3.8% citrate and were
Cordoba. Plasma total cholesterol concentrations were between
stored in containers with ice and kept in the dark. Special care was
200 and 350 mg/dL and plasma triacylglycerol concentrations
taken to avoid exposure to air, light, and ambient temperature.
were 200 mg/dL. The women were postmenopausal (but were
Plasma was separated from whole blood by low-speed centrifu-
not undergoing hormone replacement therapy). None of the par-
gation at 1500 ҂ g for 15 min at 4 °C within 1 h of extraction.
ticipants showed evidence of chronic diseases, high alcohol con-
Plasma polyphenol concentrations
sumption, or family history of early-onset cardiovascular dis-ease. None of the subjects were active smokers. The study was
Concentrations of tyrosol, hydroxytyrosol, and 3-O-methyl-
approved by the Human Investigation Review Committee at the
hydroxytyrosol (MHT), a biological metabolite of hydroxyty-
Reina Sofia University Hospital. All the participants gave their
rosol, were measured by gas chromatography–mass spectrome-
informed consent before joining the study.
try in plasma samples at 0 and 60 min (16, 17). Experimental design Lipid analysis and biochemical determinations
The participants were instructed to not take vitamins, soya
Concentrations of the different lipid variables were analyzed
supplements, or any drug treatments, including hormone treat-
with a modular autoanalyzer (DDPPII Hitachi; Roche, Basel,
ment, for the 6 wk preceding the study. Three patients were
Switzerland) with the use of Boehringer-Mannheim reagents.
taking atorvastatin, 10 mg/d, which was discontinued 6 wk be-
Concentrations of total cholesterol and triacylglycerol were mea-
fore the randomization step. The subjects were shown how to
sured by colorimetric enzymatic methods (18, 19). HDL-
follow a low-fat, carbohydrate-rich diet during that period to
cholesterol concentrations were measured by colorimetric assay
eliminate potential differences in their usual dietary habits. Com-
after the lipoproteins containing apolipoprotein (apo) B were
pliance with the stabilization diet was assessed after 2 and 4 wk
precipitated with polyethylene glycol (20). LDL-cholesterol
by means of a 3-d record and a food-frequency dietary question-
concentrations were estimated by using the Friedewald formula
naire. The participants were instructed to avoid consuming
on the basis of total cholesterol, triacylglycerol, and HDL-
polyphenol-rich foods (such as fruit or juices, wine, grape juice,
cholesterol values (21). Apo A-I and apo B concentrations were
chocolate, coffee, tea, olive oil, or soya) or performing intense
measured by immunoturbidimetry (22). The chylomicron and
physical exercise in the 24 h before the experimental breakfast.
large VLDL fractions of TRLs were isolated from 4 mL plasma
The following morning they came to the hospital after fasting for
overlayered with 0.15 mol NaCl/L, 1 mmol EDTA/L (pH 7.4;
12 h. By use of a randomized, sequential crossover design, the
density: 1.006 kg/L) by a single ultracentrifugal spin (28 000 ҂
participants were given 1 of 2 breakfasts consisting of 60 g white
g, 30 min, 4 °C) in a type 50 rotor (Beckman Instruments, Ful-
bread, 40 mL virgin olive oil (Carapelli Firenze SpA, Florence,
lerton, CA). Chylomicrons contained in the top layer were re-
Italy) with either a high (A, 400 ppm) or a low (B, 80 ppm)
moved by aspiration after the tubes were cut. The infranatant
content of phenolic compounds and 60 000 IUs vitamin A/m2
fraction was centrifuged at a density of 1.019 kg/L for 24 h at
body surface area. Patients starting with the A type breakfast
115 000 ҂ g in the same rotor. The nonchylomicron fraction of
consumed the B type after 1 wk, and conversely. Olive oil B was
TRL (also referred to as small TRL) was removed from the top of
obtained by the extraction of most of the phenolic compounds in
the tube. All operations were performed in subdued light. Large
olive oil A, so that both oils had similar contents of their remain-
and small TRL fractions were kept at Ҁ70 °C until total choles-
ing macro- and micronutrients. The procedure involved washing
terol and triacylglycerol concentrations were analyzed. Fasting
olive oil A in a separation funnel with an equal quantity of
plasma adiponectin and resistin were measured by enzyme-
double-distilled water. The mixture was shaken for 3 min and left
linked immunosorbent assay with the Quantikine Human Adi-
to settle to facilitate the separation process. The aqueous phase
ponectin/Acrp30 Immunoassay and Quantikine Human Resistin
was then discarded and the procedure repeated. The concentra-
Immunoassay (R&D Systems Inc, Minneapolis, MN). Plasma
tion of phenolic compounds was measured until it fell to trace
glucose concentrations were measured with a Hitachi 917 ana-
lyzer (Boehringer Mannheim, Mannheim, Germany) by the glu-
Throughout the 4-h duration of the study, the subjects neither
cose oxidase method (GOD-PAP). Plasma insulin concentra-
performed physical activity nor consumed anything but water.
tions were measured by microparticle enzyme immunoassay
Venous blood was drawn at 0, 30, 60, 120, and 240 min after
(Abbott Diagnostics, Matsudo-shi, Japan). Nonesterified fatty
acid concentrations were measured by enzymatic colorimetricassay (Roche Diagnostics, Penzberg, Germany). The homeosta-
Composition of the olive oils
sis model assessment of insulin resistance (HOMA-IR) was de-
Tocopherols were measured by separating the different to-
fined by the validated definition: HOMA-IR ҃ [fasting glucose
copherol isomers by means of HPLC (Beckman, Palo Alto, CA)
(mmol/L) ҂ fasting insulin (U/mL)/22.5] (23).
PHENOLS REDUCE PROTHROMBOSIS POSTPRANDIALLY
performed. A value of P 0.05 was considered to be statistically
Baseline characteristics of the hypercholesterolemic participants in the
significant. All analyses were carried out by using the statistical
software package SPSS (version 11.0; SPSS Inc, Chicago, IL). Basal and postprandial metabolic parameters
The clinical characteristics of the participants at baseline are
shown in Table 1. No significant differences were observed in
any of the incremental AUCs of the main metabolic variables
after the intake of either of the olive oils (Table 2). Basal and postprandial concentrations of tyrosol, hydroxytyrosol, and MHT 1 All values are x Ȁ SD (range in parentheses); n ҃ 21. NEFA, non-
We observed a greater increase in concentrations of plasma
esterified fatty acids; HOMA-IR, homeostasis model assessment of insulin
tyrosol, hydroxytyrosol, and MHT after the intake of the olive oil
with a high phenolic compound content than after the olive oil with a low content of phenols (Figure 1). Measurement of FVIIag, FVIIa, and PAI-1
We measured concentrations of PAI-1 in the frozen plasma
FVIIag, FVIIa, and PAI-1
samples by means of a tissue-type plasminogen activator– based
Postprandial plasma concentrations of FVIIag and FVIIa and
immunoactivity assay (Chromolize PAI-1; Trinity Biotech,
PAI-1 activity are presented in Figure 2. The intake of both olive
County Wicklow, Ireland) and concentrations of FVIIag (Asse-
oils significantly increased FVIIa activity (P ҃ 0.002) and de-
rachrom VII:Ag; Diagnostica Stago, Asnières sur Seine, France)
creased FVIIag (P ҃ 0.050) and PAI-1 activity (P ҃ 0.001) with
and FVIIa (Imubind; American Diagnostica Inc, Greenwich,
respect to baseline concentrations, which indicates a change in
CT) by enzyme-linked immunosorbent assay. All measurements
these variables during postprandial lipemia. Analysis of the in-
teraction between diet and time showed a smaller increase in
FVIIa concentration (P ҃ 0.050) and a greater decrease in PAI-1
Statistical analysis
activity (P ҃ 0.047) after the phenol-rich breakfast than after the
Duplicate values from each subject were calculated before
data analysis. Comparisons among the end values for each treat-
When we compared percentage changes from baseline values
ment period were made after adjustment for baseline values. The
in FVIIag, FVIIa, and PAI-1 values at 120 min, we found a
percentage change between concentrations at the beginning of
smaller postprandial increase in FVIIa plasma concentrations
each breakfast (basal) and concentrations 60 and 120 min after
(39.7 Ȁ 30.8% compared with 20.3 Ȁ 26.5%; P ҃ 0.018) and a
intervention with the olive oils was calculated. The area under the
greater decrease in PAI-1 plasma activity (Ҁ29.1 Ȁ 32.8% com-
curve (AUC) was defined as the area between the plasma con-
pared with Ҁ52.8 Ȁ 30.4%; P ҃ 0.021), but no significant
centration–versus–time curve and a line drawn parallel to the
differences in FVIIag, after the phenol-rich olive oil than after the
horizontal axis through the 0 h concentration. These areas
were calculated by a computer program using the trapezoidalrule. All data presented in the text and tables are expressed as
Regression analysis
means Ȁ SDs. The normality of variables was assessed by the
To further evaluate predictors of FVIIa and PAI-1, we per-
Kolmogorov-Smirnov test. The data were analyzed by analysis
formed a correlation analysis between these 2 variables and body
of variance (ANOVA) for repeated measures. Diet, time, and
mass index (BMI), metabolic variables, HOMA-IR, adiponectin,
their interaction were included in the model in addition to fasting
resistin, and plasma phenol concentrations. In a univariate cor-
concentrations as a covariate. Pearson’s linear correlation coeffi-
relation analysis, FVIIa concentrations correlated positively
cient was calculated, and a multiple linear regression analysis was
with triacylglycerol (r ҃ 0.503, P ҃ 0.001), the AUC of plasma
TABLE 2 Areas under the plasma postprandial response curves (AUCs) after the intake of the low-phenol and the phenol-rich olive oil (OO)-based breakfasts1 1 All values are x Ȁ SD; n ҃ 21. NEFAs, nonesterified fatty acids; TG, triacylglycerols; TRLs, triacylglycerol-rich lipoproteins. 2 One-factor ANOVA. FIGURE 1. Mean (ȀSD) concentrations of tyrosol, hydroxytyrosol, and 3-O-methyl-hydroxytyrosol (MHT) at baseline and 60 min after intake of a
phenol-rich olive oil breakfast (400 ppm; f) or a low-phenol olive oil breakfast (80 ppm; Ⅺ). n ҃ 21. For each panel, bars with different lowercase letters aresignificantly different from each other, P 0.05. P1: diet effect; P2: time effect; P3: diet ҂ time interaction. ANOVA for repeated-measures. Baseline valueswere used as covariants.
triacylglycerol (0.567, P ҃ 0.016), and the AUC of nonesterified
triacylglycerol-rich lipoproteins by lipoprotein lipase may be an
fatty acids (r ҃ 0.234, P ҃ 0.024) and negatively with concen-
important source of elevated concentrations of fatty acid anions
trations of hydroxytyrosol (r ҃ Ҁ0.465, P ҃ 0.039) and HDL
near the endothelium. These fatty acids are substrates for the
cholesterol (r ҃ Ҁ0.593, P ҃ 0.005). Strong direct relations were
lipoperoxidation produced by the increase in oxidative stress
found between PAI-1 activity and HOMA-IR (r ҃ 0.602, P ҃
during the postprandial period. Olive oil phenolic compounds
0.005) and triacylglycerol (r ҃ 0.487, P ҃ 0.025). PAI-1 activity
have been shown to act as chain-breaking antioxidants for the
correlated negatively with fasting adiponectin concentrations
autocatalytic chain reaction of fatty acid peroxidation (26). The
(r ҃ Ҁ0.485, P ҃ 0.026).
attenuating effect of olive oil–rich test meals on FVII was shown
To explore the importance of potential predictors, 2 stepwise
previously (6, 27), but these studies focused on the effect of
multiple linear regression models were fitted for FVIIa and
modified test meal dietary fat composition. What proportion of
PAI-1. After adjustment for HOMA-IR, fasting triacylglycerol,
this effect is due to the phenolic or fatty acid profile of virgin olive
and the AUC for triacylglycerol, only the incremental AUC of
nonesterified fatty acids remained significantly associated with
In the present study, we found a significant decrease in post-
FVIIa in the model (R2 ҃ 0.467; : 0.787; SE: 0.02; P 0.001).
prandial concentrations of FVIIag, but no significant differences
A similar strategy was used to assess the predictors of plasma
in the effects of these 2 types of olive oil. At the same time, there
PAI-1 concentrations. After adjustment for HOMA-IR, BMI,
was a smaller increase in FVIIa after the ingestion of an olive oil
and triacylglycerol, plasma adiponectin concentrations remained
with a high content of phenols than after the olive oil with a low
significantly associated with plasma PAI-1 (R2 ҃ 0.232; :
content of these compounds. Because the sole difference in the
1.594; SE: 0.629; P 0.05).
composition of these 2 oils was their phenolic content, these datasuggest that the effect of the diet on the decrease in FVIIag is due
DISCUSSION
to the difference in their fat content, and the effect on FVII
Our study showed that, in patients with hypercholesterolemia,
activation to their content of phenols.
the consumption of a breakfast containing virgin olive oil with a
How phenols interfere with this postprandial activation of
high content of phenols induces a smaller postprandial increase
FVIIa is not known. We previously showed the protective effect
in the concentration of FVIIa and a greater decrease in PAI-1
of olive oil phenols on the postprandial microvascular endothe-
plasma activity than the same olive oil with a low content of
lial function of hypercholesterolemic persons (28), an effect that
phenols. It has been suggested that the postprandial hypertriglyc-
is strongly influenced by procoagulant and prooxidant factors. It
eridemia that follows the intake of high-fat meals activates FVII.
could be hypothesized that the known antioxidant properties of
The intrinsic mechanism of this activation is not clear, although
phenols act as a potent buffer in the vicinity of endothelial cells,
it is known that some of the reactions for activation of hemostatic
thus reducing the activation of FVIIa.
factors are due to exposure to lipid bilayers with negative
We also observed a significant reduction in PAI-1 concentra-
charges, such as those of denuded endothelium or the surface of
tions 120 min after the ingestion of olive oil with a high phenolic
platelets or oxidized LDL (24). Some studies have observed that
content. Although changes in fasting PAI-1 concentrations after
FVIIa plasma concentrations correlate positively with plasma
prolonged dietary intervention periods have been described in
phospholipid concentrations (25). Our study showed a signifi-
several studies, less evidence exists of this effect of the diet in the
cant association between the incremental AUC of nonesterified
postprandial state. Furthermore, it is difficult to make a global
fatty acids and postprandial changes in FVIIa. The hydrolysis of
interpretation of the postprandial effects on PAI-1 on the basis of
PHENOLS REDUCE PROTHROMBOSIS POSTPRANDIALLY
between HOMA-IR, adiponectin, and PAI-1 were previouslyreported in both adults (40 – 42) and children (43). PAI-1 con-centrations are directly influenced by insulin (44), even in situ-ations of insulin resistance (45), a fact that has been explained interms of abdominal fat, via a higher concentration of cytokines insubjects with central obesity (41). Nevertheless, the associationof PAI-1 and insulin resistance has also been found in nonobesecohorts (46). These apparently contradictory findings may bepartially explained by the identification of a regulatory element(AP-1 response element) in the PAI-1 promoter. This elementenhances PAI-1 transcription by a factor of 7 when stimulated byinsulin increases mediated by FOX protein transcription factors(47), which may explain the association between insulin resis-tance and PAI-1. Interestingly, the same element also induces a3-fold rise in the PAI-1 transcription rate in the presence ofoxidative stress (48), as occurs in the postprandial state. Thedouble regulation of the PAI-1 promoter element may explainboth the fasting correlations between adiponectin, HOMA-IR,and PAI-1 and the larger postprandial decrease in PAI-1 after thephenol-rich breakfast as a result of its antioxidant properties and thelower activation of nuclear factor B that occurs after meals rich invirgin olive oil (49). In line with our findings, Pacheco et al (15)
recently found an enhancement in postprandial hemostasis after avery phenol-rich olive oil meal (1125 ppm of phenolic compounds),an enhancement that they evaluated in terms of a greater decrease inPAI-1, smaller tissue factor and fibrinogen AUCs, and a largerpostprandial decrease in tissue-type plasminogen activator.
The results of the present study may partly explain earlier
contradictory results of studies that tested the effects of olive oilon hemostasis. It is possible that the concentrations of micro-components of the olive oil used in some of those studies did notreach the levels needed to activate the antithrombotic properties
of olive oil. However, and although this study deals with themicrocomponents of virgin olive oil, we should still think interms of evaluating the biological properties of complete foods. In this perspective, our findings provide new evidence of thehealthy effects of virgin olive oil. In conclusion, the consumptionof a breakfast containing olive oil rich in phenolic compoundsmay improve the thrombogenic postprandial profile of FVIIa andPAI-1 concentrations associated with acute fat intake. FIGURE 2. Mean (ȀSD) acute effect on postprandial plasma factor VII
antigen (FVIIag), activated factor VII (FVIIa), and plasminogen activator
The authors express their gratitude to the “Instituto Nutrizionale Car-
inhibitor-1 (PAI-1) activity after the ingestion of a phenol-rich olive oil
apelli” (Florence, Italy), to the CEAS (Centro de Excelencia Investigadora
breakfast (400 ppm; f) or a low-phenol olive oil breakfast (80 ppm; Ⅺ). P1:
del Accite de oliva y la Salud), Jae´n, Spain; and to all of the subjects for their
diet effect; P2: time effect; P3: diet ҂ time interaction. ANOVA for repeated-
measures. Baseline values were used as covariants.
The contributions of the authors were as follows—JR, JL-M, and FP-J:
responsible for the conception and design of the study; JR, FF, CM, and YJ:
these studies because of the different designs and methods used.
responsible for the provision of study materials or subjects; JR, JL-M, JC, JF,
Both increases (3, 29) and reductions (9, 30, 31) in PAI-1 con-
FF, RdlT, MIC, and CM: responsible for the collection and assembly of data;
centrations after meals with a high fat content have been de-
JR, JL-M, JC, JF, YJ, and FP-J: responsible for the analysis and interpretation
scribed. It has even been suggested that these data might simply
of the data; JL-M, CM, FF, and FP-J: provided statistical expertise; JR, PP-M,JL-M, and FP-J: responsible for drafting the manuscript; JD-L, RdlT, MIC,
be the result of a circadian variation in PAI-1 concentrations,
JL-M, and FP-J: responsible for the critical review of the manuscript and for
without any direct relation to diet (32, 33). Nor is there a clear
important intellectual content; FP-J: obtained funding. None of the authors
explanation of the mechanism by which PAI-1 concentrations
had any personal or financial conflicts of interest.
would be influenced by the acute intake of different amounts offat, although it has been suggested that VLDL could up-regulatePAI-1 transcription (34 –36), something that can be avoided by
REFERENCES
1. Nossel HL. Relative proteolysis of the fibrinogen B beta chain by throm-
In our study, PAI-1 activity showed a greater postprandial
bin and plasmin as a determinant of thrombosis. Nature 1981;291:165–7.
2. Smith A, Patterson C, Yarnell J, Rumley A, Ben-Shlomo Y, Lowe G.
decrease after the intake of the olive oil with high phenolic
Which hemostatic markers add to the predictive value of conventional
content, whereas it correlated negatively with fasting adiponec-
risk factors for coronary heart disease and ischemic stroke? The Caer-
tin concentrations and positively with HOMA-IR. Correlations
philly Study. Circulation 2005;112:3080 –7.
3. Byrne CD, Wareham NJ, Martensz ND, Humphries SE, Metcalfe JC,
27. Roche HM, Zampelas A, Knapper JM, et al. Effect of long-term olive oil
Grainger DJ. Increased PAI activity and PAI-1 antigen occurring with an
dietary intervention on postprandial triacylglycerol and factor VII me-
oral fat load: associations with PAI-1 genotype and plasma active TGF-
tabolism. Am J Clin Nutr 1998;68:552– 60.
beta levels. Atherosclerosis 1998;140:45–53.
28. Ruano J, Lopez-Miranda J, Fuentes F, et al. Phenolic content of virgin
4. Miller GJ, Martin JC, Mitropoulos KA, et al. Plasma factor VII is acti-
olive oil improves ischemic reactive hyperemia in hypercholesterolemic
vated by postprandial triglyceridaemia, irrespective of dietary fat com-
patients. J Am Coll Cardiol 2005;46:1864 – 8.
position. Atherosclerosis 1991;86:163–71.
29. Kozima Y, Urano T, Serizawa K, Takada Y, Takada A. Impaired fi-
5. Gomez P, Fernandez de la Puebla RA, Castro P, et al. [Effect of the
brinolytic activity induced by ingestion of butter: effect of increased
Mediterranean diet on fasting concentrations of activated factor VII in
plasma lipids on the fibrinolytic activity. Thromb Res 1993;70:191–202.
healthy persons. ] Rev Esp Cardiol 2005;58:285–9 (in Spanish).
30. Tholstrup T, Miller GJ, Bysted A, Sandstrom B. Effect of individual dietary
6. Larsen LF, Jespersen J, Marckmann P. Are olive oil diets antithrom-
fatty acids on postprandial activation of blood coagulation factor VII and
botic? Diets enriched with olive, rapeseed, or sunflower oil affect post-
fibrinolysis in healthy young men. Am J Clin Nutr 2003;77:1125–32.
prandial factor VII differently. Am J Clin Nutr 1999;70:976 – 82.
31. Salomaa V, Rasi V, Pekkanen J, et al. The effects of saturated fat and
7. Allman-Farinelli MA, Gomes K, Favaloro EJ, Petocz P. A diet rich in
nҀ6 polyunsaturated fat on postprandial lipemia and hemostatic activ-
high-oleic-acid sunflower oil favorably alters low-density lipoprotein
ity. Atherosclerosis 1993;103:1–11.
cholesterol, triacylglycerols, and factor VII coagulant activity. J Am Diet
32. Angleton P, Chandler WL, Schmer G. Diurnal variation of tissue-type
plasminogen activator and its rapid inhibitor (PAI-1). Circulation 1989;
8. Williams CM. Beneficial nutritional properties of olive oil: implications
for postprandial lipoproteins and factor VII. Nutr Metab Cardiovasc Dis
33. Marckmann P, Sandstrom B, Jespersen J. Dietary effects on circadian
fluctuation in human blood coagulation factor VII and fibrinolysis. Ath-
9. Oakley FR, Sanders TA, Miller GJ. Postprandial effects of an oleic
acid-rich oil compared with butter on clotting factor VII and fibrinolysis
34. Nilsson L, Gafvels M, Musakka L, et al. VLDL activation of plasmin-
in healthy men. Am J Clin Nutr 1998;68:1202–7.
ogen activator inhibitor-1 (PAI-1) expression: involvement of the VLDL
10. Perez-Jimenez F, Castro P, Lopez-Miranda J, et al. Circulating levels of
receptor. J Lipid Res 1999;40:913–9.
endothelial function are modulated by dietary monounsaturated fat. Ath-
35. Dichtl W, Ares MP, Stollenwerk M, et al. In vivo stimulation of vascular
plasminogen activator inhibitor-1 production by very low-density li-
11. Lopez-Segura F, Velasco F, Lopez-Miranda J, et al. Monounsaturated
poprotein involves transcription factor binding to a VLDL-responsive
fatty acid-enriched diet decreases plasma plasminogen activator inhib-
element. Thromb Haemost 2000;84:706 –11.
itor type 1. Arterioscler Thromb Vasc Biol 1996;16:82– 8.
36. Sironi L, Mussoni L, Prati L, et al. Plasminogen activator inhibitor type-1
12. Willett WC, Sacks F, Trichopoulou A, et al. Mediterranean diet pyramid:
synthesis and mRNA expression in HepG2 cells are regulated by VLDL.
a cultural model for healthy eating. Am J Clin Nutr 1995;61:1402S– 6S.
Arterioscler Thromb Vasc Biol 1996;16:89 –96.
13. Petroni A, Blasevich M, Salami M, Papini N, Montedoro GF, Galli C.
37. Carroll MF, Schade DS. Timing of antioxidant vitamin ingestion alters
Inhibition of platelet aggregation and eicosanoid production by phenolic
postprandial proatherogenic serum markers. Circulation 2003;108:24 –31.
components of olive oil. Thromb Res 1995;78:151– 60.
38. Ren S, Shen GX. Impact of antioxidants and HDL on glycated LDL-
14. Kohyama N, Nagata T, Fujimoto S, Sekiya K. Inhibition of arachidonate
induced generation of fibrinolytic regulators from vascular endothelial
lipoxygenase activities by 2-(3,4-dihydroxyphenyl)ethanol, a phenolic
cells. Arterioscler Thromb Vasc Biol 2000;20:1688 –93.
compound from olives. Biosci Biotech Biochem 1997;61:347–50.
39. Devaraj S, Chan AV Jr, Jialal I. alpha-Tocopherol supplementation
15. Pacheco YM, Lopez S, Bermudez B, Abia R, Muriana FJ. Extra-virgin
decreases plasminogen activator inhibitor-1 and P-selectin levels in type
vs. refined olive oil on postprandial hemostatic markers in healthy sub-
2 diabetic patients. Diabetes Care 2002;25:524 –9.
jects. J Thromb Haemost 2006;4:1421–2.
40. Mertens I, Ballaux D, Funahashi T, et al. Inverse relationship between
16. Miro-Casas E, Farre Albaladejo M, Covas MI, et al. Capillary gas
plasminogen activator inhibitor-I activity and adiponectin in overweight and
chromatography-mass spectrometry quantitative determination of hy-
obese women. Interrelationship with visceral adipose tissue, insulin resis-
droxytyrosol and tyrosol in human urine after olive oil intake. Anal
tance, HDL-chol and inflammation. Thromb Haemost 2005;94:1190 –5.
41. Pannacciulli N, De Mitrio V, Marino R, Giorgino R, De Pergola G. Effect
17. Miro-Casas E, Covas MI, Farre M, et al. Hydroxytyrosol disposition in
of glucose tolerance status on PAI-1 plasma levels in overweight and
obese subjects. Obes Res 2002;10:717–25.
18. Bucolo G, David H. Quantitative determination of serum triacylglycer-
42. Mertens I, Considine RV, Van der Planken M, Van Gaal LF. Hemostasis
ols by the use of enzymes. Clin Chem 1973;19:476 – 82.
and fibrinolysis in non-diabetic overweight and obese men and women.
19. Allain CC, Poon LS, Chan CS, Richmond W, Fu PC. Enzymatic deter-
Is there still a role for leptin? Eur J Endocrinol 2006;155:477– 84.
mination of total serum cholesterol. Clin Chem 1974;20:470 –5.
43. Valle M, Martos R, Gascon F, Canete R, Zafra MA, Morales R. Low-
20. Briggs CJ, Anderson D, Johnson P, Deegan T. Evaluation of the poly-
grade systemic inflammation, hypoadiponectinemia and a high concen-
ethylene glycol precipitation method for the estimation of high-density
tration of leptin are present in very young obese children, and correlate
lipoprotein cholesterol. Ann Clin Biochem 1981;18:177– 81.
with metabolic syndrome. Diabetes Metab 2005;31:55– 62.
21. Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concen-
44. Banfi C, Eriksson P, Giandomenico G, et al. Transcriptional regulation
tration of low-density lipoprotein cholesterol in plasma, without use of
of plasminogen activator inhibitor type 1 gene by insulin: insights into
the preparative ultracentrifuge. Clin Chem 1972;18:499 –502.
the signaling pathway. Diabetes 2001;50:1522–30.
22. Riepponen P, Marniemi J, Rautaoja T. Immunoturbidimetric determi-
45. Samad F, Pandey M, Bell PA, Loskutoff DJ. Insulin continues to induce
nation of apolipoproteins A-1 and B in serum. Scand J Clin Lab Invest
plasminogen activator inhibitor 1 gene expression in insulin-resistant
mice and adipocytes. Mol Med 2000;6:680 –92.
23. Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF,
46. Nakamura T, Adachi H, Hirai Y, Satoh A, Ohuchida M, Imaizumi T.
Turner RC. Homeostasis model assessment: insulin resistance and beta-
Association of plasminogen activator inhibitor-1 with insulin resistance
cell function from fasting plasma glucose and insulin concentrations in
in Japan where obesity is rare. Metabolism 2003;52:226 –9.
47. Fujita H, Kang M, Eren M, Gleaves LA, Vaughan DE, Kume T. Foxc2
24. Kjalke M, Silveira A, Hamsten A, Hedner U, Ezban M. Plasma lipopro-
is a common mediator of insulin and transforming growth factor beta
teins enhance tissue factor-independent factor VII activation. Arterio-
signaling to regulate plasminogen activator inhibitor type I gene expres-
scler Thromb Vasc Biol 2000;20:1835– 41.
25. Mariani G, Bernardi F, Bertina R, et al. Serum phospholipids are the
48. Larsen LF, Bladbjerg EM, Jespersen J, Marckmann P. Effects of dietary
main environmental determinants of activated factor VII in the most
fat quality and quantity on postprandial activation of blood coagulation
common FVII genotype. European Union Concerted Action “Clotart.”
factor VII. Arterioscler Thromb Vasc Biol 1997;17:2904 –9.
49. Bellido C, Lopez-Miranda J, Blanco-Colio LM, et al. Butter and walnuts,
26. Fito´ M, Covas MI, Lamuela-Ravento´s RM, et al. Protective effect of
but not olive oil, elicit postprandial activation of nuclear transcription
olive oil and its phenolic compounds against low density lipoprotein
factor B in peripheral blood mononuclear cells from healthy men. Am J
If you are taking any medications on this list, they should be discontinued 14 days prior to surgery and only Tylenol should be taken for pain. All other medications that you are currently taking must be specifically cleared by your doctor prior to surgery. It is absolutely necessary that all of your current medications be specifically cleared by your doctor and the nursing staff. Medicati
 Intake of phenol-rich virgin olive oil improves the postprandialprothrombotic profile in hypercholesterolemic patients1–3
Juan Ruano, José Lo´pez-Miranda, Rafael de la Torre, Javier Delgado-Lista, Javier Ferna´ndez, Javier Caballero,María Isabel Covas, Yolanda Jiménez, Pablo Pérez-Martínez, Carmen Marín, Francisco Fuentes, andFrancisco Pérez-Jiménez
ABSTRACT
Intake of phenol-rich virgin olive oil improves the postprandialprothrombotic profile in hypercholesterolemic patients1–3
Juan Ruano, José Lo´pez-Miranda, Rafael de la Torre, Javier Delgado-Lista, Javier Ferna´ndez, Javier Caballero,María Isabel Covas, Yolanda Jiménez, Pablo Pérez-Martínez, Carmen Marín, Francisco Fuentes, andFrancisco Pérez-Jiménez
ABSTRACT but with different contents of phenolic compounds, had different
and were subsequently analyzed in a Jasco FP-920 spectroflu-
effects on hemostasis postprandially.
but with different contents of phenolic compounds, had different
and were subsequently analyzed in a Jasco FP-920 spectroflu-
effects on hemostasis postprandially. PHENOLS REDUCE PROTHROMBOSIS POSTPRANDIALLY
performed. A value of P 0.05 was considered to be statistically
Baseline characteristics of the hypercholesterolemic participants in the
significant. All analyses were carried out by using the statistical
software package SPSS (version 11.0; SPSS Inc, Chicago, IL).
PHENOLS REDUCE PROTHROMBOSIS POSTPRANDIALLY
performed. A value of P 0.05 was considered to be statistically
Baseline characteristics of the hypercholesterolemic participants in the
significant. All analyses were carried out by using the statistical
software package SPSS (version 11.0; SPSS Inc, Chicago, IL).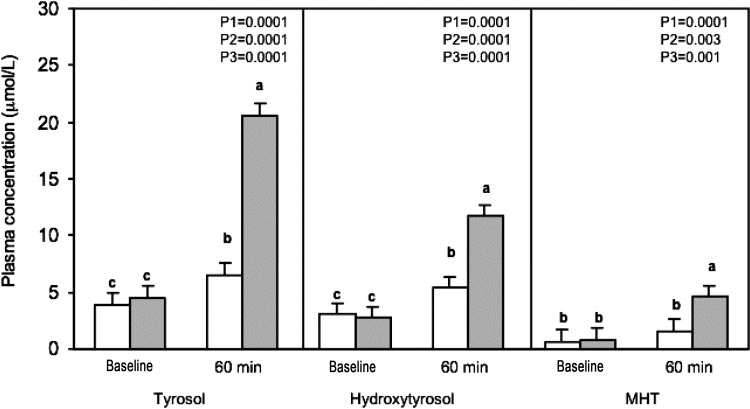
 FIGURE 1. Mean (ȀSD) concentrations of tyrosol, hydroxytyrosol, and 3-O-methyl-hydroxytyrosol (MHT) at baseline and 60 min after intake of a
FIGURE 1. Mean (ȀSD) concentrations of tyrosol, hydroxytyrosol, and 3-O-methyl-hydroxytyrosol (MHT) at baseline and 60 min after intake of a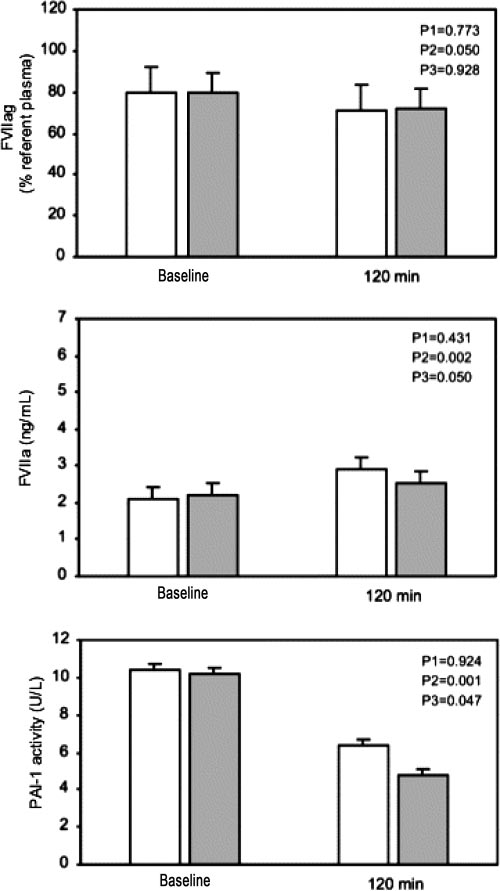
 PHENOLS REDUCE PROTHROMBOSIS POSTPRANDIALLY
between HOMA-IR, adiponectin, and PAI-1 were previouslyreported in both adults (40 – 42) and children (43). PAI-1 con-centrations are directly influenced by insulin (44), even in situ-ations of insulin resistance (45), a fact that has been explained interms of abdominal fat, via a higher concentration of cytokines insubjects with central obesity (41). Nevertheless, the associationof PAI-1 and insulin resistance has also been found in nonobesecohorts (46). These apparently contradictory findings may bepartially explained by the identification of a regulatory element(AP-1 response element) in the PAI-1 promoter. This elementenhances PAI-1 transcription by a factor of 7 when stimulated byinsulin increases mediated by FOX protein transcription factors(47), which may explain the association between insulin resis-tance and PAI-1. Interestingly, the same element also induces a3-fold rise in the PAI-1 transcription rate in the presence ofoxidative stress (48), as occurs in the postprandial state. Thedouble regulation of the PAI-1 promoter element may explainboth the fasting correlations between adiponectin, HOMA-IR,and PAI-1 and the larger postprandial decrease in PAI-1 after thephenol-rich breakfast as a result of its antioxidant properties and thelower activation of nuclear factor B that occurs after meals rich invirgin olive oil (49). In line with our findings, Pacheco et al (15)
recently found an enhancement in postprandial hemostasis after avery phenol-rich olive oil meal (1125 ppm of phenolic compounds),an enhancement that they evaluated in terms of a greater decrease inPAI-1, smaller tissue factor and fibrinogen AUCs, and a largerpostprandial decrease in tissue-type plasminogen activator.
PHENOLS REDUCE PROTHROMBOSIS POSTPRANDIALLY
between HOMA-IR, adiponectin, and PAI-1 were previouslyreported in both adults (40 – 42) and children (43). PAI-1 con-centrations are directly influenced by insulin (44), even in situ-ations of insulin resistance (45), a fact that has been explained interms of abdominal fat, via a higher concentration of cytokines insubjects with central obesity (41). Nevertheless, the associationof PAI-1 and insulin resistance has also been found in nonobesecohorts (46). These apparently contradictory findings may bepartially explained by the identification of a regulatory element(AP-1 response element) in the PAI-1 promoter. This elementenhances PAI-1 transcription by a factor of 7 when stimulated byinsulin increases mediated by FOX protein transcription factors(47), which may explain the association between insulin resis-tance and PAI-1. Interestingly, the same element also induces a3-fold rise in the PAI-1 transcription rate in the presence ofoxidative stress (48), as occurs in the postprandial state. Thedouble regulation of the PAI-1 promoter element may explainboth the fasting correlations between adiponectin, HOMA-IR,and PAI-1 and the larger postprandial decrease in PAI-1 after thephenol-rich breakfast as a result of its antioxidant properties and thelower activation of nuclear factor B that occurs after meals rich invirgin olive oil (49). In line with our findings, Pacheco et al (15)
recently found an enhancement in postprandial hemostasis after avery phenol-rich olive oil meal (1125 ppm of phenolic compounds),an enhancement that they evaluated in terms of a greater decrease inPAI-1, smaller tissue factor and fibrinogen AUCs, and a largerpostprandial decrease in tissue-type plasminogen activator. 3. Byrne CD, Wareham NJ, Martensz ND, Humphries SE, Metcalfe JC,
27. Roche HM, Zampelas A, Knapper JM, et al. Effect of long-term olive oil
Grainger DJ. Increased PAI activity and PAI-1 antigen occurring with an
dietary intervention on postprandial triacylglycerol and factor VII me-
oral fat load: associations with PAI-1 genotype and plasma active TGF-
tabolism. Am J Clin Nutr 1998;68:552– 60.
3. Byrne CD, Wareham NJ, Martensz ND, Humphries SE, Metcalfe JC,
27. Roche HM, Zampelas A, Knapper JM, et al. Effect of long-term olive oil
Grainger DJ. Increased PAI activity and PAI-1 antigen occurring with an
dietary intervention on postprandial triacylglycerol and factor VII me-
oral fat load: associations with PAI-1 genotype and plasma active TGF-
tabolism. Am J Clin Nutr 1998;68:552– 60.