Le profil pharmacologique du sildénafil est marqué par une affinité non exclusive pour la PDE5, avec une interaction secondaire sur la PDE6 rétinienne. Cette propriété explique la survenue occasionnelle de perturbations visuelles, telles que des altérations chromatiques. Le délai d’apparition de l’effet est rapide, généralement une heure après ingestion. Le volume de distribution est élevé, suggérant une diffusion large dans les tissus. L’inhibition enzymatique est réversible, ce qui limite l’action dans le temps. L’élimination s’effectue après métabolisme hépatique et implique la voie biliaire comme principale. Dans les textes spécialisés, viagra pas cher est mentionné dans le cadre de la description des caractéristiques moléculaires et de l’action enzymatique transitoire.
092399 treatment of hair loss
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
Androgens are important in regulating hair growth. At puberty, androgens increase the size of follicles inthe beard, chest, and limbs and decrease the size of
A L A S T A I R J . J . W O O D , M . D. , Editor
follicles in the bitemporal region, which reshapes thehairline in men and many women. ANDROGENETIC ALOPECIA TREATMENT OF HAIR LOSS
Androgenetic alopecia is hereditary thinning of
the hair induced by androgens in genetically suscep-
tible men and women.7,8 This condition is also knownas male-pattern hair loss or common baldness in menand as female-pattern hair loss in women. Thinning
AIR loss is a common and distressing symp-
of the hair usually begins between the ages of 12
and 40 years in both sexes, and approximately half
promote hair growth — finasteride and mi-
the population expresses this trait to some degree
noxidil — we can now treat patients with some types
before the age of 50.9,10 The pattern of inheritance
of hair loss. Both drugs influence the hair-growth cy-
cle and increase the length and diameter of existing
Pathophysiology
hair, although their mechanisms of action differ. Inthis article, I will focus on the treatment of two com-
In susceptible hair follicles of the scalp, dihydro-
mon problems, androgenetic alopecia and alopecia
testosterone binds to the androgen receptor, and the
areata, both of which involve a reversible alteration
hormone-receptor complex then activates the genes
responsible for the gradual transformation of large,terminal follicles to miniaturized follicles.13-16 With
THE HAIR-GROWTH CYCLE
successive hair cycles, the duration of anagen shortens
Hair growth is cyclic, with phases of growth (an-
and the follicles become smaller, producing shorter,
agen), involution (catagen), and rest (telogen) (Fig.
finer hairs that cover the scalp poorly. These minia-
1).1-3 The cycles of active growth and rest are regu-
turized hairs of various lengths and diameters are the
lated by complex messages between the epithelium
hallmark of androgenetic alopecia.8,10,17 At the same
and the dermis that are not yet well understood. In
time, the number of follicles per unit of area remains
a normal scalp, most follicles are growing (90 to 95
percent), a few are undergoing involution (less than
Dihydrotestosterone is formed by the peripheral
1 percent), and the remainder are resting (5 to 10 per-
conversion of testosterone by 5a-reductase. There are
cent).4-6 At the end of telogen, hair is released and
two isoforms of 5a-reductase — type 1 and type 2 —
shed and the next cycle is initiated. Each day, up to
which, together with other enzymes, regulate specific
100 hairs in telogen are shed from the head and about
steroid transformations in the skin. Young men and
the same number of follicles enter anagen. The du-
young women with androgenetic alopecia have higher
ration of anagen determines the length of hair, and
levels of 5a-reductase, more androgen receptors, and
the volume of the hair bulb determines the diameter.
lower levels of cytochrome P-450 aromatase, which
We are born with all our terminal hair follicles —
converts testosterone to estradiol, in hair follicles in
approximately 100,000 on the scalp — that are pre-
the frontal region of the scalp than in the occipital
determined to grow long, thick hair. Other follicles
region.18 The various clinical patterns of androgenet-
are predetermined to grow vellus hair, which is short,
ic alopecia in men and women may reflect quanti-
fine, and relatively nonpigmented and covers much
tative differences in the levels of 5a-reductase, the
of the body. Follicles can become larger or smaller
number of androgen receptors, and the levels of aro-
under systemic and local influences that alter the du-
matase in specific regions of the scalp at various ages.
ration of anagen and the volume of the hair matrix. Treatment in Men
In men, androgenetic alopecia ranges from the
bitemporal recession of hair, to thinning of the fron-
From the Department of Dermatology, University of California at San
tal and vertex regions of the scalp, to complete bald-
Francisco, San Francisco. Address reprint requests to Dr. Price at 350 Par-
ness and loss of all hair except the occipital and tem-
nassus Ave., Ste. 404, San Francisco, CA 94117.
1999, Massachusetts Medical Society.
poral fringes. In some cases, men have diffuse thinning
Downloaded from www.nejm.org at ALBERT EINSTEIN COLLEGE OF MED on July 18, 2004.
Copyright 1999 Massachusetts Medical Society. All rights reserved. D R U G T H E R A P Y TABLE 1. SELECTIVE ACTIONS OF TESTOSTERONE Testosterone Spermatogenesis Dihydrotestosterone Growth of prostate Growth of terminal hair (beard, limbs, trunk, exter-
Bitemporal reshaping of hairlineAndrogenetic alopeciaAcne
Figure 1. Cycle of Scalp-Hair Growth.
is based on the absence of androgenetic alopecia in
Every scalp hair has a phase of growth (anagen), which lasts
men with congenital deficiency of type 2 5a-reduc-
two to six years; a phase of involution (catagen), which lasts two
tase19,23-26 and the presence of increased 5a-reductase
to three weeks; and a resting phase (telogen), which lasts two to
activity and dihydrotestosterone levels in hair follicles
three months and is followed by shedding of the hair. The cycleis then repeated. All hair loss affects or disrupts one of these
of men with balding scalps.16,18,27,28 Finasteride rapid-
ly lowers serum and scalp dihydrotestosterone levelsby more than 60 percent. It has no affinity for theandrogen receptor and therefore does not interferewith the actions of testosterone (Table 1), and it has
all over the scalp. The pattern of hair loss, combined
no androgenic, estrogenic, progestational, or other
with onset at an early age and the presence of min-
iaturized hairs, supports the diagnosis.
In three randomized, double-blind, placebo-con-
The goal of therapy is to increase coverage of the
trolled studies, a total of 1879 men who were 18 to
scalp and to retard further hair thinning. In the
41 years old with mild to moderately severe thin-
United States, oral finasteride, at a dose of 1 mg per
ning of the hair but not complete baldness received
day, and topical solutions of 5 percent and 2 percent
oral finasteride at a dose of 1 mg per day or placebo
minoxidil are currently the only drugs approved for
for one year.29-31 Two of these studies enrolled a total
promoting hair growth in men with androgenetic
of 1553 men with loss of hair predominantly at the
alopecia. Both drugs can increase coverage of the scalp
vertex, and the third enrolled 326 men with predom-
by enlarging existing hairs, and both retard further
inantly frontal hair loss. As compared with placebo,
thinning, in both the vertex and the frontal regions.
finasteride significantly increased hair counts and im-
However, neither drug restores all the hair, and the
proved scalp coverage, as was evident in photographs
response differs among men. A good candidate for
treatment has definite thinning and many miniatur-
In the men with hair loss at the vertex, the initial
ized hairs. If thinning is minimal, the main perceived
treatment was continued for a second year, but some
response may be retardation of further thinning. Nei-
men who received placebo for the first year were giv-
ther drug benefits men who are completely bald or
en finasteride and some who initially received finas-
those with bitemporal recession without visible hair.
teride were given placebo in the second year (Fig.
In general, treatment for 6 to 12 months is needed to
2). In the second year, hair counts remained stable at
improve scalp coverage. Continued treatment is need-
the increased level in the men who continued to re-
ed to maintain benefit; if treatment is stopped, the
ceive finasteride. Hair counts decreased in the men
benefits will be lost within 6 to 12 months and hair
who were switched from finasteride to placebo after
density will be the same as it would have been with-
one year, whereas the counts increased in those
switched from placebo to finasteride. There was a pro-gressive increase in scalp coverage, as determined by
Finasteride
global photographs of the scalp, in 66 percent of the
Finasteride is a competitive inhibitor of type 2
finasteride group, as compared with 7 percent of
5a-reductase and inhibits the conversion of testos-
the placebo group, after two years.29 These results
terone to dihydrotestosterone.19-22 The rationale for
indicate that the number of responding hairs is es-
the use of finasteride to treat male-pattern hair loss
tablished after about one year and that continued
Downloaded from www.nejm.org at ALBERT EINSTEIN COLLEGE OF MED on July 18, 2004.
Copyright 1999 Massachusetts Medical Society. All rights reserved.
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
male-pattern hair loss in men who were predomi-
nantly in their 60s and 70s and who were treated
with 5 mg of finasteride daily for benign prostatic
Finasteride at a dose of 1 mg daily is safe and well
tolerated. The only adverse effects in the clinical tri-
als, which included 1879 men, were reversible and
were reported by slightly more men in the finaster-
ide than in the placebo group; these effects included
decreased libido in 1.8 percent of the men in the fi-
nasteride group, as compared with 1.3 percent in theplacebo group; erectile dysfunction in 1.3 percent
and 0.7 percent, respectively; and ejaculatory dys-
function in 1.2 percent and 0.7 percent.31 These sex-
ual adverse effects gradually disappeared during pro-
longed treatment and disappeared in days or weeks
In men 18 to 41 years old who were taking 1 mg
of finasteride daily, serum prostate-specific antigenlevels decreased by 0.2 ng per milliliter,31 which was
Figure 2. Change in the Mean (±SE) Hair Count from Base Line
not a clinically important reduction. However, in old-
(Month 0) at the Anterior Leading Edge of the Vertex ThinningArea in Men Given 1 mg of Finasteride or Placebo Daily for 24
er men with benign prostatic hyperplasia, finasteride
at doses of 1 mg or 5 mg daily decreases serum pros-
In the second year, some men who received placebo during the
tate-specific antigen levels by about 50 percent. In
first 12 months were given finasteride and some who initially
older men who are taking finasteride, the results of
received finasteride were given placebo. The dotted line indi-
a prostate-specific antigen test should be doubled to
cates no change. Adapted from Kaufman et al.29 with the per-
compensate for the effect of the drug.32-34
Minoxidil
Minoxidil promotes hair growth when it has been
treatment increases the length, diameter, and pig-
affected by various conditions, including androge-
mentation of these hairs so that coverage of the scalp
netic alopecia. It increases the duration of anagen and
enlarges miniaturized and suboptimal follicles, irre-
After two years of treatment with finasteride,
spective of the underlying cause. For example, in ad-
about two thirds of men have improved scalp cover-
dition to its effectiveness in patients with androgenet-
age, about one third have the same amount of hair as
ic alopecia, minoxidil promotes hair growth in patients
they did at the outset, and about 1 percent lose hair.
with alopecia areata, congenital hypotrichosis, and
Since the miniaturization of follicles occurs over the
loose anagen syndrome. Minoxidil was developed to
course of many years, reversal of this process also takes
treat hypertension, and this aspect of the drug’s action
many years. With treatment for more than two years,
is the one that is best understood. It is a potassium-
the clinical impression is that scalp coverage continues
channel opener and vasodilator. Its mechanism of ac-
to increase; five-year controlled studies are in prog-
tion with respect to the stimulation of hair growth
ress to verify this impression. It is not known to what
is not known, but it appears to be independent of
extent follicles will enlarge, and there is no way to
vasodilatation.35-38 The addition of minoxidil to cul-
identify the men who will have the best response.
tures of hair follicles increases survival.35
In December 1997, 1-mg tablets of finasteride
A 2 percent solution of topical minoxidil was ap-
were approved by the Food and Drug Administration
proved by the FDA in 1988 for promoting hair
(FDA) for the treatment of androgenetic alopecia in
growth in men with androgenetic alopecia. Its effica-
men. It is to be given once daily, with or without
cy was established in a 12-month placebo-controlled
food. No dosage adjustments are needed on the ba-
study of 2294 men who were 18 to 50 years old and
sis of age or renal function. It is metabolized in the
had mild-to-moderate thinning of the hair at the
liver and should be used with caution in men with
vertex. Treatment with minoxidil significantly in-
abnormal liver function. In men who are 60 years of
creased hair counts.10,39-41 Histologic studies con-
age or older, finasteride may not be an effective treat-
firmed that minoxidil increases the diameter of the
ment for male-pattern hair loss, because type 2 5a-
reductase activity in the scalp may not be as high as
In 1997, a 5 percent solution of topical minoxidil
in younger men. This decreased activity may partly ex-
was approved by the FDA as an over-the-counter treat-
plain why there have been few reports of reversal of
ment for promoting hair growth. In a 48-week study
Downloaded from www.nejm.org at ALBERT EINSTEIN COLLEGE OF MED on July 18, 2004.
Copyright 1999 Massachusetts Medical Society. All rights reserved. D R U G T H E R A P Y
of twice-daily treatment with the 5 percent solution,
the 2 percent solution, or placebo in 393 men who
were 18 to 49 years old and had mild-to-moderate
thinning at the vertex, hair counts were 45 percent
higher among the 157 men in the group receiving5 percent minoxidil than among the 158 men in the
group receiving 2 percent minoxidil and almost fivetimes as high as those among the 78 men in the pla-
The efficacy of drugs that stimulate hair growth
can also be assessed by clipping and weighing hairgrown in a small, marked area on the scalp.44,45 Thismethod was used in a 96-week double-blind study
of four groups of nine men with androgenetic alope-cia.45 Three groups received one of the following:
5 percent topical minoxidil, 2 percent topical minox-
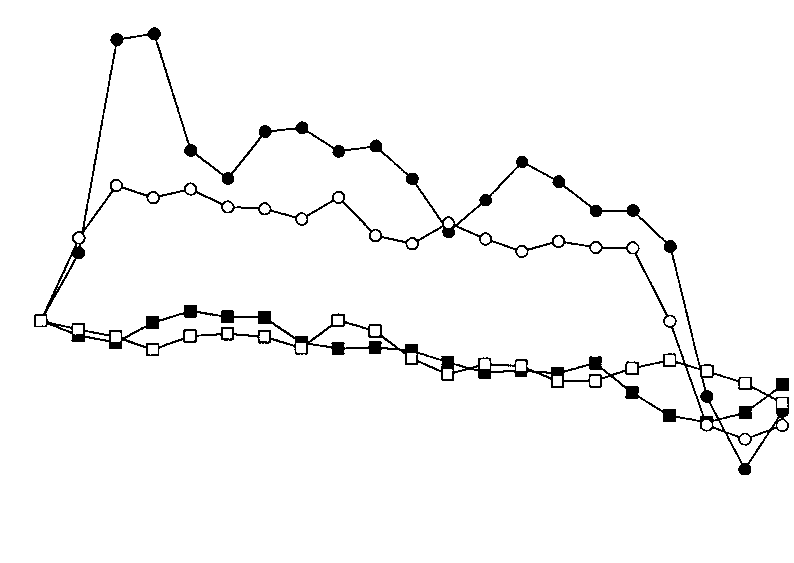
Figure 3. Mean Percent Change in Hair Weight per Square Cen-
idil, or placebo; the fourth group received no treat-
timeter of Scalp from Base Line (Week 0) among Men with An-
ment. Hair samples were taken from the frontal area
drogenetic Alopecia Who Received 5 Percent Minoxidil, 2 Per-
of the scalp. After 96 weeks, treatment was stopped
cent Minoxidil, Placebo, or No Treatment for 96 Weeks.
and the men were followed for 24 more weeks. Both
The dotted line indicates no change, and the vertical arrow at96 weeks marks the cessation of treatment. Adapted from Price
solutions of minoxidil were significantly superior (P<
et al.45 with the permission of the publisher.
0.05) to placebo or no treatment in promoting hairgrowth and slowing hair loss, with the 5 percent so-lution having the greater efficacy (Fig. 3); the placeboand untreated groups had a steady decrease in hairweight of about 6 percent per year. In the groups re-
solution because of its higher content of propylene
ceiving minoxidil, the peak hair weight was followed
glycol. Minoxidil or the formulated solution may also
by a similar small decline during this period. Never-
cause allergic contact dermatitis or photoallergic con-
theless, the hair weight in the minoxidil groups was
tact dermatitis.48-50 Hypertrichosis is another derma-
about 30 percent greater than that in the placebo
tologic adverse effect, which occurs in women but is
and untreated groups. The rapid loss of hair weight
after treatment with minoxidil was stopped (Fig. 3)
Neither the 5 percent nor the 2 percent solution
confirms its substantial growth-promoting effect.
of minoxidil alters systolic or diastolic blood pres-
Minoxidil initially causes a surge of growth in min-
sure, pulse rate, or body weight when applied twice
iaturized hairs (Fig. 3). These hairs continue to have
daily.43,51 With the 5 percent solution, the mean se-
a shortened growth cycle and fall out quickly, which
rum level of minoxidil is 1.2 ng per milliliter, well
explains the temporary increase in shedding that pa-
below the level of 20.0 ng per milliliter at which
tients may notice after 10 to 12 weeks of therapy.
minimal hemodynamic changes in pulse rate and
One milliliter of minoxidil solution must be applied
twice daily to achieve and then maintain efficacy.46The solution is applied to the scalp and spread lightly
Treatment in Women
with a finger; massage is not needed. Spray applica-
Androgenetic alopecia occurs as often in women
tors are not recommended, because most of the so-
as in men but is camouflaged by hair styling (Table
lution reaches the hair rather than the scalp. Men us-
2). In women, the thinning of hair is diffuse but is
ing minoxidil who wish to take finasteride should
most marked on the frontal or parietal areas of the
continue to apply minoxidil for at least four months
scalp. The process is milder in women than in men
after starting finasteride to prevent the loss of hair
because of differences in the level of 5a-reductase
that occurs after the cessation of minoxidil treatment
and cytochrome P-450 aromatase and in the number
(Fig. 3).45 The combined use of minoxidil and finas-
of androgen receptors in the hair follicles of the
teride has not been studied in humans, but in a study
scalp.18 Women typically retain a rim of hair along the
in stumptail macaques the effect of minoxidil and fi-
frontal hairline, even when the scalp is visible.8,10,52
nasteride combined was greater than the effect of
Increased spacing between hairs makes the “central
part” look wider over the frontal region of the scalp
The adverse effects of topical minoxidil are mainly
than over the occipital region. The patient may note
dermatologic. Irritation of the scalp, including dry-
that her “ponytail” is much thinner. The diagnosis
ness, scaling, itching, and redness, occurs in approx-
of androgenetic alopecia is supported by these clin-
imately 7 percent of patients who use the 2 percent
ical features, the presence of miniaturized hairs with
solution and in more of those who use the 5 percent
large variation in diameter and length, and onset at an
Downloaded from www.nejm.org at ALBERT EINSTEIN COLLEGE OF MED on July 18, 2004.
Copyright 1999 Massachusetts Medical Society. All rights reserved.
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
TABLE 2. MISCONCEPTIONS AND FACTS ABOUT ANDROGENETIC TABLE 3. EVALUATION OF WOMEN WITH ANDROGENETIC MISCONCEPTION CONDITIONS TO BE RULED OUT OR ASSESSED MEANS OF EVALUATION
the following are present: irregular menses, infertil-
Use of teasing, hair Use of hair styling, teasing,
*Androgen excess should be considered if any of the following are
present: irregular menses, infertility, hirsutism, severe cystic acne, viriliza-
*The incidence is the same as that among men.
the 5 percent solution was not significantly moreeffective than the 2 percent solution. An ongoing52-week placebo-controlled study of more than 500
early age. Biopsy of the scalp is not routinely needed
women is comparing the effectiveness of the two
but is helpful when the diagnosis is uncertain.
Most women with androgenetic alopecia have nor-
Minoxidil solution must be applied twice daily,
mal menses, pregnancies, and endocrine function,
which is a large drawback for some women. If the
including normal serum androgen levels. Extensive
hair has been washed, the scalp must be completely
hormonal evaluation is not usually needed unless oth-
dry before minoxidil is applied. The solution must
er symptoms and signs of androgen excess are present
be applied directly to the scalp with a dropper or ex-
(Tables 2 and 3). Other causes of hair loss may need
The severity and type of adverse effects of minox-
Women with androgenetic alopecia are often more
idil in women are the same as those in men, except
devastated by their thinning hair than are men.54,55
that hypertrichosis is more common. The incidence
They need reassurance that they will not become bald
of hypertrichosis is about 3 to 5 percent among wom-
and that they may safely use hair sprays, dyes, and
en who use 2 percent minoxidil and is higher among
permanents to make their hair appear fuller (Table 2).
those who use the 5 percent solution, although pre-cise data are lacking. It occurs above the eyebrows,
Minoxidil
in the malar region, laterally on the cheeks, and occa-
Topical minoxidil solution is the only drug avail-
sionally above the upper lip and on the chin. Hyper-
able for promoting hair growth in women with an-
trichosis diminishes or disappears after about one
drogenetic alopecia. The 2 percent solution of minox-
year, even with continued use of minoxidil, and it re-
idil was approved for this use by the FDA in 1991
solves within one to six months after the drug is
after it was found to be effective in two double-
stopped. Bleaching of the longer, darker hair usually
blind, placebo-controlled, 32-week studies of 550
suffices for cosmetic purposes; hair-removal proce-
women who were 18 to 45 years old.56,57 The mi-
dures are seldom needed. The reason for this sym-
noxidil-treated women had significantly higher hair
metric, dose-related hypertrichosis is not clear; local
counts than the women who received placebo. In a
intravascular spread by the extensive blood supply of
third 32-week study (of eight women), in which hair
the scalp, inadvertent manual transfer of minoxidil to
weight was the primary end point, the average total
the face, and contact with a pillow onto which mi-
hair weight increased by 42.5 percent in the minox-
noxidil has been transferred from the scalp have been
idil group as compared with 1.9 percent in the pla-
The 5 percent solution of topical minoxidil was
Finasteride
compared with the 2 percent solution in a total of
Finasteride is contraindicated in women who are
493 women with androgenetic alopecia in two pla-
or may become pregnant, because 5a-reductase in-
cebo-controlled studies, one 32 weeks long and the
hibitors may cause abnormalities of the external gen-
other 48 weeks long. On the basis of hair-count data,
italia of male fetuses. This contraindication is based
Downloaded from www.nejm.org at ALBERT EINSTEIN COLLEGE OF MED on July 18, 2004.
Copyright 1999 Massachusetts Medical Society. All rights reserved. D R U G T H E R A P Y
on findings in men with 5a-reductase deficiency.19,23
The assumption that alopecia areata is an autoim-
In 136 postmenopausal women with androgenetic
mune disease is based on the presence of activated
alopecia who were given 1 mg of finasteride or pla-
CD4 and CD8 lymphocytes around affected anagen
cebo daily for one year, both groups lost hair and
hair bulbs61,62 and on the ability to transfer alopecia
there was no significant difference in hair loss be-
areata by T lymphocytes from affected scalp to ex-
tween the finasteride and placebo groups.58
plants of human scalp on mice with severe combinedimmunodeficiency.63 As is the case with many other
Estrogen
autoimmune diseases, there is a strong association of
The role of estrogen in hair growth in humans is
alopecia areata with certain HLA class II alleles, es-
not clear. Estrogen, both oral and topical, has been
pecially DQB1*03 and DRB1*1104, which appear
used in women with androgenetic alopecia, although
to be markers of general susceptibility to alopecia ar-
no controlled studies have been done. Since topical
eata.64-66 In addition, the frequency of two other al-
minoxidil solution seems to be more effective than
leles — DRB1*0401 and DQB1*0301 — is signifi-
estrogen in terms of improving scalp coverage and
cantly increased among patients with alopecia totalis
slowing further hair loss, in my own practice, I no
and those with alopecia universalis, the most exten-
longer prescribe estrogen for women with androge-
netic alopecia. Nevertheless, the activity of aroma-tase in hair follicles in the frontal and occipital re-
Treatment
gions of the scalp hair is significantly higher in
Patients with alopecia areata are treated with ei-
women with androgenetic alopecia than in men
ther immunomodulating therapies, such as gluco-
with this condition. This higher activity may have a
corticoids, topical immunotherapy, or anthralin, or
role in the milder expression of this trait in women.18
biologic-response modifiers, such as minoxidil.61,67,68
When an oral contraceptive or a combination of
These treatments stimulate hair growth but do not
estrogen and progestin is prescribed for women with
prevent hair loss and probably do not influence the
androgenetic alopecia, care should be taken to select
course of the disease. Treatment should be contin-
a progestin with little or no androgenic activity,
ued until remission occurs or until residual patches
such as norgestimate or ethynodiol diacetate. Wom-
of alopecia are concealed by regrown hair, which
en with this condition should not take testosterone
may take months or years. The choice of therapy de-
or androgen precursors, such as dehydroepiandros-
pends primarily on the patient’s age and the extent
of the hair loss (Table 4).67,69 Treatment is most ef-fective in milder cases; no treatment works well for
Spironolactone
patients with total (100 percent) loss of scalp hair.
Spironolactone is a weak competitive inhibitor of
Hair follicles are not destroyed in patients with
the binding of androgen to its receptor, and it de-creases the synthesis of testosterone as well. It hassome efficacy in the treatment of hirsutism.59 It seemsto have little efficacy in women with androgeneticalopecia, but no controlled studies have been done
TABLE 4. TREATMENT FOR PATIENTS WITH ALOPECIA AREATA,
ACCORDING TO AGE AND SEVERITY OF CONDITION.*
and there are no data on hair count or hair weight,nor are there any photographic data. Patients «10 years of age 5% Topical minoxidil solution, topical glucocorticoid, or both ALOPECIA AREATA
Alopecia areata is an autoimmune disease that af-
Patients >10 years of age
fects almost 2 percent of the U.S. population.60 It
ranges in severity from small, round patches of hair
Intralesional glucocorticoid, 5% topical minoxidil solution, or both, with
loss that regrow spontaneously to persistent, exten-
sive patchy involvement to the loss of all scalp hair
5% Topical minoxidil solution, with or without topical glucocorticoid
(alopecia totalis) or all scalp and body hair (alopecia
universalis). Alopecia areata affects both sexes equal-
ly and occurs at all ages, although children and
young adults are affected most often. Spontaneous
remission and recurrence are common. The patients
Intralesional glucocorticoid, 5% topical minoxidil solution, or both
are usually otherwise healthy, but atopy, thyroid dis-
*The National Alopecia Areata Foundation, 710 C St., Ste. 11, San Rafael,
ease, and vitiligo are more common among them
CA 94901-3853 (telephone number, 415-456-4644; Web site, www.
than among the general population. Measurement
alopeciaareata.com), provides informational brochures, newsletters, research
of serum thyrotropin is recommended for children
updates, sources of scalp prostheses, videotapes for schoolchildren, and lo-cations of support groups and holds an annual conference to help patients
with alopecia areata, as well as those with a family
†Anthralin is left on the scalp for 20 to 60 minutes.
Downloaded from www.nejm.org at ALBERT EINSTEIN COLLEGE OF MED on July 18, 2004.
Copyright 1999 Massachusetts Medical Society. All rights reserved.
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
TABLE 5. SUGGESTED METHODS OF TREATMENT FOR ALOPECIA AREATA. Intralesional glucocorticoid All sites
The preferred compound is triamcinolone acetonide (10 mg/ml),* administered with a 3-ml syringe with a 30-gauge,
1/2-in.-long needle. Inject 0.1 ml or less into the mid-dermis at multiple sites 1 cm apart; do not raise wheal or inject
into subcutaneous tissue. Repeat every 4 to 6 weeks; if atrophy of the skin occurs, do not reinject affected site until atrophy resolves. Optional topical anesthesia may be used: apply a mixture of 2.5% lidocaine and 2.5% prilocaine (Emla cream) in a thick layer to intact skin and cover with occlusive dressing for one hour before injections are given; remove cream immediately before injections.
The maximal dose is 20 mg per visit. When more than 50% of scalp is affected, inject only selected sites.
The maximal dose is 1.25 mg per visit injected into the mid-dermis of each brow at 5 or 6 sites (for a total of 2.5 mg
The maximal dose is 7.5 mg per visit. 5% Topical minoxidil solution Scalp and beard
The maximal dose is 1 ml per application. Apply twice daily to affected sites. Spread solution with fingers. Wash hands
afterward. This treatment is not effective for patients with total (100 percent) loss of scalp hair.
Apply two applications to each eyebrow with a finger twice daily, using a mirror to ensure precise placement. Hold a
cotton ball over the eye for protection. Wash hands afterward. Anthralin (short contact)† Apply 0.5 to 1% anthralin cream to affected scalp once daily; leave on 20 to 30 minutes daily for 2 wk, then 45 minutes
daily for 2 wk, up to a maximum of 1 hour daily. Wash hands afterward and avoid getting anthralin in the eyes. Remove from scalp with mineral oil, then wash off with soap and water. Do not use on brows or beard. Some patients tolerate overnight application. Topical glucocorticoid Apply twice daily. Topical immunotherapy Use diphencyprone or squaric acid dibutyl ester to induce contact sensitization. For initial sensitization, apply 2% solution
of selected contact allergen in acetone to a 4-cm2 area on one side of the scalp. After initial sensitization, apply diluted solution of contact allergen weekly to same half of scalp in two coats. The patient washes off the allergen after 48 hr after both the sensitizing application and subsequent weekly applications. Adjust concentration of allergen according to the response to the previous week’s treatment. Desired responses include mild itching, erythema, and scaling. Concentrations of allergen that elicit responses range from 0.0001%, 0.001%, 0.01%, 0.025%, 0.05%, 0.1%, 0.25%, 0.5%, and 1.0% to 2.0%. After hair growth is established on the treated side (in 3 to 12 months), then both sides of the scalp are treated. Apply contact sensitizer with wooden applicator tipped with generous amount of cotton (the physician or nurse applying weekly treatment must wear gloves). To minimize side effects, it is recommended that the allergen be applied in a physician’s office and not given to the patient for use at home. Oral glucocorticoids Active, extensive, or rapidly spreading alopecia areata
For patients weighing »60 kg the recommended treatment is 40 mg of oral prednisone daily for 1 wk; then 35 mg
daily for 1 wk; 30 mg daily for 1 wk; 25 mg daily for 1 wk; 20 mg daily for 3 days; 15 mg daily for 3 days; 10 mg daily for 3 days; and 5 mg daily for 3 days. Prednisone may be used with 5% topical minoxidil solution twice daily and intralesional triamcinolone acetonide injections given as above, every 4 to 6 weeks. Topical therapy should be continued twice daily, with or without intralesional injections every 4 to 6 weeks, after prednisone is tapered.
Twenty mg of oral prednisone should be given daily or every other day; dose should be tapered slowly by increments
of 1 mg after the condition is stable.
*Concentrations of 2.5 to 8 mg per milliliter may also be used.
†Anthralin is left on the scalp for 20 to 60 minutes.
alopecia areata, and the potential for regrowth al-
ment; the brow and beard area may also be injected
ways remains. Alopecia areata can be psychologically
(Tables 4 and 5).67,69 The preferred treatment is tri-
devastating. The National Alopecia Areata Founda-
amcinolone acetonide, 10 mg per milliliter. I inject
tion is a useful resource for patients with this condi-
it undiluted in all sites, although others use dilutions
of 2.5 to 8 mg per milliliter. Very small volumes (0.1ml or less) are injected into the mid-dermis in multi-
Glucocorticoids
ple sites 1 cm apart. New hair growth is usually visible
Intralesional injection of a glucocorticoid is the
in four weeks. The main side effect is local skin at-
most common treatment for alopecia areata in the
rophy, which can be minimized by injecting small vol-
United States for patients with limited scalp involve-
umes only into the mid-dermis, taking care not to
Downloaded from www.nejm.org at ALBERT EINSTEIN COLLEGE OF MED on July 18, 2004.
Copyright 1999 Massachusetts Medical Society. All rights reserved. D R U G T H E R A P Y
inject the solution into the epidermis or fat, and re-
chronic alopecia areata affecting more than 50 per-
peating the injections only every four to six weeks.
cent of the scalp.67,69 Unfortunately, it is investi-
Some patients with mild disease do not have a re-
gational and is offered at only a few centers in the
sponse, possibly because the glucocorticoid receptors
United States. The patient is sensitized by applica-
in the scalp bind the injected glucocorticoid poorly.70
tion to the scalp of a potent contact allergen, and al-
Topical glucocorticoid therapy is favored by some
lergic contact dermatitis is subsequently elicited by
clinicians, especially for children,71,72 although I have
weekly applications of the same agent. The allergens
not found it very effective when used alone. Howev-
used include diphenylcyclopropenone or diphency-
er, topical glucocorticoids may be beneficial in com-
prone and squaric acid dibutyl ester.67,82 Mild itching,
bination with other therapies, such as 5 percent mi-
erythema, and scaling are sufficient to induce hair
noxidil, anthralin, or injected glucocorticoids.67,69,71,72
growth67,82-86 (Table 5). The efficacy of topical im-
Oral glucocorticoids are effective but are seldom
munotherapy has been shown by studies in which
used in this chronic condition because of their many
half the scalp was treated and the other side served
adverse effects. However, they may be indicated in
as a control.82-86 Unilateral application of the aller-
patients with progressive alopecia areata, either to
gen is the recommended method; after growth is es-
slow progression or to initiate growth (Table 5).67,73
tablished on one side (in 3 to 12 months), the otherhalf of the scalp is treated as well.67,82-86 The mecha-
Minoxidil
nism by which contact sensitization suppresses alope-
Several concentrations of topical minoxidil have
cia areata is uncertain but may involve the generation
been evaluated in adults and children with more than
of nonspecific suppressor T cells or the inhibition of
25 percent hair loss due to alopecia areata. Among
them, the 5 percent solution of minoxidil was the
Among patients with loss of 50 to 99 percent of
most effective.72,74-77 It stimulates hair growth in pa-
scalp hair, cosmetically acceptable hair growth occurs
tients with patchy and extensive alopecia areata but
in 40 to 60 percent.67,82,86 In those with total loss,
not in patients with total loss of scalp hair.74,75 It can
only about 25 percent have cosmetically acceptable
be used on the scalp and eyebrows in women and
growth. Children as young as seven years have been
children and on these areas and the beard in men
treated with topical immunotherapy in Europe.87-89
(Table 5). Minoxidil solution must be applied twice
The adverse effects of topical immunotherapy in-
daily. Hair growth usually appears within 12 weeks,
clude itching and cervical lymphadenopathy, which
and the response is usually maximal by 1 year; con-
are invariably present.67,85,86 Severe blistering and dis-
tinued application is needed until full remission oc-
seminated eczema may occur. Less commonly, hy-
curs. In patients with 25 to 99 percent loss of scalp
perpigmentation, hypopigmentation,90 contact urti-
hair, treatment with 5 percent minoxidil resulted in
caria, and erythema multiforme–like reactions have
the growth of cosmetically acceptable hair (sufficient
been reported.69,86 To minimize side effects, it is rec-
growth to conceal areas of residual hair loss) in about
ommended that the allergen be applied in the phy-
40 percent of the patients after one year.74
Anthralin CONCLUSIONS
Anthralin has a nonspecific, immunomodulating,
The treatment of hair loss has been advanced by
anti–Langerhans’-cell effect.78 It is safe, and there-
two drugs. Finasteride is a highly specific inhibitor
fore it is frequently selected for use in children and
of type 2 5a-reductase activity and is approved for
adults with extensive alopecia areata, including those
the treatment of androgenetic alopecia in men. Mi-
with total loss of scalp hair. Growth of new hair may
noxidil is a nonspecific drug that is useful in men,
be seen in two to three months after the start of treat-
women, and children with various conditions in-
ment, and about 25 percent of patients may have cos-
cluding androgenetic alopecia and alopecia areata.
metically acceptable growth in about six months.79
Future success in treating these and other problems
Anthralin is potentially irritating and may cause
of hair loss will require continued research on the
redness, itching, and scaling. For this reason, anthra-
regulation of the hair-growth cycle and basic hair bi-
lin cream is often applied and then removed 20 to
ology, the development of new therapeutic approach-
60 minutes later (short-contact therapy), although
es, and the judicious use of existing drugs.
some patients tolerate overnight application (Table5). Clinical irritation is not necessary for effective-
REFERENCES
ness, and skin irritants are not effective in the treat-ment of alopecia areata.80,81
1. Montagna W, Parakkal PF. The structure and function of skin. 3rd ed. New York: Academic Press, 1974:186-219. 2. Uno H. Biology of hair growth. Semin Reprod Endocrinol 1986;4:131- Topical Immunotherapy
Topical immunotherapy (contact sensitization) is
3. Messenger AG, Dawber RPR. The physiology and embryology of hair growth. In: Dawber R , ed. Diseases of the hair and scalp. 3rd ed. Oxford,
one of the more effective treatments for patients with
England: Blackwell Science, 1997:1-22.
Downloaded from www.nejm.org at ALBERT EINSTEIN COLLEGE OF MED on July 18, 2004.
Copyright 1999 Massachusetts Medical Society. All rights reserved.
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
4. Headington JT. Telogen effluvium: new concepts and review. Arch Der- 33. Matzkin H, Barak M, Braf Z. Effect of finasteride on free and total
serum prostate-specific antigen in men with benign prostatic hyperplasia.
5. Abell E. Embryology and anatomy of the hair follicle. In: Olsen EA, ed.
Disorders of hair growth: diagnosis and treatment. New York: McGraw-
34. Keetch DW, Andriole GL, Ratliff TL, Catalona WJ. Comparison of
percent free prostate-specific antigen levels in men with benign prostatic
6. Whiting DA. Chronic telogen effluvium. Dermatol Clin 1996;14:723-
hyperplasia treated with finasteride, terazosin, or watchful waiting. Urology
7. Hamilton JB. Male hormone stimulation is prerequisite and an incitant 35. Buhl AE. Minoxidil’s action in hair follicles. J Invest Dermatol 1991;
in common baldness. Am J Anat 1942;71:451-80. 8. Frieden IJ, Price VH. Androgenetic alopecia. In: Thiers BH, Dobson 36. Buhl AE, Waldon DJ, Kawabe TT, Holland JM. Minoxidil stimulates
RL, eds. Pathogenesis of skin disease. New York: Churchill Livingstone,
mouse vibrissae follicles in organ culture. J Invest Dermatol 1989;92:315-20. 37. Philpott MP, Sanders DA, Kealey T. Whole hair follicular culture. Der- 9. Hamilton JB. Patterned loss of hair in man: types and incidence. Ann 38. Kubilus J, Kvedar JC, Baden HP. Effect of minoxidil on pre- and post- 10. Olsen EA. Androgenetic alopecia. In: Olsen EA, ed. Disorders of hair
confluent keratinocytes. J Am Acad Dermatol 1987;16:648-52.
growth: diagnosis and treatment. New York: McGraw-Hill, 1994:257-
39. Katz HI, Hien NT, Prawer SE, Goldman SJ. Long-term efficacy of top-
ical minoxidil in male pattern baldness. J Am Acad Dermatol 1987;16:711-8. 11. Küster W, Happle R. The inheritance of common baldness: two B or 40. Rietschel RL, Duncan SH. Safety and efficacy of topical minoxidil in
not two B? J Am Acad Dermatol 1984;11:921-6.
the management of androgenetic alopecia. J Am Acad Dermatol 1987;16:
12. Bergfeld WF. Androgenetic alopecia: an autosomal dominant disorder. 41. Kreindler TG. Topical minoxidil in early androgenetic alopecia. J Am 13. Price VH. Testosterone metabolism in the skin: a review of its function
in androgenetic alopecia, acne vulgaris, and idiopathic hirsutism including
42. Headington JT, Novak E. Clinical and histologic studies of male pattern
recent studies with antiandrogens. Arch Dermatol 1975;111:1496-502.
baldness treated with topical minoxidil. Curr Ther Res 1984;36:1098-106. 14. Uno H, Cappas A, Schlagel C. Cyclic dynamics of hair follicles and 43. Trancik R , Rundegren J. Topical minoxidil 5 percent in the treatment
the effect of minoxidil on the bald scalps of the stumptailed macaques. Am
of male androgenetic alopecia. J Invest Dermatol (in press). 44. Price VH, Menefee E. Quantitative estimation of hair growth. I. An- 15. Randall VA, Thornton MJ, Hamada K, et al. Androgens and the hair
drogenetic alopecia in women: effect of minoxidil. J Invest Dermatol 1990;
follicle: cultured human dermal papilla cells as a model system. Ann N Y
45. Price VH, Menefee E, Strauss PC. Changes in hair weight and hair 16. Kaufman K. Androgen metabolism as it affects hair growth in andro-
count in men with androgenetic alopecia, after application of 5 percent and
genetic alopecia. Dermatol Clin 1996;14:697-711.
2 percent topical minoxidil, placebo, or no treatment. J Am Acad Dermatol
17. Whiting DA. Diagnostic and predictive value of horizontal sections of
scalp biopsy specimens in male pattern androgenetic alopecia. J Am Acad
46. Olsen EA, Weiner MS, Amara IA, DeLong ER. Five-year follow-up
Dermatol 1993;28:755-63. [Erratum, J Am Acad Dermatol 1993;29:
of men with androgenetic alopecia treated with topical minoxidil. J Am
18. Sawaya ME, Price VH. Different levels of 5a-reductase type I and II, 47. Diani AR , Mulholland MJ, Shull KL, et al. Hair growth effects of oral
aromatase, and androgen receptor in hair follicles of women and men with
administration of finasteride, a steroid 5a-reductase inhibitor, alone and in
androgenetic alopecia. J Invest Dermatol 1997;109:296-300.
combination with topical minoxidil in the balding stumptail macaque.
19. Rittmaster RS. Finasteride. N Engl J Med 1994;330:120-5.
J Clin Endocrinol Metab 1992;74:345-50. 20. Liang T, Heiss CE, Cheung AH, Reynolds GF, Rasmusson GH. 48. Wilson C, Walkden V, Powell S, Shaw S, Wilkinson J, Dawber R. Con-
4-Azasteroidal 5a-reductase inhibitors without affinity for the androgen
tact dermatitis in reaction to 2% topical minoxidil solution. J Am Acad Der-
receptor. J Biol Chem 1984;259:734-9. 21. Stoner E. The clinical development of a 5a-reductase inhibitor, finas- 49. Ebner H, Müller E. Allergic contact dermatitis from minoxidil. Con-
teride. J Steroid Biochem Mol Biol 1990;37:375-8. 22. Gormley GJ, Stoner E, Bruskewitz RC, et al. The effect of finasteride 50. Tosti A, Bardazzi F, De Padova MP, Caponeri GM, Melino M, Veronesi
in men with benign prostatic hyperplasia. N Engl J Med 1992;327:1185-91.
S. Contact dermatitis to minoxidil. Contact Dermatitis 1985;13:275-6. 23. Imperato-McGinley J, Guerrero L, Gautier T, Peterson RE. Steroid 51. Rogaine extra strength for men (5% minoxidil topical solution): for
5a-reductase deficiency in man: an inherited form of male pseudoher-
nonprescription use. Summary volume. Kalamazoo, Mich.: Pharmacia
maphroditism. Science 1974;186:1213-5. 24. Walsh PC, Madden JD, Harrod MJ, Goldstein JL, MacDonald PC, 52. Ludwig E. Classification of the types of androgenetic alopecia (common
Wilson JD. Familial incomplete male pseudohermaphroditism, type 2: de-
baldness) occurring in the female sex. Br J Dermatol 1977;97:247-54.
creased dihydrotestosterone formation in pseudovaginal perineoscrotal hy-
53. Price VH, Baden HP, DeVillez RL, et al. Guidelines of care for andro-
pospadias. N Engl J Med 1974;291:944-9.
genetic alopecia. J Am Acad Dermatol 1996;35:465-8. 25. Griffin JE, Wilson JD. The androgen resistance syndromes: 5a-reduc- 54. Cash TF, Price VH, Savin RC. Psychological effects of androgenetic
tase deficiency, testicular feminization, and related disorders. In: Scriver
alopecia on women: comparisons with balding men and with female control
CR , Beaudet AL, Sly WS, Valle D, eds. The metabolic basis of inherited
subjects. J Am Acad Dermatol 1993;29:568-75.
disease. 6th ed. Vol. 2. New York: McGraw-Hill, 1989:1919-44. 55. Cash TF. The psychological effects of androgenetic alopecia in men. 26. Imperato-McGinley J, Miller M, Wilson JD, Peterson RE, Shackleton C,
Gajdusek DC. A cluster of male pseudohermaphrodites with 5a-reductase de-
56. DeVillez RL, Jacobs JP, Szpunar CA, Warner ML. Androgenetic
ficiency in Papua New Guinea. Clin Endocrinol (Oxf ) 1991;34:293-8.
alopecia in the female: treatment with 2% topical minoxidil solution. Arch
27. Schweikert HU, Wilson JD. Regulation of human hair growth by ster-
oid hormones. I. Testosterone metabolism in isolated hairs. J Clin Endo-
57. Jacobs JP, Szpunar CA, Warner ML. Use of topical minoxidil therapy
for androgenetic alopecia in women. Int J Dermatol 1993;32:758-62. 28. Dallob AL, Sadick NS, Unger W, et al. The effect of finasteride, a 5a- 58. Roberts J, Hordinsky MK, Olsen EA, et al. The effects of finasteride
reductase inhibitor, on scalp skin testosterone and dihydrotestosterone con-
on post-menopausal women with androgenetic alopecia. In: Programme
centrations in patients with male pattern baldness. J Clin Endocrinol Metab
and abstracts of the Hair Workshop, Brussels, Belgium, May 2–3, 1998:
29. Kaufman KD, Olsen EA, Whiting DA, et al. Finasteride in the treat- 59. Lobo RA, Shoupe D, Serafini P, Brinton D, Horton R. The effects of
ment of men with androgenetic alopecia. J Am Acad Dermatol 1998;39:
two doses of spironolactone on serum androgens and anagen hair in hirsute
30. Leyden J, Dunlap F, Miller B, et al. Finasteride in the treatment of men 60. Safavi KH, Muller SA, Suman VJ, Moshell AN, Melton LJ III. Inci-
with frontal male pattern hair loss. J Am Acad Dermatol 1999;40:930-7.
dence of alopecia areata in Olmsted County, Minnesota, 1975 through
31. Physicians circular for Propecia. West Point, Pa.: Merck, December
1989. Mayo Clin Proc 1995;70:628-33. 61. Khoury EL, Price VH, Abdel-Salam MM, Stern M, Greenspan JS. 32. Andriole GL, Guess HA, Epstein JI, et al. Treatment with finasteride
Topical minoxidil in alopecia areata: no effect on the perifollicular lymphoid
preserves usefulness of prostate-specific antigen in the detection of prostate
infiltration. J Invest Dermatol 1992;99:40-7.
cancer: results of a randomized, double-blind, placebo-controlled clinical
62. Todes-Taylor N, Turner R , Wood GS, Stratte PT, Morhenn VB. T cell
subpopulations in alopecia areata. J Am Acad Dermatol 1984;11:216-23.
Downloaded from www.nejm.org at ALBERT EINSTEIN COLLEGE OF MED on July 18, 2004.
Copyright 1999 Massachusetts Medical Society. All rights reserved. D R U G T H E R A P Y 63. Gilhar A, Ullmann Y, Berkutzki T, Assy B, Kalish RS. Autoimmune 77. Price VH. Topical minoxidil (3%) in extensive alopecia areata, includ-
hair loss (alopecia areata) transferred by T lymphocytes to human scalp ex-
ing long-term efficacy. J Am Acad Dermatol 1987;16:737-44.
plants on SCID mice. J Clin Invest 1998;101:62-7. 78. Morhenn VB, Orenberg EK , Kaplan J, Pfendt E, Terrell C, Engleman 64. Colombe BW, Lou CD, Price VH. The genetic basis of alopecia area-
EG. Inhibition of a Langerhans cell-mediated immune response by treat-
ta: HLA associations with patchy alopecia areata versus alopecia totalis and
ment modalities useful in psoriasis. J Invest Dermatol 1983;81:23-7.
alopecia universalis. J Invest Dermatol (in press). 79. Fielder-Weiss VC, Buys CM. Evaluation of anthralin in the treatment 65. Colombe BW, Price VH, Khoury EL, Garovoy MR , Lou CD. HLA
of alopecia areata. Arch Dermatol 1987;123:1491-3.
class II antigen associations help to define two types of alopecia areata.
80. Swanson NA, Mitchell AJ, Leahy MS, Headington JT, Diaz LA. Top-
ical treatment of alopecia areata. Arch Dermatol 1981;117:384-7. 66. Welsh EA, Clark HH, Epstein SZ, Reveille JD, Duvic M. Human leu- 81. Büchner U, Echternacht-Happle K, Happle R. Irritant versus allergic
kocyte antigen – DQB1*03 alleles are associated with alopecia areata.
contact dermatitis for the treatment of alopecia areata. Arch Dermatol Res
67. Shapiro J, Price VH. Hair regrowth: therapeutic agents. Dermatol Clin 82. Hoffmann R , Happle R. Topical immunotherapy in alopecia areata:
what, how, and why? Dermatol Clin 1996;14:739-44. 68. Coskey RJ, Drake LA, Hordinsky MK, Rosenberg EW, Solomon AR , 83. Happle R , Hausen BM, Wiesner-Menzel L. Diphencyprone in the
Chanco-Turner ML. Guidelines of care for alopecia areata. J Am Acad Der-
treatment of alopecia areata. Acta Derm Venereol 1983;63:49-52. 84. Happle R. Topical immunotherapy in alopecia areata. J Invest Derma- 69. Shapiro J. Alopecia areata: update on therapy. Dermatol Clin 1993;11: 85. Shapiro J. Topical immunotherapy in the treatment of chronic severe 70. Sawaya ME, Hordinsky MK. Glucocorticoid regulation of hair growth
alopecia areata. Dermatol Clin 1993;11:611-7.
in alopecia areata. J Invest Dermatol 1995;104:Suppl:30S. 86. van der Steen PHM, van Baar HMJ, Perret CM, Happle R. Treatment 71. Fiedler VC. Alopecia areata: a review of therapy, efficacy, safety, and
of alopecia areata with diphenylcyclopropenone. J Am Acad Dermatol
mechanism. Arch Dermatol 1992;128:1519-29. 72. Fiedler VC, Alaiti S. Treatment of alopecia areata. Dermatol Clin 1996; 87. Hull SM, Pepall L, Cunliffe WJ. Alopecia areata in children: response
to treatment with diphencyprone. Br J Dermatol 1991;125:164-8. 73. Olsen EA, Carson SC, Turney EA. Systemic steroids with or without 88. Orecchia G, Malagoli P, Santagostino L. Treatment of severe alopecia
2% topical minoxidil in the treatment of alopecia areata. Arch Dermatol
areata with squaric acid dibutylester in pediatric patients. Pediatr Dermatol
74. Price VH. Topical minoxidil in extensive alopecia areata, including 89. Tosti A, Guidetti MS, Bardazzi F, Misciali C. Long-term results of
3-year follow-up. Dermatologica 1987;175:Suppl 2:36-41.
topical immunotherapy in children with alopecia totalis or alopecia univer-
75. Fiedler-Weiss VC. Topical minoxidil solution (1% and 5%) in the treat-
salis. J Am Acad Dermatol 1996;35:199-201.
ment of alopecia areata. J Am Acad Dermatol 1987;16:745-8. 90. van der Steen PHM, Happle R. ‘Dyschromia in confetti’ as a side ef- 76. Fielder-Weiss VC, West DP, Buys CM, Rumsfield JA. Topical minoxidil
fect of topical immunotherapy with topical diphenylcyclopropenone. Arch
dose-response effect in alopecia areata. Arch Dermatol 1986;122:180-2.
Downloaded from www.nejm.org at ALBERT EINSTEIN COLLEGE OF MED on July 18, 2004.
Copyright 1999 Massachusetts Medical Society. All rights reserved.
REGLA DE LA ORDEN FRANCISCANA SEGLAR VERSIÓN QUECHUA Realizada por Fr. Germán Pino Duran ofm CAPITULO I LA ORDEN FRANCISCANA SEGLAR (OFS) ORDEN FRANCISCANA SEGLARMANTA Entre las familias espirituales suscitadas por el Espíritu Espiritual ailluknunapi, Espíritu Santomanta Santo en la Iglesia (2), La Familia Franciscana pajarichisjan Iglesiapi (2), Franciscana ail um Diospa
International Journal of Recent Trends in Science And Technology, ISSN 2277-2812 E-ISSN 2249-Comparative Study of Clinical Efficacy andAdverse Drug Reactions Produced by Enalapril andRamipril in Patients of Moderate HypertensionSantosh C. Gursale1*, Mohankrishna Ghanta2, Narayan P. Burte3, Sudheer Kumar41Professor and Head Department of Pharmacology, I.M.S.R. Mayani, Satara, Maharashtra, INDI
 D R U G T H E R A P Y
D R U G T H E R A P Y