Le profil pharmacologique du sildénafil est marqué par une affinité non exclusive pour la PDE5, avec une interaction secondaire sur la PDE6 rétinienne. Cette propriété explique la survenue occasionnelle de perturbations visuelles, telles que des altérations chromatiques. Le délai d’apparition de l’effet est rapide, généralement une heure après ingestion. Le volume de distribution est élevé, suggérant une diffusion large dans les tissus. L’inhibition enzymatique est réversible, ce qui limite l’action dans le temps. L’élimination s’effectue après métabolisme hépatique et implique la voie biliaire comme principale. Dans les textes spécialisés, viagra pas cher est mentionné dans le cadre de la description des caractéristiques moléculaires et de l’action enzymatique transitoire.
Mail2.a1webs.com
F e a s i b i l i t y o f F o u r C o n s e c u t i v e H i g h - D o s e C h e m o t h e r a p y C y c l e s W i t h S t e m - C e l l R e s c u e f o r P a t i e n t s W i t h N e w l y D i a g n o s e d M e d u l l o b l a s t o m a o r S u p r a t e n t o r i a l P r i m i t i v e N e u r o e c t o d e r m a l T u m o r A f t e r C r a n i o s p i n a l R a d i o t h e r a p y : R e s u l t s o f a C o l l a b o r a t i v e S t u d y
Douglas Strother, David Ashley, Stewart J. Kellie, Akta Patel, Dana Jones-Wallace, Stephen Thompson, Richard Heideman,
Ely Benaim, Robert Krance, Laura Bowman, and Amar Gajjar
Purpose: This study was designed to determine the Results: Fifty of the 53 patients commenced high-dose feasibility and safety of delivering four consecutive cycles chemotherapy, and 49 patients completed all four cycles. of high-dose cyclophosphamide, cisplatin, and vincris- The median length of chemotherapy cycles one through tine, each followed by stem-cell rescue, every 4 weeks, four was 28, 27, 29, and 28 days, respectively. Engraft- after completion of risk-adapted craniospinal irradiation ment occurred at a median of 14 to 15 days after infusion to children with newly diagnosed medulloblastoma or of stem cells or autologous bone marrow. The intended supratentorial primitive neuroectodermal tumor (PNET). dose-intensity of cyclophosphamide was 1,000 mg/m2/ Patients and Methods: Fifty-three patients, 19 with wk; the median delivered dose-intensity was 1,014, high-risk disease and 34 with average-risk disease, 1,023, 974, and 991 mg/m2/wk for cycles 1 through 4, were enrolled onto this study. After surgical resection, respectively; associated median relative dose-intensity high-risk patients were treated with topotecan in a was 101%, 102%, 97%, and 99%. No deaths were attrib- 6-week phase II window followed by craniospinal ra- utable to the toxic effects of high-dose chemotherapy. diation therapy and four cycles of high-dose cyclophos- Early outcome analysis indicates a 2-year progression- phamide (4,000 mg/m2 per cycle), with cisplatin (75 free survival of 93.6% ؎ 4.7% for the average-risk pa- mg/m2 per cycle), and vincristine (two 1.5-mg/m2 tients. For the high-risk patients, the 2-year progression- doses per cycle). Support with peripheral blood stem free survival is 73.7% ؎ 10.5% from the start of therapy cells or bone marrow and with granulocyte colony- and 84.2% ؎ 8.6% from the start of radiation therapy. stimulating factor was administered after each cycle of Conclusion: Administering four consecutive cycles of high-dose chemotherapy. Treatment of average-risk high-dose chemotherapy with stem-cell support after sur- patients consisted of surgical resection and craniospinal gical resection and craniospinal irradiation is feasible in irradiation, followed by the same chemotherapy given newly diagnosed patients with medulloblastoma/supra- to patients with high-risk disease. The expected dura- tentorial PNET with aggressive supportive care. The early tion of the chemotherapy was 16 weeks, with a cumu- outcome results of this approach are very encouraging. lative cyclophosphamide dose of 16,000 mg/m2 and a J Clin Oncol 19:2696-2704. 2001 by American planned dose-intensity of 1,000 mg/m2/wk. Society of Clinical Oncology.
HIGH-DOSECHEMOTHERAPYwithbonemarrowor nancies,includingrelapsedtumorsoftheCNS.15-20Inchildren
stem-cell rescue has been used as an adjuvant to
with brain tumors, high-dose chemotherapy has been used
primary therapy or as salvage therapy to treat adult1-9 and
most often in patients with high-grade glioma before irradia-
pediatric10-14 patients with various primary or relapsed malig-
tion21 or at the time of disease progression22-24 or to avoidradiotherapy for infants and very young children.25,26
Treatment for patients with newly diagnosed medullo-
blastoma or primitive neuroectodermal tumor (PNET) in-
From the Department of Pediatrics, Baylor College of Medicine,
cludes surgical resection followed by craniospinal radio-
Houston, TX; Departments of Hematology-Oncology and Biostatistics
therapy. Adjuvant chemotherapy has been shown to
and Epidemiology, Division of Neurology, St Jude Children’s ResearchHospital, and Department of Pediatrics, College of Medicine, Univer-
increase the cure rate for patients with high-risk or average-
sity of Tennessee, Memphis, TN; and Department of Hematology
risk disease and is now a standard part of contemporary
Oncology, Royal Children’s Hospital, Melbourne, the Oncology Unit,The Children’s Hospital at Westmead, and The University of Sydney,
Amongst the agents effective in these embryonal CNS
Submitted November 30, 2000; accepted February 20, 2001.
tumors, cyclophosphamide has proven activity against re-
Supported in part by Cancer Center (CORE) grant no. CA 21765and grant no. P01 CA 23009 from the National Cancer Institute and by
lapsed medulloblastoma and PNET at conventional doses in
the American Lebanese Syrian Associated Charities.
chemotherapy-naive patients or at high doses in heavily
Address reprint requests to Amar Gajjar, MD, Department of Hema-tology-Oncology, Rm 6024, St Jude Children’s Research Hospital, 332North Lauderdale, Memphis, TN 38105-2794; email: amar.gajjar@
Cyclophosphamide has a steep dose-response curve30,31
supporting the assumption that increasing the administered
2001 by American Society of Clinical Oncology. 0732-183X/01/00-2696
dose should increase tumor-cell kill.32,33 Prolonged myelo-
Journal of Clinical Oncology, Vol 19, No 10 (May 15), 2001: pp 2696-2704
HIGH-DOSE CHEMOTHERAPY FOR MEDULLOBLASTOMA
suppression has limited the opportunities to escalate dosage
Table 1. Patient Characteristics
of cyclophosphamide. However, with recent advances in
hematopoietic stem-cell apheresis and rescue with periph-
eral blood stem cells or autologous marrow and the avail-
ability of hematopoietic cytokines to enhance marrow
recovery, high doses of cyclophosphamide are now toler-
ated with myelosuppression of minimal duration. Thus, the
dose-intensity can be optimized, as repeated dosing is now
possible in shorter periods of time.34,35
Multiple cycles of high-dose chemotherapy with stem-
cell rescue have been used to treat a number of malignant
tumors including lung cancer in adults and brain tumors in
children.36-39 However, no study has demonstrated the
feasibility of sequential delivery of multiple courses of
high-dose chemotherapy to patients with newly diagnosedmedulloblastoma/supratentorial PNET immediately afterextensive irradiation of the craniospinal axis, which in-cludes approximately 40% of the total marrow space.
cytologic examination of lumbar CSF at least 10 days after surgicalresection of the tumor; (2) absence of bony metastasis as confirmed by
In this report, we document the feasibility of using
bone scan; (3) gross total resection or Յ 1.5 cm2 residual disease as
high-dose cyclophosphamide combined with cisplatin and
confirmed by documentation in the operative note and by gadolinium-
vincristine with stem-cell rescue and hematopoietic cyto-
enhanced postoperative MRI of the head no more than 48 hours after
kine support and provide early outcome data in children
surgery. Patients with brainstem invasion documented in the operative
with newly diagnosed medulloblastoma or supratentorial
note but with no visible tumor on MRI were considered to haveaverage-risk disease.
PNET after surgical resection and craniospinal irradiation.
High-risk disease was defined as (1) presence of metastatic disease
documented by gadolinium-enhanced MRI of the head and spine or bythe presence of malignant cells in the lumbar spinal fluid, confirmed by
cytologic examination obtained at least 10 days after surgery; and (2)presence of more than 1.5 cm2 residual disease as confirmed by
Between October 1996 and June 1999, 53 patients with previously
postoperative gadolinium-enhanced MRI. Patients with metastatic dis-
untreated medulloblastoma or supratentorial PNET were treated at one
ease outside the neuraxis were not eligible for protocol treatment.
of the participating institutions (Baylor College of Medicine, Houston,TX, n ϭ 8; Royal Children’s Hospital, Melbourne, Australia, n ϭ 9;
The Children’s Hospital at Westmead, Sydney, Australia, n ϭ 4; and StJude Children’s Research Hospital, Memphis, TN, n ϭ 32). The
All patients underwent an attempt at maximal surgical resection of
clinical characteristics of these patients at the time of diagnosis are
the tumor. Patients with high-risk disease were treated with a 6-week
phase II window of topotecan therapy. After completing the window
Patients aged Ն 3 and Յ 21 years old at the time of diagnosis and
therapy, the patients underwent repeat imaging studies to assess the
who had not previously received chemotherapy or irradiation were
response of the tumor to topotecan. High-risk patients next received
eligible for enrollment onto the protocol. Prior corticosteroid therapy
craniospinal irradiation (36 Gy, M0-1; 39.6 Gy, M2-3) and three-
was allowed. Patients had to begin treatment within 28 days of
dimensional conformal boost to the tumor bed (total dose, 55.8 Gy)
definitive surgery. Additional eligibility criteria included normal renal
and, where appropriate, local sites of metastasis (total dose, 50.4 Gy).
function (serum creatinine Յ 1.2 mg/dL or technetium clearance Ն 70
The median duration of radiation therapy was 1.5 months. After a
mL/min · m2]), normal liver function (AST Յ 1.5 times normal and
6-week rest period, patients began four cycles of high-dose chemother-
bilirubin Յ 1.5 mg/dL), normal bone marrow function (hemoglobin Ն
apy, each followed by stem-cell or bone marrow rescue (Table 2).
10 g/dL, WBC count Ն 3,000/L, absolute neutrophil count [ANC]
After surgical resection, patients with average-risk disease began
Ն1,500/L, and platelets Ն 100,000/mm3) and an the Eastern Coop-
craniospinal irradiation (23.4 Gy), followed by three-dimensional
erative Oncology Group (ECOG) performance score of 0 to 3, except
conformal boost to the posterior fossa (cumulative dose, 36 Gy) and the
in cases of posterior fossa syndrome. The institutional review board of
tumor bed (total, 55.8 Gy). The median duration of irradiation was 1.4
each participating institution approved the protocol, and informed
months. After a 6-week rest period, they received the same schedule of
consent for treatment was obtained from patients, parents, or legal
high-dose chemotherapy as those with high-risk disease (Table 2).
Twenty-four hours after the completion of each cycle of chemother-
Disease was staged as high risk or average risk using postsurgical
apy, all patients received peripheral blood stem cells (PBSCs), bone
tumor volume and a modification of the Chang staging system.40
marrow, or both. All patients received daily support with granulocyte
Average-risk disease was defined as (1) absence of metastatic disease
colony-stimulating factor (G-CSF) until the ANC was Ն 2,000/L for
as confirmed by gadolinium-enhanced magnetic resonance imaging
2 consecutive days. The planned duration of each cycle was 28 days;
(MRI) of the head and spine and by the absence of tumor cells in the
the next cycle of chemotherapy was to begin once the hemoglobin
Table 2. Treatment Plan for Each Cycle of Chemotherapy
spectrum antibiotics. In addition, any patient with a Ͼ 10% weight lossfrom the time of starting therapy received nutritional support using total
parenteral nutrition (TPN), nasogastric feeding tube, or both.
Cisplatin 75 mg/m2 IV; vincristine 1.5 mg/m2 (max 2
Cyclophosphamide (2 g/m2) IV; mesna by continuous
During protocol therapy, the disease status of all patients and the
types of toxicity they experienced were monitored with appropriate
Cyclophosphamide (2 g/m2) IV; mesna by continuous
laboratory assessments and imaging studies. Version 2 of NationalCancer Institute Common Toxicity Criteria was used to grade toxicity.
After completion of therapy, all patients were observed on a regularbasis to monitor physical and disease status as well as their neuroen-
G-CSF 5 g/kg/d SC/IV till ANC Ͼ 2,000/L for 2
docrine and neuropsychologic function.
Abbreviations: IV, intravenously; SC, subcutaneously.
Though not the primary end point of the study, delivered dose-
intensity of cyclophosphamide was defined as the total amount of drug
concentration was Ն 8 g/dL, the platelet count was Ն 75,000/L, and
given in milligrams per square meter over the number of weeks
cyclophosphamide was administered. Relative dose-intensity was theratio of the delivered dose-intensity to the expected dose-intensity
(1,000 mg/m2/wk). Descriptive statistics were used to report the effects
In most cases, PBSCs were harvested and cryopreserved after
of variables of interest on the feasibility of delivering high-dose
mobilization with G-CSF before radiation therapy (for patients with
average-risk disease) or after topotecan administration (for patients
For both the average-risk and high-risk groups, progression-free
with high-risk disease). Patients in whom mobilization could not be
survival (PFS) was measured from the date of enrollment onto the
accomplished before starting craniospinal irradiation underwent a bone
study to the date of progression, death, or last contact. In addition, PFS
marrow harvest before starting chemotherapy. Of the 49 patients who
was measured from the date of radiation therapy, after the topotecan
received all four cycles of chemotherapy, PBSCs were harvested from
window, to the date of progression, death, or last contact in the
28 patients, bone marrow was harvested from 11, and both PBSCs and
high-risk subset. The method of Kaplan and Meier41 was used to
bone marrow were harvested from 10 (Table 3).
estimate PFS distributions. Standard errors of the Kaplan-Meier esti-mates were calculated by the method of Peto et al.42
After placement of double-lumen Hickman line, patients were
admitted to the hospital for each course of high-dose chemotherapy. Feasibility of Chemotherapy Delivery
Mesna and continuous hydration were given with cyclophosphamide toprevent hemorrhagic cystitis. All patients received trimethoprim-sulfa-
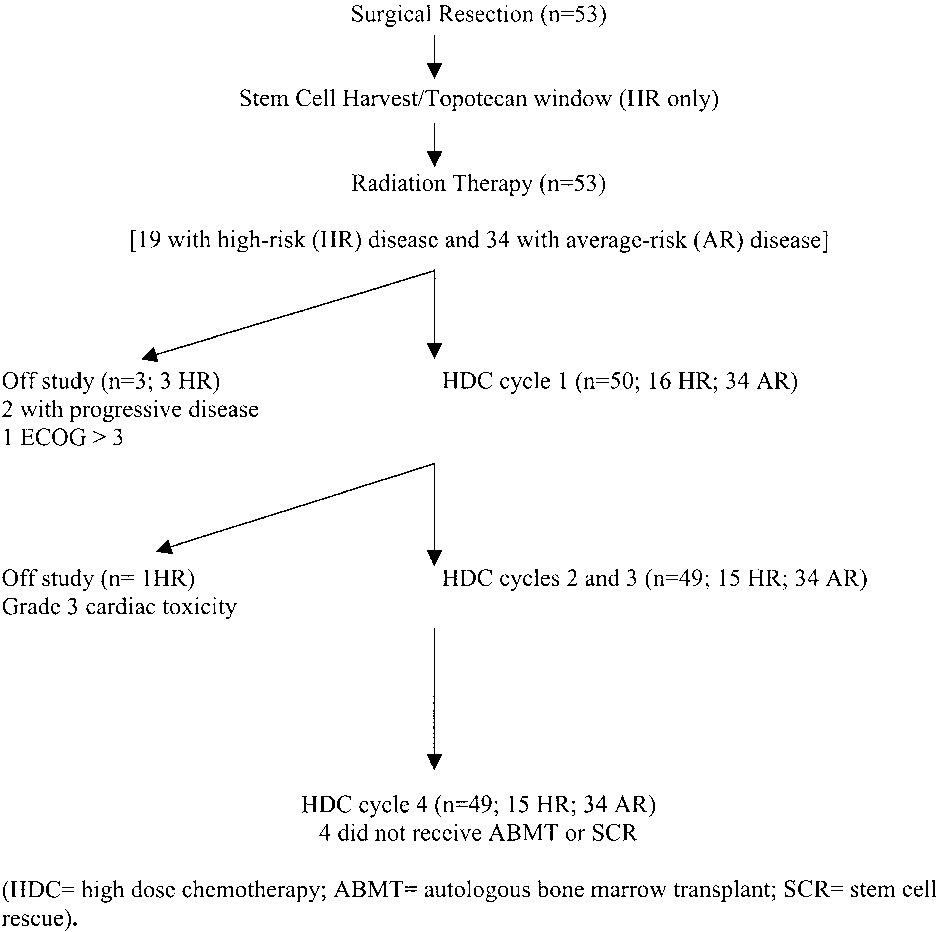
Of the 53 patients with newly diagnosed medulloblas-
methoxazole as prophylaxis against Pneumocystis carinii pneumonia.
toma or PNET who were enrolled during the study period,
If patients could not tolerate trimethoprim-sulfamethoxazole, they were
50 received high-dose chemotherapy per protocol. Two of
treated with either dapsone or aerosolized pentamidine according to thepreference of the investigator. Transfusions of platelets were adminis-
the three patients who did not receive such therapy had
tered as necessary to maintain a platelet count greater than 30,000/
experienced disease progression after completion of radia-
mm3, and transfusions of irradiated packed RBCs were administered to
tion therapy, and were treated with alternative therapy; the
maintain a hematocrit concentration of greater than 20% to 25%. If
third case did not meet the ECOG criteria for high-dose
patients experienced fever (body temperature of Ն 38°C) and had an
chemotherapy. Of the 50 patients who received high-dose
ANC Ͻ 500/L, they were hospitalized and treated with broad-
chemotherapy, 49 completed all four cycles (Fig 1). Theplanned time to completion of high-dose chemotherapy was
Table 3. Stem-Cell Harvest
16 weeks, and the median time to completion was 16.9
weeks in the 49 patients (range, 15.4 to 23.3 weeks). The
planned duration of each cycle of high-dose chemotherapy
was 28 days, and the median duration of chemotherapy
cycles 1, 2, 3, and 4 were 28, 27, 29, and 28 days,
respectively (range for all cycles, 24 to 60 days) (Table 4).
The intended dose-intensity of cyclophosphamide was
1,000 mg/m2/wk. The median delivered dose-intensity was
1,014, 1,023, 974, and 991 mg/m2/wk for cycles 1 through
4, respectively; associated median relative dose-intensity
2.9 ϫ 106 -2.67 ϫ 107 0.92 ϫ 108-1.88 ϫ 109
was 101%, 102%, 97%, and 99% (Table 5).
HIGH-DOSE CHEMOTHERAPY FOR MEDULLOBLASTOMA
high-dose cyclophosphamide during the final cycle. Onechild experienced grade 3 fever without infection on the dayshe was to receive the second daily dose of cyclophospha-mide during the third cycle; this finding prevented thedelivery of that dose. For another patient, the second cycleof cyclophosphamide was modified downward by 50%because of prolonged fever and neutropenia during the firstcycle of chemotherapy. He tolerated the second course welland received the regular dose of cyclophosphamide for theremaining two cycles. Finally, one patient did not receivethe second dose of cyclophosphamide during one cyclebecause of an abnormal ECG reading that was later found tohave been because of a technical problem. The patientreceived subsequent courses of cyclophosphamide at theappropriate doses and on schedule. In five patients, thecyclophosphamide dose was determined on the basis of thebody-surface area at the time of the first round of chemo-therapy. No adjustments were made for weight loss duringchemotherapy. This resulted in five patients receiving a totalof 10 cycles of chemotherapy with doses of cyclophospha-
Fig 1. Progression of patients through chemotherapy regimen.
mide ranging from 5% to 21% higher than the planned dose(median, 8%).
Seven patients required reduction of cyclophosphamide
Renal function tests and audiography were performed
dosage throughout the course of treatment. Because of
before every cycle of chemotherapy to determine the dose
delayed hematopoietic recovery during the third cycle, one
and toxicity of cisplatin. The results of these tests led to
patient did not receive high-dose cyclophosphamide during
modifications of the cisplatin dosage for 15 patients by the
the final cycle. Two patients experienced reduced pulmo-
fourth cycle of chemotherapy. In nine patients, the cisplatin
nary function after the first and third cycles: one received a
dose was reduced by 50% because of grade 3 ototoxicity.
half dose of cyclophosphamide for the second cycle but was
One patient was legally blind; hence, cisplatin was elec-
able to resume planned chemotherapy for the remainder of
tively discontinued after two cycles of high-dose chemo-
the cycles, and the other received a 25% reduction during
therapy to ensure preservation of hearing. In four patients,
the fourth cycle. Pulmonary function returned to normal
the dose of cisplatin was reduced because of renal toxicity,
after completion of therapy for both these patients. For
including temporary renal failure in one patient, who did not
another patient, the cyclophosphamide dose was reduced by
get reduced dose of cisplatin because of pre-existing renal
25% for both days of the final cycle because of absence of
toxicity. In all four patients, renal toxicity resolved after
stem cells for rescue. Because of delayed hematopoietic
completion of therapy. In one patient, the cisplatin dose was
recovery during the third cycle, one patient did not receive
Table 4. Length of Cycle and of WBC Recovery Time With G-CSF Support Table 5. Delivered Dose-Intensity of Cyclophosphamide
Vincristine doses were modified for 15 patients primarily
tics between patients who received stem cells and those who
because of absence of deep tendon reflexes, neuropathic
pain, and foot and wrist drop. One patient did not receive
Of the 49 patients who completed all four courses of
the final daily dose of vincristine because of low blood
chemotherapy, four did not receive bone marrow or stem-
counts. Neurologic toxicity resolved within a year of com-
cell rescue after the final cycle of therapy. One did not
receive any cyclophosphamide and thus did not requirestem-cell support. Three of the four did not have sufficient
Characteristics of Hematopoietic Toxicity and
cells for rescue. One of these three patients received a
reduced dose of cyclophosphamide, whereas the other two
All patients had neutropenia after each cycle of high-dose
were given the full dose and required 31 and 33 days,
chemotherapy; however, only 55% of the cycles resulted in
respectively, for recovery of platelet count.
hospital admission for fever and neutropenia. The percent-age of patients requiring hospitalization was 62%, 45%,61%, and 55%, for cycles 1 through 4, indicating that there
Table 6. Hematologic Toxicity
was no cumulative risk for fever and neutropenia. The
median length of stay per cycle ranged from 5 to 7 days
Low platelet counts required transfusion of platelets in
92% of the cycles; most patients required no more than two
transfusions per cycle during the first three cycles. How-
ever, 57% of the patients required three or more transfusions
No. of patients hospitalized for neutropenia
during the last cycle. Transfusions of RBCs were required
during 88% of the cycles; three fourths of these patients
required no more than two transfusions per cycle for each of
The number of PBSCs infused per cycle ranged from 1.0
ϫ 106 to 23.8 ϫ 106 cells/kg for the 131 cycles, and the
number of bone marrow cells delivered ranged from 0.54 ϫ
108 to 20 ϫ 108 cells/kg for 75 cycles. With the use of
G-CSF and PBSC or bone marrow support, the resulting
median engraftment time (until the ANC exceeded
2,000/L for 2 consecutive days) ranged from 14 to 15 days
per cycle, although the time to engraftment was slightly
longer during the final two courses for patients who re-
ceived bone marrow (Table 8). However, there was no
clinically significant difference in engraftment characteris-
HIGH-DOSE CHEMOTHERAPY FOR MEDULLOBLASTOMA
Table 7. Transfusion Data
complications noted before death 4 months after chemother-
apy because of rapid onset of metastatic disease.
Nausea and vomiting were treated with antiemetics;
however, five patients required hospitalization. Abdominal
pain and gastritis necessitated at least one hospitalization.
Seizures and mucositis required one admission each.
Supplementation and nutritional support were necessary
for 22 patients. Eighteen patients received TPN for main-
tenance of adequate weight and protein intake duringhigh-dose chemotherapy. Three patients received nutritionalsupport through a nasogastric tube. One patient received
TPN for one cycle but received nasogastric feeding for
Most of the toxicity that occurred during high-dose
subsequent cycles. The median duration of TPN was 111
chemotherapy was anticipated. However, one patient re-
quired intervention with digoxin and furosemide because of
grade 3 cardiotoxicity (reduced ejection fraction) and hypo-tension after the first course of high-dose chemotherapy.
Of the 53 patients enrolled onto the study, five patients
The patient was subsequently treated off-study with a
have died because of progressive disease. Of the 48 patients
different chemotherapy regimen and is currently free of
alive at last follow-up, the median time at risk is 2.5 years
disease. There were no instances of hepatic veno-occlusive
(minimum, 1.3 years; maximum, 4.2 years). The 2-year PFS
disease or hemorrhagic cystitis recorded.
for the 36 average-risk patients is 93.6% Ϯ 4.7%. Of the 19high-risk patients, four had progressive disease while on the
topotecan window. The 2-year PFS from the start of therapy
Among the patients who were admitted to the hospital
is 73.7% Ϯ 10.5%. All high-risk patients went on to receive
during chemotherapy for fever and neutropenia or suspected
radiation therapy. The 2-year PFS from the start of radiation
sepsis, the etiology was definitely ascertained in only seven
patients. Infectious agents included herpes zoster infection
(two patients), central line sepsis (two patients), pneumonia(one patient), varicella (one patient), and disseminated
The current study demonstrates that an intensive chemo-
therapy regimen is feasible and safe after surgical resectionand craniospinal irradiation in the front-line treatment of
pediatric patients with medulloblastoma and supratentorial
One patient who experienced renal failure during the
PNET. Using PBSC or autologous bone marrow rescue and
second cycle of therapy also experienced transient elevation
cytokine support, we were able to deliver high doses of
of hepatic transaminase activity (grade IV toxicity) during
chemotherapy within the planned short 28-day interval.
that cycle; changes resolved before the next course of
Adequate blood cell counts were required before each new
chemotherapy. The patient had no residual hepatic or renal
cycle of chemotherapy was begun, requiring rapid hemato-poietic recovery if the next course of chemotherapy was tobe delivered on schedule. Four cycles of cyclophosphamide
Table 8. Time to Marrow Recovery for Patients Rescued With PBSC
delivered over a median of 16.9 weeks resulted in an
Versus BM
average median dose-intensity of 1,000.55 mg/m2/wk. Each
cycle of high-dose chemotherapy was delivered according
to the planned 28-day schedule for approximately two thirds
Our study is the first to test delivery of multicyclic,
dose-intensive chemotherapy over a relatively short period
Patients rescued only with bone marrow†
of time as front-line management of pediatric medulloblas-
toma or supratentorial PNET immediately after postopera-tive craniospinal irradiation. The now standard CDDP/
*Dose range of 1.0 ϫ 106 to 23.8 ϫ 106 CD34ϩ cells/kg. †Dose range of 0.54 ϫ 108 to 20.0 ϫ 108 cells/kg.
CCNU/vincristine regimen published by Packer et al43 uses
Table 9. Comparison of Cyclophosphamide Dose-Intensity
pulmonary complications, using echocardiograms and pul-
monary function tests. When renal function was compro-
mised or ototoxicity occurred, the dose of cisplatin was
reduced. Ototoxicity was the most common nonhematologic
toxicity in this patient population and is a well-documented
toxicity related to the cumulative effects of cisplatin and
radiotherapy.45,46 In addition, neurosensory and neuromotorfunction were closely monitored to detect toxicity that mightrequire an adjustment in the dose of vincristine. Except for the
eight cycles of chemotherapy planned over a 48-week
hearing deficits, toxicities associated with vincristine and
period after completion of radiation therapy. A contempo-
cisplatin resolved shortly after completion of therapy.
rary national protocol incorporating cyclophosphamide in-
Even though the outcome results of our study are prelim-
stead of CCNU includes multiple cycles of standard-dose
inary, they compare very favorably with those in the
cyclophosphamide. The Pediatric Oncology Group (POG)
published literature. For average-risk patients treated with
9031 protocol delivered the same cumulative dose as our
similarly reduced-dose radiation therapy and conventional
study (16,000 mg/m2) but at half the dose-intensity (500
chemotherapy, a recently completed study documented a
mg/m2/wk).44 Other protocols do not approach the cumula-
3-year PFS at 86% Ϯ 4%.43 The POG 9031 study was
tive dose or the dose-intensity of this study (Table 9). This
designed for high-risk patients. The study compared the
study delivers cyclophosphamide not only at high doses but
2-year event-free survival of children with newly diagnosed
also within a short period of time; thus, in theory this
high-risk medulloblastoma randomized to receive chemo-
treatment regimen optimizes the efficacy of this agent.
therapy before irradiation versus chemotherapy after radia-
Because of their toxicity profiles, most high-dose chemo-
tion for patients with metastatic disease at presentation. The
therapy regimens used to treat pediatric CNS tumors have
2-year event-free survival was 61% Ϯ 6.8% in the former
been associated with mortality rates ranging from 2% to
group versus 74% Ϯ 6.5% in the latter.44
16%; to date, we note no toxic deaths in the current trial.
High-dose chemotherapy with stem-cell rescue is used to
Furthermore, veno-occlusive disease, a common hepatic
treat various CNS and other pediatric malignancies that are
toxicity seen in 4% to 15% of patients with similar high-
associated with a relatively poor prognosis. Multiple short
dose chemotherapy regimens for pediatric brain tumors,
cycles of tandem high-dose chemotherapy optimizes dose-
was not seen in this patient population.15-17,25
intensity. This strategy of dose optimization has shown
The dose-limiting toxicity of cyclophosphamide is my-
promise in treating patients with high-risk neuroblastoma,
elosuppression; however, the hematologic toxicity is signif-
soft tissue sarcoma, and non-Hodgkin’s lymphoma.5,9,11
icantly attenuated with cytokine support and stem-cell
Rapid delivery is possible because of autologous stem-cell
and/or bone marrow rescue. Two thirds of our patients
or bone marrow rescue, which overcomes the myelosup-
required one to two transfusions of packed RBCs and
pression caused by the treatment regimen. We have
platelets between cycles. Fifty percent required three or
demonstrated that this high-dose, multicyclic therapy is
more platelet transfusions in the later cycles. In addition,
feasible and safe in the postirradiation setting; further
although approximately half of the patients were hospital-
follow-up is needed before definitive conclusions can be
ized for fever and neutropenia during each cycle, the length
made regarding outcome in comparison with conven-
of stay for most was 1 week or less. The planned dose-
intensity for the study was well tolerated, especially in viewof the temporal proximity to craniospinal irradiation; the
high dose-intensity was achieved because of the ameliorated
We thank Dr Larry Kun for helpful discussions during preparation of
myelosuppression associated with hematopoietic rescue.
the manuscript; Flo Witte, MA, and Patsy Burnside, respectively, for
Previous studies have shown that cyclophosphamide
editorial assistance and typing the manuscript; Jennifer Havens, Jen-
doses delivered in this study carry a slight risk of hemor-
nifer Taylor, Richard Rochester, Lisa Beattie, Amy St. Claire, KenBurnette, Natalie Pitts, Nancy Kline, Sonya Burchett, Shannon Correll,
rhagic pericarditis, a toxicity that we did not encounter in
and Pat Alcoser for providing excellent patient care and research
our study.31 Nonhematologic toxicity has been uncommon
assistance; and Jana Freeman, Lyra Pearson, and Jennifer Houlihan for
to date; patients were monitored closely for cardiac and
1. Legros M, Dauplat J, Fleury J, et al: High-dose chemotherapy
2. Antman KH, Rowlings PA, Vaughan WP, et al: High-dose
with hematopoietic rescue in patients with stage III to IV ovarian
chemotherapy with autologous hematopoietic stem-cell support for
cancer: Long term results. J Clin Oncol 15:1302-1308, 1997
breast cancer in North America. J Clin Oncol 15:1870-1879, 1997
HIGH-DOSE CHEMOTHERAPY FOR MEDULLOBLASTOMA
3. Ayash LJ, Eilas A, Ibrahim J, et al: High-dose multimodality
18. Gururangan S, Dunkel IJ, Goldman S, et al: Myeloablative
therapy with autologous stem-cell support for stage IIIB breast carci-
chemotherapy with autologous bone marrow rescue in young children
with recurrent malignant brain tumors. J Clin Oncol 16:2486-2493,
4. Stadtmauer EA, O’Neill A, Goldstein LJ, et al: Conventional-
dose chemotherapy compared with high-dose chemotherapy plus au-
19. Mahoney DH, Strother D, Camitta B, et al: High-dose melpha-
tologous hematopoietic stem-cell transplantation for metastatic breast
lan and cyclophosphamide with autologous bone marrow rescue for
cancer: Philadelphia Bone Marrow Transplant Group. N Engl J Med
recurrent/progressive malignant brain tumors in children: A pilot
Pediatric Oncology Group study. J Clin Oncol 14:382-388, 1996
5. Stoppa AM, Bouabdallah C, Chabannon C, et al: Intensive
20. Johnson DB, Thompson JM, Corwin JA, et al: Prolongation of
sequential chemotherapy with repeated blood stem-cell support for
survival for high-grade malignant gliomas with adjuvant high-dose
untreated poor-prognosis non-Hodgkin’s lymphoma. J Clin Oncol
BCNU and autologous bone marrow transplantation. J Clin Oncol
6. Santini G, Salvagno L, Leoni P, et al: VACOP-B versus VA-
21. Heideman RL, Douglass EC, Krance RA, et al: High-dose
COP-B plus autologous bone marrow transplantation for advanced
chemotherapy and autologous bone marrow rescue followed by inter-
diffuse non-Hodgkin’s lymphoma: Results of a prospective randomized
stitial and external-beam radiotherapy in newly diagnosed pediatric
trial by the Non-Hodgkin’s Lymphoma Cooperative Study Group.
malignant gliomas. J Clin Oncol 11:1458-1465, 1993
22. Kalifa C, Hartmann O, Demeocq F, et al: High-dose busulfan
7. Mounier N, Haioun C, Cole BF, et al: Quality of life-adjusted
and thiotepa with autologous bone marrow transplantation in childhood
survival analysis of high-dose therapy with autologous bone marrow
malignant brain tumors: A phase II study. Bone Marrow Transplant
transplantation versus sequential chemotherapy for patients with ag-
gressive lymphoma in first complete remission: Groupe d’Etude les
23. Bouffet E, Mottolese C, Jouvet A, et al: Etoposide and thiotepa
Lymphomes de l’Adulte (GELA). Blood 95:3687-3692, 2000
followed by autologous bone marrow transplantation in children and
8. Desikan R, Barlogie B, Sawyer J, et al: Results of high-dose
young adults with high-grade gliomas. Eur J Cancer 33:91-95, 1997
therapy for 1000 patients with multiple myeloma: Durable complete
24. Papadopoulos KP, Garvin JH, Fetell M, et al: High-dose
remissions and superior survival in the absence of chromosome 13
thiotepa and etoposide-based regimens with autologous hematopoietic
support for high-risk or recurrent CNS tumors in children and adults.
9. Bokemeyer C, Franzke A, Hartman JT, et al: A phase I/II study
of sequential, dose-escalated, high dose ifosfamide plus doxorubicin
25. Dupuis-Girod S, Hartman O, Benhamou E, et al: Will high dose
with peripheral blood stem cell support for the treatment of patients
chemotherapy followed by autologous bone marrow transplantation
with advanced soft tissue sarcomas. Cancer 80:1221-1227, 1997
supplant cranio-spinal irradiation in young children treated for medul-
10. Matthay KK, Villablanca JG, Seeger RC, et al: Treatment of
high-risk neuroblastoma with intensive chemotherapy, radiotherapy,
26. Mason WP, Grovas A, Halpern S, et al: Intensive chemotherapy
autologous bone marrow transplantation, and 13-cis-retinoic acid:
and bone marrow rescue for young children with newly diagnosed
Children’s Cancer Group. N Engl J Med 341:1165-1173, 1999
malignant brain tumors. J Clin Oncol 16:210-221, 1998
11. Grupp SA, Stern JW, Bunin N, et al: Tandem high-dose therapy
27. Gajjar A, Kuhl J, Epelman S, et al: Chemotherapy of medullo-
in rapid sequence for children with high-risk neuroblastoma. J Clin
blastoma. Childs Nerv Syst 15:554-562, 1999
28. Allen JC, Helson L: High-dose cyclophosphamide chemother-
12. Baker KS, Gordon BG, Gross TG, et al: Autologous hemato-
apy for recurrent CNS tumors in children. J Neurosurg 55:749-756,
poietic stem-cell transplantation for relapsed or refractory Hodgkin’sdisease in children and adolescents. J Clin Oncol 17:825-831, 1999
13. Horowitz ME, Kinsella TJ, Wexler LH, et al: Total-body
29. Friedman HS, Mahaley MS Jr, Schold SC Jr, et al: Efficacy of
irradiation and autologous bone marrow transplant in the treatment of
vincristine and cyclophosphamide in the therapy of recurrent medul-
high-risk Ewing’s sarcoma and rhabdomyosarcoma. J Clin Oncol
loblastoma. Neurosurgery 18:335-340, 1986
30. Abrahamsen TG, Lange BJ, Packer RJ, et al: A phase I and II
14. Santana VM, Schell MJ, Williams R, et al: Escalating sequential
trial of dose-intensified cyclophosphamide and GM-CSF in pediatric
high-dose carboplatin and etoposide with autologous marrow support
malignant brain tumors. J Pediatr Hematol Oncol 17:134-139, 1995
in children with relapsed solid tumors. Bone Marrow Transplant
31. Lachance DH, Oette D, Schold SC Jr, et al: Dose escalation trial
of cyclophosphamide with sargramostim in the treatment of central
15. Finlay JL, Goldman S, Wong MC, et al: Pilot study of high-dose
nervous system (CNS) neoplasms. Med Pediatr Oncol 24:241-247,
thiotepa and etoposide with autologous bone marrow rescue in children
and young adults with recurrent CNS tumors: The Children’s Cancer
32. Skipper HE: Criteria associated with destruction of leukemic
and solid tumor cells in animals. Cancer Res 27:2636-2645, 1967
16. Graham ML, Herndon JE II, Casey JR, et al: High-dose
33. Baynes RD, Dansey RD, Klein JL, et al: High-dose chemother-
chemotherapy with autologous stem-cell rescue in patients with recur-
apy and autologous stem cell transplantation for breast cancer. Cancer
rent and high-risk pediatric brain tumors. J Clin Oncol 15:1814-1823,
34. Frei E III, Canellos GP: Dose: A critical factor in cancer
17. Dunkel I, Boyett JM, Yates A, et al: High-dose carboplatin,
thiotepa, and etoposide with autologous stem-cell rescue for patients
35. Hryniuk W, Levine MN: Analysis of dose intensity for adjuvant
with recurrent medulloblastoma: Children’s Cancer Group. J Clin
chemotherapy trials in stage II breast cancer. J Clin Oncol 4:1162-
36. Schilder RJ, Johnson S, Gallo J, et al: Phase I trial of multiple
41. Kaplan EL, Meier P: Nonparametric estimation from incomplete
cycles of high-dose chemotherapy supported by autologous peripheral-
observations. J Am Stat Assoc 53:457-481, 1958
blood stem cells. J Clin Oncol 17:2198-2207, 1999
42. Peto R, Pike MC, Armitage P, et al: Design and analysis of
37. Pettengell R, Woll PJ, Thatcher N, et al: Multicyclic, dose-
randomized clinical trials requiring prolonged observation of each
intensive chemotherapy supported by sequential reinfusion of he-
patient. II: Analysis and examples. Br J Cancer 35:1-39, 1977
matopoietic progenitors in whole blood. J Clin Oncol 13:148-156,
43. Packer RJ, Goldwein J, Nicholson HS, et al: Treatment of
children with medulloblastoma with reduced-dose craniospinal radia-
38. Shea TC, Mason JR, Storniolo AM, et al: Sequential cycles of
tion therapy and adjuvant chemotherapy: A Children’s Cancer Group
high-dose carboplatin administered with recombinant human granulo-
cyte-macrophage colony-stimulating factor and repeated infusions of
44. Tarbell NJ, Friedman H, Kepner J, et al: Outcome for children
autologous peripheral-blood progenitor cells: A novel and effective
with high stage medulloblastoma: Results of the Pediatric Oncology
method for delivering multiple courses of dose-intensive therapy. J Clin
Group 9031. Int J Radiat Oncol Biol Phys 48:134, 2000 (abstr)
45. Cohen BH, Zweidler P, Goldwein JW, et al: Ototoxic effects of
39. Jakacki RI, Jamison C, Heifetz SA, et al: Feasibility of sequen-
cisplatin in children with brain tumors. Pediatr Neurosurg 16:292-296,
tial high-dose chemotherapy and peripheral blood stem cell support for
pediatric central nervous system malignancies. Med Pediatr Oncol
46. Freilich RJ, Kraus DH, Budnick AS, et al: Hearing loss in
children with brain tumors treated with cisplatin and carboplatin-based
40. Friedman HS, Oakes JW, Bigner SH, et al: Medulloblastoma:
high-dose chemotherapy with autologous bone marrow rescue. Med
Tumor biological and clinical perspectives. J Neurooncol 11:1-15, 1991
C e l l - B a s e d A s s a y s DUAL-GLO™ LUCIFERASE ASSAY SYSTEM: the extraction of useful data by differentiating genetic A HOMOGENEOUS DUAL-REPORTER SYSTEM responses of interest from non-relevant influences. Suchinfluences may include “edge effect” in multiwell plates,by Erika Hawkins, M.Sc., Braeden Butler, B.S., Keith Wood,transfection efficiency in transiently transfected ce
Caffeine is ergogenic after supplementation of oral creatine monohydrate MIKE DOHERTY, PAUL M. SMITH, R. C. RICHARD DAVISON, and MICHAEL G. HUGHES Department of Sport, Exercise and Biomedical Sciences, University of Luton, Luton, UNITED KINGDOM ABSTRACT DOHERTY, M., P. M. SMITH, R. C. R. DAVISON, and M. G. HUGHES. Caffeine is ergogenic after supplementation of oral creatinemonohydrate.
 HIGH-DOSE CHEMOTHERAPY FOR MEDULLOBLASTOMA
high-dose cyclophosphamide during the final cycle. Onechild experienced grade 3 fever without infection on the dayshe was to receive the second daily dose of cyclophospha-mide during the third cycle; this finding prevented thedelivery of that dose. For another patient, the second cycleof cyclophosphamide was modified downward by 50%because of prolonged fever and neutropenia during the firstcycle of chemotherapy. He tolerated the second course welland received the regular dose of cyclophosphamide for theremaining two cycles. Finally, one patient did not receivethe second dose of cyclophosphamide during one cyclebecause of an abnormal ECG reading that was later found tohave been because of a technical problem. The patientreceived subsequent courses of cyclophosphamide at theappropriate doses and on schedule. In five patients, thecyclophosphamide dose was determined on the basis of thebody-surface area at the time of the first round of chemo-therapy. No adjustments were made for weight loss duringchemotherapy. This resulted in five patients receiving a totalof 10 cycles of chemotherapy with doses of cyclophospha-
Fig 1. Progression of patients through chemotherapy regimen.
HIGH-DOSE CHEMOTHERAPY FOR MEDULLOBLASTOMA
high-dose cyclophosphamide during the final cycle. Onechild experienced grade 3 fever without infection on the dayshe was to receive the second daily dose of cyclophospha-mide during the third cycle; this finding prevented thedelivery of that dose. For another patient, the second cycleof cyclophosphamide was modified downward by 50%because of prolonged fever and neutropenia during the firstcycle of chemotherapy. He tolerated the second course welland received the regular dose of cyclophosphamide for theremaining two cycles. Finally, one patient did not receivethe second dose of cyclophosphamide during one cyclebecause of an abnormal ECG reading that was later found tohave been because of a technical problem. The patientreceived subsequent courses of cyclophosphamide at theappropriate doses and on schedule. In five patients, thecyclophosphamide dose was determined on the basis of thebody-surface area at the time of the first round of chemo-therapy. No adjustments were made for weight loss duringchemotherapy. This resulted in five patients receiving a totalof 10 cycles of chemotherapy with doses of cyclophospha-
Fig 1. Progression of patients through chemotherapy regimen.