Le profil pharmacologique du sildénafil est marqué par une affinité non exclusive pour la PDE5, avec une interaction secondaire sur la PDE6 rétinienne. Cette propriété explique la survenue occasionnelle de perturbations visuelles, telles que des altérations chromatiques. Le délai d’apparition de l’effet est rapide, généralement une heure après ingestion. Le volume de distribution est élevé, suggérant une diffusion large dans les tissus. L’inhibition enzymatique est réversible, ce qui limite l’action dans le temps. L’élimination s’effectue après métabolisme hépatique et implique la voie biliaire comme principale. Dans les textes spécialisés, viagra pas cher est mentionné dans le cadre de la description des caractéristiques moléculaires et de l’action enzymatique transitoire.
Microsoft word - infant girl.doc
Hypothalamic Hamartoma with Precocious Puberty in infant girl: Case Report
By: Prof. Dr. Abdel-Wahab M. Ibrahim, MD, FRCS, LRCP, and Ibrahim Abdel-Aal MSc, Mansoura Neurosurgery Department, Manoura University, Egypt. Email: [email protected]Introduction:
Sexual precocity can result from primary dysfunction of the neuroendocrine system within the brain. Various entities are implicated to be involved in precocious puberty: hypothalamic hamartomas, astrocytomas, suprasellar cysts, hydrocephalus, craniopharyngiomas and postinfec-tious states [1]. Central nervous system hamartomas are usually encountered in proximity to the hypothalamus [2, 3]. Hypothalamic hamartoma is a rare congenital non neo-plastic heterotopia consisting of neurons, glial cells and fiber bundles. Clinically, most patients with hypothalamic hamartomas present with precocious puberty and/or gelastic epilepsy and behavioural abnormality [1,4].
The pathogenesis of precocious puberty and its optimal treatment has not been established. The therapeutic options include both surgical excision and administration of a GnRH analogue [5]. We report an interesting case of precious puberty caused by hypothalamic hamartoma in an infant girl and review of literature.
Case Report:
A 1.5-year-old infant girl referred to our neurosurgery department from pediatric department, who presented with premature development of secondary sexual characters such as pubic hair growth, enlargement of the both breast, and vaginal discharge for the last 4 months prior to admission. On examination, her height was 91 cm and her weight 14.8 kg. General examination revealed, enlargement of both breasts, premature suprapubic hair growth with vaginal discharge. Neurological examination revealed no abnormality. Her hematological and other routine biochemical investigations showed no abnormality.
Endocrinal evaluation revealed FSH: 6 mlu/ml ( N 3.4 -10 ) LH: 7 mlu/ml (N 1.6 - 8.3 ) ESTRADIOL: 31.3pg/ml (Follicular Phase) PROLACTINE: 25.3 ng/ml with normal ACTH and T3 , T4 ,and TSH . The bone age was that of 2-2.5 year-old (Fig 2). Pre and post contrast CT scan Brain showed a small rounded lesion in the suprasellar area without enhancement (Fig 3). Her cranial MRI revealed a well- defined; suprasellar rounded mass lesion isointense in all pulse sequences to brain tissue measuring 15x15X1.5 mm, abutting the optic chaisma. The lesion has No gadolinium enhanced after gadolinium administration (fig. 4). The lesion was resected via a right subfrontal approach, and partial excision was done with smooth postoperative condition.
Fig (1) A 1.5 year old infant girl with enlargement of breast and pubic hair growth
Fig (2) X ray of ossification centre of metacarpal heads and knee denoting that patient
Fig (3) pre and post contrast CT scan Brain axial cuts
Figure (4) MRI brain T1WI precontrast , axial T2 WI , Sagittal post contrast
And Coronal T2WI after gadolinium showed a small rounded well defined isointense lesion in
All studies in the area of suprasellar area with no enhancement in postcontrast study
Fig (5) A 3 months follow up MRI brain postcontrast
Showed decrease in the size of hamartoma
Lesion was approached by right subfrontal approach, through the space between the optic nerve and the right carotid artery. The pituitary stalk was identified and preserved and the lesion was excised partially piecemeal. The lesion was grayish white, firm, non suckable and was found attached to the floor of the anterior third ventricle. Postoperative period was smooth. The histopathological examination of tissue showed a hamartoma.
At 3 months follow up, the patient clinically has a good general and neurological condition but still has an enlarged breast with pubic hair; Endocrinological evaluation revealed normalization of hormone levels. Serum FSH drop to 2.9 IU/L, serum LH to 1.5 IU/L , and s. Prolactin to 5.5 ng/ml. Repeated MRI brain revealed a decease in the size of hamrtoma (Fig 5)
Discussion:
Since the first case reported in 1934, about 100 cases of hypothalamic hamartomas have been reported in the literature [2]. Most of these patients present with isosexual precocious puberty. Hypothalamic hamartoma is the cause of 75% of cases of sexual precocious puberty in 1- to 3-year-old children [6]. Precocious puberty is defined as the occurrence of puberty in girls aged less than 8 years and in boys aged less than 9.5 years [3]. Males have a deepening of the voice, muscular development, acne, pubic hair and enlarged testes and penis. In females, breast development, menses, pubic hair and excessive muscularity are noted [3]. The children are large for the age, and bone age is advanced by at least 3 years [7]. In up to 21 % of the patients, gelastic seizures occur [8]. The pathogenesis of these peculiar symptoms is still not clear.
In the case of sexual precocity, it has been speculated that the local pressure [1, 9], abnormal neuronal connections [10], an independent endocrine activity [11, 12] or a combination of these may play a role.
Precocious puberty may have peripheral or central causes. Peripheral causes include those conditions in which sex steroid stimulation is via a mechanism other than GnRH-stimulated pituitary gonadotropin secretion. On the other hand, central causes result in physiologically normal but early puberty as a consequence of episodic GnRH, LH and FSH secretion [3]. Various pathological abnormalities that affect the hypothalamus, such as arachnoid cysts within the third ventricle, trauma, septo-optic dysplasia, neurophacomatoses, irradiation, neoplasms and hamartomas, can result in central precocious puberty [3]. Hamartomas act as independent neurosecre-tory organs, releasing GnRH granules into the tuber cine-reum, where they are released into the hypophyseal portal circulation [3, 11, 12]. The GnRH-containing neurons within the hamartoma act as independent episodic pulsatile secretory units and are outside the normal neurophys-iological regulation [3].
On the CT scan, hypothalamic hamartomas appear as isodense, enhancing masses located below the hypothalamus. They are frequently attached to the hypothalamus by a pedicle. However, MRI is the diagnostic imaging study of choice to define the morphology of the lesion. Ti-weighted images show an iso intense mass and T2-weighted images show hamartomas to be isointense to hyperintense, relative to the gray matter [3].
Arita et al. [4] classified hypothalamic hamartomas into two types: 'pa-rahypothalamic' and 'intrahypothalamic'. The parahypo-thalamic type of hamartoma is attached to the floor of the third ventricle or suspended from the floor by a peduncle. The intrahypothalamic type consists of a hamartoma enveloping the hypothalamus and distorts the third ventricle [4]. Parahypothalamic hamartomas are associated with precocious puberty and intrahypothalamic hamartomas present with intractable seizure [4]. The majority of hamartomas are pedunculated and extend into the inter-peduncular cistern; the remaining hamartomas are sessile, with a wide attachment to the hypothalamus [13].
The case reported here had a narrow attachment to the floor of the third ventricle. Microscopically,
hypothalamic hamartomas are primarily composed of mature neurons interspersed with glial cells. There is moderate glial cellu-larity within a fibrillar background and without characteristics of neoplastic differentiation [9, 13]. There are independent neuroendocrine units with neurons containing neurosecretory granules, blood vessels with fenestrated endothelium, and double basement membranes may be present [12]. Pathologically, hamartomas have to be differentiated from low-grade gliomas, gangliogliomas and gangliocytomas.
Treatment of precocious puberty is aimed at stopping untimely pubertal development to avoid psychosocial consequences related to it and to slow rapid growth and skeletal maturation to avoid tall stature in childhood, early growth cessation and short stature in adulthood [3]. Precocious puberty secondary to hypothalamic hamartoma can be treated by a GnRH analog. The GnRH from a hamartoma is released in an independent episodic pulsatile pattern [11]. Since pulsatile GnRH release is necessary to initiate puberty, continuous pituitary stimulation by either GnRH or a GnRH analogue will maintain persistently high GnRH levels, inhibit gonadotrophin secretion and stop puberty from progressing [14]. Similarly, long-acting GnRH therapy has also been reported to cause regression of hypothalamic hamartoma [5]. However, there are various disadvantages associated with GnRH analog therapy.
The treatment is very expensive and it may not reverse the muscularity and adolescent personality often seen in these patients. Similarly, treatment may be necessary for many years depending on the age of the child, and it may be associated with various side effects [3]. Surgery is the mainstay of treatment for precocious puberty due to hypothalamic hamartoma. The majority of cases can be cured by surgery [2, 3, 15]. Various surgical approaches have been used for the removal of hypothalamic hamartoma and include subtemporal, pterional and rarely transcallosal approaches [2, 3, 16, 17].
Most resections of hamartomas were performed using pterional approach [2, 15]. However, Albright et al. [3] used the sub-temporal approach for the removal of hypothalamic hamartoma. In their patients, the hamartomas were adherent posteriorly to the anterior surface of the brainstem and basilar artery, and lysing these adhesions using the pterional approach would have been difficult. Sessile lesions are harder to remove and a subtotal excision of only the exophytic portion is indicated leaving the residual tumor flush with the ventral surface of the hypothala-mus [3]. However, Rosenfeld et al. [17] reported a total excision of the sessile or intrahypothalamic type of hamartomas using transcallosal approach without any complications. Gamma knife radiosurgery can be an effective and safe alternative treatment modality for hypothalamic hamartoma capable of achieving good seizure control and improving behavioral disorders in selected cases [18].
Conclusion:
Considering the risk of surgery and the possibility incomplete response, hormonal treatment ideally should be the initial treatment of CPP secondary to hypothalamic hamartoma ; however the cost and availability of treatment may be the deciding factors in some areas. References:
1. Balagura S, Shulman K, Sobel EH: Precocious puberty of cerebral origin. Surg Neurol 1979;
2. Luo S, Li C, Ma Z, Zhang Y, Jia G, Cheng Y: Microsurgical treatment for hypothalamic ha
martoma in children with precocious puberty. Surg Neurol 2002;57:356-362.
3. Albright AL, Lee PA: Neurosurgical treatment of hypothalamic hamartomas causing preco cious
4. Arita K, Ikawa F, Kurisu K, Sumida M, Ha- rada K, Uozumi T, Monden S, Yoshida J,
Nishi Y: The relationship between magnetic resonance imaging findings and clinical mani festations of hypothalamic hamartoma. J Neu rosurg 1999;91:212-220.
5. Harada K, Yoshida J, Wakabayashi T, Okabe H, Sugita K: A super long-acting LH-RH ana
logue induces regression of hypothalamic hamartoma associated with precocious puberty. Acta Neurochir (Wien) 1995;137:102-105.
6. Starceski PJ, Lee PA, Albright AL, Migeon CJ: Hypothalamic hamartomas and sexual precoci
ty. Evaluation of treatment options. Am J Dis Child 1990; 144:225-228.
7. Markin RS, Leibrock LG, Huseman CA, McComb RD: Hypothalamic hamartoma: A
report of 2 cases. Pediatr Neurosci 1987; 13:19- 26.
8. Boyko OB, Curnes JT, Oakes WJ, Burger PC:Hamartomas of the tuber cinereum: CT, MR,
and pathologic findings. AJNR Am J Neurora-diol 1991; 12:309-314.
9. Alvarez-Garijo JA, Albiach VJ, Vila MM, Mulas F, Esquembre V: Precocious puberty and
hypothalamic hamartoma with total recovery after surgical treatment. Case report. J Neuro surg 1983;58:583-585.
10. Wolman L, Balmforth GV: Precocious puberty due to hypothalamic hamartoma in a patient
surviving to late middle age. J Neurol Neuro surg Psychiatry 1963:26:275-280.
11. Culler FL, James HE, Simon ML, Jones KL: Identification of gonadotropin-releasing hor
mone in neurons of a hypothalamic hamartoma in a boy with precocious puberty. Neuro- surgeryl985;17:408-412.
12. Judge DM, Kulin HE, Page R, Santen R, Tra- pukdi S: Hypothalamic hamartoma: A source
of luteinizing-hormone-releasing factor in precocious puberty. N Engl J Med 1977;296:7-10.
13. Yamada S, Sano T: Neuropathology of the hypothalamus; in Barrow DL, Selman W
(eds):Neuroendocrinology. Baltimore, Williams & Wilkins,pp 259-278.
14. Conn PM, Crowley WF Jr: Gonadotropin releasing hormones and its analogues. N Engl J
15. Romner B, Trumpy JH, Marhaug G, Isaksson HJ, Anke IM: Hypothalamic hamartoma caus
ing precocious puberty treated by surgery: Case report. Surg Neurol 1994;41:306-309.
16. Stewart L, Steinbok P, Daaboul J: Role of surgical resection in the treatment of hypothalam
ic hamartomas causing precocious puberty. Report of six cases. J Neurosurg 1998;88:340- 345.
17. Rosenfeld JV, Harvey AS, Wrennall J, Zacharian M, Berkovic SF: Transcallosal resection of
hypothalamic hamartomas, with control of seizures, in children with gelastic epilepsy. Neuro- surgery2001;48:108-118.
18. Unger F, Schrottner O, Feichtinger M, Bone G, Haselsberger K, Sutter B: Stereotactic radiosur
gery for hypothalamic hamartomas. Acta Neurochir Suppl 2002;84:57-63.
All Rights Reserved (c) Egyptian Society of Neurological Surgeons (ESNS) www.esns.org.eg
Health Update From: Hugh F. Stallworth, MD, MPH Tainted Weight Loss Products Monterey County Health Officials are alerting health care providers to the finding of new undeclared drug ingredients in over the counter weight loss products The U.S. Food and Drug Administration (FDA) has expanded, for the second time, the nationwide alert to consumers about tainted weight loss
✦ InterChange With American soldiers returning from combat in the Middle East, thesubject of post-traumatic stress disorder (PTSD) is in the news. The disorderhas been closely associated with the stress and strain of war, but it’s importantto note that this problem doesn’t just affect veterans, but a surprising numberIn fact, a study by the Veterans Administration (VA) involving the ge
 Hypothalamic Hamartoma with Precocious Puberty in infant girl:
Hypothalamic Hamartoma with Precocious Puberty in infant girl: 




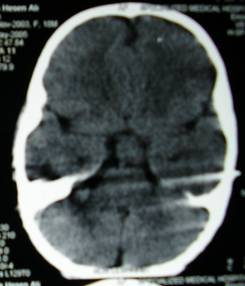
 Fig (1) A 1.5 year old infant girl with enlargement of breast and pubic hair growth
Fig (2) X ray of ossification centre of metacarpal heads and knee denoting that patient
Fig (3) pre and post contrast CT scan Brain axial cuts
Fig (1) A 1.5 year old infant girl with enlargement of breast and pubic hair growth
Fig (2) X ray of ossification centre of metacarpal heads and knee denoting that patient
Fig (3) pre and post contrast CT scan Brain axial cuts

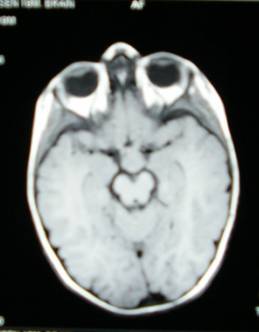
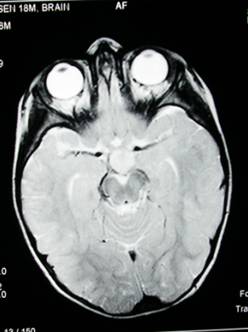
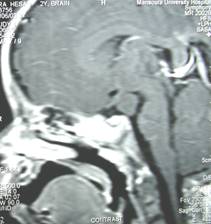
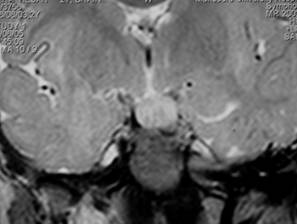
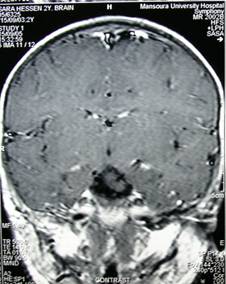
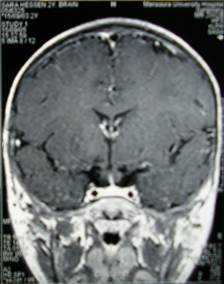 Figure (4) MRI brain T1WI precontrast , axial T2 WI , Sagittal post contrast
And Coronal T2WI after gadolinium showed a small rounded well defined isointense lesion in
All studies in the area of suprasellar area with no enhancement in postcontrast study
Fig (5) A 3 months follow up MRI brain postcontrast
Showed decrease in the size of hamartoma
Figure (4) MRI brain T1WI precontrast , axial T2 WI , Sagittal post contrast
And Coronal T2WI after gadolinium showed a small rounded well defined isointense lesion in
All studies in the area of suprasellar area with no enhancement in postcontrast study
Fig (5) A 3 months follow up MRI brain postcontrast
Showed decrease in the size of hamartoma
 Lesion was approached by right subfrontal approach, through the space between the optic nerve and the right carotid artery. The pituitary stalk was identified and preserved and the lesion was excised partially piecemeal. The lesion was grayish white, firm, non suckable and was found attached to the floor of the anterior third ventricle. Postoperative period was smooth. The histopathological examination of tissue showed a hamartoma.
At 3 months follow up, the patient clinically has a good general and neurological condition but still has an enlarged breast with pubic hair; Endocrinological evaluation revealed normalization of hormone levels. Serum FSH drop to 2.9 IU/L, serum LH to 1.5 IU/L , and s. Prolactin to 5.5 ng/ml. Repeated MRI brain revealed a decease in the size of hamrtoma (Fig 5)
Discussion:
Lesion was approached by right subfrontal approach, through the space between the optic nerve and the right carotid artery. The pituitary stalk was identified and preserved and the lesion was excised partially piecemeal. The lesion was grayish white, firm, non suckable and was found attached to the floor of the anterior third ventricle. Postoperative period was smooth. The histopathological examination of tissue showed a hamartoma.
At 3 months follow up, the patient clinically has a good general and neurological condition but still has an enlarged breast with pubic hair; Endocrinological evaluation revealed normalization of hormone levels. Serum FSH drop to 2.9 IU/L, serum LH to 1.5 IU/L , and s. Prolactin to 5.5 ng/ml. Repeated MRI brain revealed a decease in the size of hamrtoma (Fig 5)
Discussion:  hypothalamic hamartomas are primarily composed of mature neurons interspersed with glial cells. There is moderate glial cellu-larity within a fibrillar background and without characteristics of neoplastic differentiation [9, 13]. There are independent neuroendocrine units with neurons containing neurosecretory granules, blood vessels with fenestrated endothelium, and double basement membranes may be present [12]. Pathologically, hamartomas have to be differentiated from low-grade gliomas, gangliogliomas and gangliocytomas.
Treatment of precocious puberty is aimed at stopping untimely pubertal development to avoid psychosocial consequences related to it and to slow rapid growth and skeletal maturation to avoid tall stature in childhood, early growth cessation and short stature in adulthood [3]. Precocious puberty secondary to hypothalamic hamartoma can be treated by a GnRH analog. The GnRH from a hamartoma is released in an independent episodic pulsatile pattern [11]. Since pulsatile GnRH release is necessary to initiate puberty, continuous pituitary stimulation by either GnRH or a GnRH analogue will maintain persistently high GnRH levels, inhibit gonadotrophin secretion and stop puberty from progressing [14]. Similarly, long-acting GnRH therapy has also been reported to cause regression of hypothalamic hamartoma [5]. However, there are various disadvantages associated with GnRH analog therapy.
The treatment is very expensive and it may not reverse the muscularity and adolescent personality often seen in these patients. Similarly, treatment may be necessary for many years depending on the age of the child, and it may be associated with various side effects [3]. Surgery is the mainstay of treatment for precocious puberty due to hypothalamic hamartoma. The majority of cases can be cured by surgery [2, 3, 15]. Various surgical approaches have been used for the removal of hypothalamic hamartoma and include subtemporal, pterional and rarely transcallosal approaches [2, 3, 16, 17].
Most resections of hamartomas were performed using pterional approach [2, 15]. However, Albright et al. [3] used the sub-temporal approach for the removal of hypothalamic hamartoma. In their patients, the hamartomas were adherent posteriorly to the anterior surface of the brainstem and basilar artery, and lysing these adhesions using the pterional approach would have been difficult. Sessile lesions are harder to remove and a subtotal excision of only the exophytic portion is indicated leaving the residual tumor flush with the ventral surface of the hypothala-mus [3]. However, Rosenfeld et al. [17] reported a total excision of the sessile or intrahypothalamic type of hamartomas using transcallosal approach without any complications. Gamma knife radiosurgery can be an effective and safe alternative treatment modality for hypothalamic hamartoma capable of achieving good seizure control and improving behavioral disorders in selected cases [18].
Conclusion:
hypothalamic hamartomas are primarily composed of mature neurons interspersed with glial cells. There is moderate glial cellu-larity within a fibrillar background and without characteristics of neoplastic differentiation [9, 13]. There are independent neuroendocrine units with neurons containing neurosecretory granules, blood vessels with fenestrated endothelium, and double basement membranes may be present [12]. Pathologically, hamartomas have to be differentiated from low-grade gliomas, gangliogliomas and gangliocytomas.
Treatment of precocious puberty is aimed at stopping untimely pubertal development to avoid psychosocial consequences related to it and to slow rapid growth and skeletal maturation to avoid tall stature in childhood, early growth cessation and short stature in adulthood [3]. Precocious puberty secondary to hypothalamic hamartoma can be treated by a GnRH analog. The GnRH from a hamartoma is released in an independent episodic pulsatile pattern [11]. Since pulsatile GnRH release is necessary to initiate puberty, continuous pituitary stimulation by either GnRH or a GnRH analogue will maintain persistently high GnRH levels, inhibit gonadotrophin secretion and stop puberty from progressing [14]. Similarly, long-acting GnRH therapy has also been reported to cause regression of hypothalamic hamartoma [5]. However, there are various disadvantages associated with GnRH analog therapy.
The treatment is very expensive and it may not reverse the muscularity and adolescent personality often seen in these patients. Similarly, treatment may be necessary for many years depending on the age of the child, and it may be associated with various side effects [3]. Surgery is the mainstay of treatment for precocious puberty due to hypothalamic hamartoma. The majority of cases can be cured by surgery [2, 3, 15]. Various surgical approaches have been used for the removal of hypothalamic hamartoma and include subtemporal, pterional and rarely transcallosal approaches [2, 3, 16, 17].
Most resections of hamartomas were performed using pterional approach [2, 15]. However, Albright et al. [3] used the sub-temporal approach for the removal of hypothalamic hamartoma. In their patients, the hamartomas were adherent posteriorly to the anterior surface of the brainstem and basilar artery, and lysing these adhesions using the pterional approach would have been difficult. Sessile lesions are harder to remove and a subtotal excision of only the exophytic portion is indicated leaving the residual tumor flush with the ventral surface of the hypothala-mus [3]. However, Rosenfeld et al. [17] reported a total excision of the sessile or intrahypothalamic type of hamartomas using transcallosal approach without any complications. Gamma knife radiosurgery can be an effective and safe alternative treatment modality for hypothalamic hamartoma capable of achieving good seizure control and improving behavioral disorders in selected cases [18].
Conclusion:  5. Harada K, Yoshida J, Wakabayashi T, Okabe H, Sugita K: A super long-acting LH-RH ana
logue induces regression of hypothalamic hamartoma associated with precocious puberty. Acta Neurochir (Wien) 1995;137:102-105.
6. Starceski PJ, Lee PA, Albright AL, Migeon CJ: Hypothalamic hamartomas and sexual precoci
ty. Evaluation of treatment options. Am J Dis Child 1990; 144:225-228.
7. Markin RS, Leibrock LG, Huseman CA, McComb RD: Hypothalamic hamartoma: A
report of 2 cases. Pediatr Neurosci 1987; 13:19- 26.
8. Boyko OB, Curnes JT, Oakes WJ, Burger PC:Hamartomas of the tuber cinereum: CT, MR,
and pathologic findings. AJNR Am J Neurora-diol 1991; 12:309-314.
9. Alvarez-Garijo JA, Albiach VJ, Vila MM, Mulas F, Esquembre V: Precocious puberty and
hypothalamic hamartoma with total recovery after surgical treatment. Case report. J Neuro surg 1983;58:583-585.
10. Wolman L, Balmforth GV: Precocious puberty due to hypothalamic hamartoma in a patient
surviving to late middle age. J Neurol Neuro surg Psychiatry 1963:26:275-280.
11. Culler FL, James HE, Simon ML, Jones KL: Identification of gonadotropin-releasing hor
mone in neurons of a hypothalamic hamartoma in a boy with precocious puberty. Neuro- surgeryl985;17:408-412.
12. Judge DM, Kulin HE, Page R, Santen R, Tra- pukdi S: Hypothalamic hamartoma: A source
of luteinizing-hormone-releasing factor in precocious puberty. N Engl J Med 1977;296:7-10.
13. Yamada S, Sano T: Neuropathology of the hypothalamus; in Barrow DL, Selman W
(eds):Neuroendocrinology. Baltimore, Williams & Wilkins,pp 259-278.
14. Conn PM, Crowley WF Jr: Gonadotropin releasing hormones and its analogues. N Engl J
15. Romner B, Trumpy JH, Marhaug G, Isaksson HJ, Anke IM: Hypothalamic hamartoma caus
ing precocious puberty treated by surgery: Case report. Surg Neurol 1994;41:306-309.
16. Stewart L, Steinbok P, Daaboul J: Role of surgical resection in the treatment of hypothalam
ic hamartomas causing precocious puberty. Report of six cases. J Neurosurg 1998;88:340- 345.
17. Rosenfeld JV, Harvey AS, Wrennall J, Zacharian M, Berkovic SF: Transcallosal resection of
hypothalamic hamartomas, with control of seizures, in children with gelastic epilepsy. Neuro- surgery2001;48:108-118.
18. Unger F, Schrottner O, Feichtinger M, Bone G, Haselsberger K, Sutter B: Stereotactic radiosur
gery for hypothalamic hamartomas. Acta Neurochir Suppl 2002;84:57-63.
All Rights Reserved (c) Egyptian Society of Neurological Surgeons (ESNS)
5. Harada K, Yoshida J, Wakabayashi T, Okabe H, Sugita K: A super long-acting LH-RH ana
logue induces regression of hypothalamic hamartoma associated with precocious puberty. Acta Neurochir (Wien) 1995;137:102-105.
6. Starceski PJ, Lee PA, Albright AL, Migeon CJ: Hypothalamic hamartomas and sexual precoci
ty. Evaluation of treatment options. Am J Dis Child 1990; 144:225-228.
7. Markin RS, Leibrock LG, Huseman CA, McComb RD: Hypothalamic hamartoma: A
report of 2 cases. Pediatr Neurosci 1987; 13:19- 26.
8. Boyko OB, Curnes JT, Oakes WJ, Burger PC:Hamartomas of the tuber cinereum: CT, MR,
and pathologic findings. AJNR Am J Neurora-diol 1991; 12:309-314.
9. Alvarez-Garijo JA, Albiach VJ, Vila MM, Mulas F, Esquembre V: Precocious puberty and
hypothalamic hamartoma with total recovery after surgical treatment. Case report. J Neuro surg 1983;58:583-585.
10. Wolman L, Balmforth GV: Precocious puberty due to hypothalamic hamartoma in a patient
surviving to late middle age. J Neurol Neuro surg Psychiatry 1963:26:275-280.
11. Culler FL, James HE, Simon ML, Jones KL: Identification of gonadotropin-releasing hor
mone in neurons of a hypothalamic hamartoma in a boy with precocious puberty. Neuro- surgeryl985;17:408-412.
12. Judge DM, Kulin HE, Page R, Santen R, Tra- pukdi S: Hypothalamic hamartoma: A source
of luteinizing-hormone-releasing factor in precocious puberty. N Engl J Med 1977;296:7-10.
13. Yamada S, Sano T: Neuropathology of the hypothalamus; in Barrow DL, Selman W
(eds):Neuroendocrinology. Baltimore, Williams & Wilkins,pp 259-278.
14. Conn PM, Crowley WF Jr: Gonadotropin releasing hormones and its analogues. N Engl J
15. Romner B, Trumpy JH, Marhaug G, Isaksson HJ, Anke IM: Hypothalamic hamartoma caus
ing precocious puberty treated by surgery: Case report. Surg Neurol 1994;41:306-309.
16. Stewart L, Steinbok P, Daaboul J: Role of surgical resection in the treatment of hypothalam
ic hamartomas causing precocious puberty. Report of six cases. J Neurosurg 1998;88:340- 345.
17. Rosenfeld JV, Harvey AS, Wrennall J, Zacharian M, Berkovic SF: Transcallosal resection of
hypothalamic hamartomas, with control of seizures, in children with gelastic epilepsy. Neuro- surgery2001;48:108-118.
18. Unger F, Schrottner O, Feichtinger M, Bone G, Haselsberger K, Sutter B: Stereotactic radiosur
gery for hypothalamic hamartomas. Acta Neurochir Suppl 2002;84:57-63.
All Rights Reserved (c) Egyptian Society of Neurological Surgeons (ESNS)