Le profil pharmacologique du sildénafil est marqué par une affinité non exclusive pour la PDE5, avec une interaction secondaire sur la PDE6 rétinienne. Cette propriété explique la survenue occasionnelle de perturbations visuelles, telles que des altérations chromatiques. Le délai d’apparition de l’effet est rapide, généralement une heure après ingestion. Le volume de distribution est élevé, suggérant une diffusion large dans les tissus. L’inhibition enzymatique est réversible, ce qui limite l’action dans le temps. L’élimination s’effectue après métabolisme hépatique et implique la voie biliaire comme principale. Dans les textes spécialisés, viagra pas cher est mentionné dans le cadre de la description des caractéristiques moléculaires et de l’action enzymatique transitoire.
Mjms2009-0068v.pmd
Maced J Med Sci electronic publication ahead of print, Ugwu et al. Antibiotic Resistance Patterns of Staphylococcus aureuspublished on November 03, 2009 as doi:10.3889/MJMS.1857-5773.2009.0068
Macedonian Journal of Medical Sciences. 2009 Dec 15; 2(4):XXX-XXX. doi:10.3889/MJMS.1857-5773.2009.0068
OPENACCESS Basic Research Antibiotic Resistance Patterns of Staphylococcus aureus Isolated from Nostrils of Healthy Human Subjects in a Southeastern Nigeria Locality
Malachy C Ugwu, Damian C Odimegwu*, Emmanuel C Ibezim, and Charles O Esimone
Division of Pharmaceutical Microbiology, Department of Pharmaceutics, Faculty of Pharmaceutical Sciences, University ofNigeria, Nsukka, 410001, Enugu State, NigeriaAbstract Key words: Background. Antibiotic resistant bacteria have been a source of ever-increasing therapeutic Staphylococcus aureus; multi-drug resist-
problem with profound health and socioeconomic pressures. Hence, continued surveillance
for bacteria susceptibility pattern is useful to determine the existing and future challenges of
Correspondence: Aim. This study was carried out to evaluate the resistance patterns of some community
isolates of Staphylococcus aureus to some conventional antibiotics within a locality in
Department of Pharmaceutics, Faculty ofPharmaceutical Sciences, University of
Material and methods. Preliminary characterizations of the plasmid DNA were also carried
Nigeria, Nsukka, 410001,Enugu State, Nigeria
Results. Here we show the results obtained, the resistances of the isolates to the antibiotics
were recorded in the following order: Flucloxacillin > Cotrimoxazole > Cephalexin > Chloram-
phenicol > Tetracycline > Minocycline ~ Clindamycin > Gentamicin ~ Erythromycin > Amoxicillin-
Clavulanic acid ~ Cloxacillin > Amoxicillin. The MIC results showed that the isolates were highly
susceptible to Clindamycin but resistant to Tetracycline. Clindamycin was equally shown toexert a relatively higher bactericidal activity among five other antibiotics tested. Preliminarycharacterization of eight (8) isolated bacteria plasmids from eight resistant bacteria isolatesgave mobilities (distances travelled) ranging from 3- 5 mm. These plasmids may be responsiblefor their observed high level of drug resistance. Early antibiotics susceptibility surveillanceexercises therefore helps ascertain and generate a good framework for effective manage-ment and control of resistant and multiple-drug resistant strains. Conclusion. The outcome of such surveillance exercises would both find usefulness in shaping the existing antibiotics prescription policies in order to achieve therapeutic endpoint and also help to slow down or prevent the emergence of multiple drug-resistant strains. Introduction
infections, and pneumonia (2-4). Staphylococcal in-
Staphylococcus aureus is the cause of a wide
fection leads to a worsening of some already existing
range of pyogenic infections, though also a commensal
superficial infections. Infection ranges from such su-
of human skin and nares. It has emerged over the past
perficial infection to deep infection as septicaemia,
several decades as a leading cause of hospital – and
making S. aureus an important subject of consistent
community – acquired infections (1). S. aureus has
studies (5). Infection rate from S. aureus is high and the
been found to be the most frequently isolated pathogen
recent increased recognition of community acquired
causing bloodstream infections, skin and soft tissue
infections has important clinical and pharmacologicalimplications for the health care provider (6). In recent
Maced J Med Sci. 2009 Dec 15; 2(4):XXX-XXX.
years, many isolates of S. aureus have evolved resist-
40C until used for further studies. All study activities
ance to both synthetic and traditional antimicrobial
were conducted at the Pharmaceutical Microbiology
chemotherapy and their prevalence outside the hospi-
unit of the Department of Pharmaceutics, University of
tal is of potential epidemiological threat (7-8). Resist-
ance to commonly available and affordable antibioticsposes a major concern in the management of bacterial
infections, especially in resource poor countries (9).
The culture media used in the study include,
Imprudent practices in the use of antibiotics in human
Nutrient broth (Oxoid, England), Mannitol salt agar
medicine and for prophylaxis in animal husbandry
(Oxoid, England) Nutrient agar (Fluka Spain) and
contribute significantly to the emergence of multidrug
Peptone water. Gram Staining reagents, buffer solu-
resistant (MDR) strains. In several studies worldwide,
tion, Tris-ethylenediamine tetra- acetic acid sodium
Staphylococcus aureus from normal flora seem to
sulfate (TENS), sodium acetate, Ethidium bromide
constitute an important reserviour of antimicrobial
and Bromo – phenol blue were all analar grade rea-
resistance gene (10) which can be transferred to other
microbial pathogens thus propagating the resistancetraits among microbial populations. The prevalence of
antibiotic – resistant Staphylococci at various skinsites in both healthy and hospitalized patients has
The following antibiotics used were obtained
received considerable attention because of the role of
from ABTEK, India: Amoxicillin – Clavulanic acid
these organisms as nosocomial pathogens especially
(AUG) 30 μg, Amoxicillin (AMX) 25 μg, Erythromycin
in immune-compromised host. Thus surveillance stud-
(ERY) 5 μg, Gentamicin (GEN) 10 μg, Cotrimoxazole
ies and monitoring of antibiotic resistance in Staphylo-
(COT) 25 μg, chloramphenicol (CHL) 30 μg, Cephalexin
coccus aureus isolated from the nostril of human
(CLX) 30 μg, Clindamycin (DAL) 2 μg, Flucloxacillin
subjects is clearly important as data obtained from
(FLX) 5 μg and Minocycline 30 μg. The following drugs
these exercises may be used to devise mechanisms
were also used: Gentamicin (80 mg/ml) (Gentalek)
for the appropriate use of antibiotics in chemothera-
Yugoslavia, Clindamycin (150 mg) (Dalacin CTM) Pfizer
peutics as well as help to stem the emergence and
USA, Flucloxacillin (Floxapen 250 mg) Beecham Eng-
subsequent spread of drug resistance among bacteria
land, Tetracycline (Tetraclin® 250 mg) Greenfield
populations. Moreover, beneficial retrospective stud-
ies on multi-drug resistance must put the availableconventional antibiotics in the area into consideration.
Based on this we embarked on this study to
Antibiotic sensitivity of the isolates was deter-
determine the resistance patterns of Staphylococcus
mined using previously established procedure (13). aureus to conventional antibiotics. This paper therefore
Briefly, the isolates were cultured in nutrient broth at
reports the prevalence of community-acquired MDR S.
370C for 24 h. Two (2) loopfuls of the suspension of each
aureus in Nsukka metropolis, Southeastern Nigeria.
isolate were inoculated into 20 ml of sterile molten agarin 10 cm diameter Petri dishes and mixed. The plateswere allowed to set and the antibiotic Sensitivity disc
Materials and Methods
(ABTEK, India) containing Amoxicllin – Clavulanate(AUG) 30 μg, Amoxicillin (AMX) 25 μg, Erythromycin
(ERY) 5 μg, Gentamicin (GEN) 10 μg, Cotrimoxazole
(COT) 25 μg, chloramphenicol (CHL) 30 μg, Cephalexin
Community strains of Staphylococcus aureus
(CLX) 30 μg, Clindamycin (DAL) 2 μg, Flucloxacillin
were isolated from nostrils of 100 healthy human
(FLX) 5 μg and Minocycline 30 μg.were aseptically
subjects within Nsukka metropolis, Enugu State (hav-
placed on their surfaces. The plates were incubated at
ing obtained their informed consent, and ethical ap-
370C for 24 h and the resultant inhibition zone diam-
proval) using sterile swab sticks. The population com-
eters (IZDs) were measured and recorded.
prised of 60 female and 40 male undergraduate stu-dents, all aged between 18 and 26 years. Samples
Determination of minimum inhibitory
were collected between July and August 2008 while
isolation and identification of the bacterial isolateswere performed according to standard bacteriological
The antibiotics, Gentamicin, Clindamycin, Tet-
techniques previously established (11-12). Thereafter
racycline, Cephalexin and Flucloxacillin were used for
all the S. aureus isolates were stored in agar slants at
this assay. Standard protocols employing agar dilution
Ugwu et al. Antibiotic Resistance Patterns of Staphylococcus aureus
method were used for this assay (13). Briefly, stock
poured into a gel tray. This was allowed for 20 mins to
solution of each antibiotic was made with distilled
solidity and the comb was carefully removed from the
water. Five serial dilutions (2-fold) of each stock solu-
gel. The gel carrier was removed from the pouring tray
tion were done. Exactly 1 ml from each serial dilution
and was placed in the gel electrophoresis box. A 250
was incorporated into 10 ml of molten nutrient agar and
ml TBE was used to fill the electrophoresis box until the
allowed to solidify. Each of the solidified plate was
divided into nine sections and labeled. One loopful ofeach suspension of the test organisms was streaked
Electrophoresis of the DNA Samples. Using
on the plates according to their numbering. The MIC of
micropipette, a 50 μL sample of DNA and 3 μL of
each antibiotic for each organism was recorded after
loading dye (ethidium bromide) were added together
overnight incubation at 370C as the lowest concentra-
and this was carefully mixed together by pipetting the
tion yielding no growth or a barely visible haze.
solutions up and down (16). Each sample was loadedcarefully into the gel wells, one sample per well and this
was placed on the gel box at the negative charge end
of the electrophoresis machine. Buffered water wasadded which sealed the agarose containing the sam-
This is an extension of the MIC Procedure,
ple DNA and acts as electrolyte by moving the current
since the agar plates showing no growth in the MIC
as well as the sample DNA towards the positive end for
tests were used for this test. Discs were cut from each
2 hrs with a voltage of 63 V. Thereafter the agarose
agar plate and transferred into corresponding container
containing the sample DNA was removed and allowed
of fresh nutrient medium (13) and incubated at 370C for
to drain off. With the aid of UV light, UV certified safety
48 h. Microbial growth or death were ascertained via
glasses and camera, a picture showing size and
turbidity of the medium. The minimal concentration of
movement of the sample DNA was taken to determine
the antibiotic that produced total cell death is the MBC.
the mobility in millimeter using a known sample stand-ard (16, 17). Plasmid Profile Studies Using Agarosegel ElectrophoresisExtraction of Plasmid DNA. Previously estab-
lished protocols were employed for this study (14-16).
Samples were collected from the 100 human
Selected resistant isolates were grown in a 5 ml double
subjects within the Nsukka community thus repre-
strength Mueller Hinton broth for 72 h at 370C. The 72
senting a collection of wild type strains of Staphyloco-
h grown cultures were centrifuged in a micro centrifuge
ccus aureus available within the assessed commu-
for 10 mins at 10,000 rpm to obtain pellets. Thesupernatant was gently decanted and the cell pelletswere vortexed for 5 min. Thereafter, 300 μg of Tris EDTA
(TE) buffer and 150 μL of 3.0 M sodium aqueous
acetate was added at pH 5.2 and was vortexed for 3mins to lyse the bacteria cell pellet. The samples werecentrifuged again for 2 min in a microcentrifuge (Biofuge,Biotra Bio-trade Hecrus Sepatech Co. Ltd USA) andthe supernatant was transferred to a fresh tube, mixedwell with 0.9 ml of 100% ethanol which had been pre-cooled to – 200C to precipitate the bacteria DNA. It wascentrifuged again for 2 min and the supernatant wasdiscarded. The pellet was rinsed twice with 1 ml of 70%ethanol and was dried under vacuum for 2 – 3 mins,after which it was resuspended in 20 - 40 μL of TE buffer
Preparation of Gel. A 1.0 g quantity of agarose
was dissolved in 100 ml of Tris Borate EDTA buffer
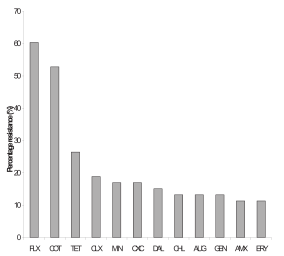
Figure 1: Antibiotic susceptibility rates among the S. aureus
(TBE) to form 1.0% gel. The agarose solution was
isolates. KEY: AUG = Amoxicillin – Clavulanic acid, AMX =
allowed to cool to a temperature of about 400C. There-
Amoxicillin, TET = Tetracycline, ERY = Erythromycin, COT =
after ethidium bromide was added and the mixture
Cotrimoxazole, CHL = Chloramphenicol, CLX = Cephalexin,CXC = Cloxacillin, DAL = Clindamycin, FLX = Flucloxacillin, MIN
Maced J Med Sci. 2009 Dec 15; 2(4):XXX-XXX.
nity. Fifty-three (53) isolates of Staphylococcus aureus
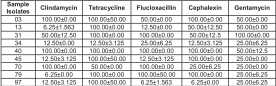
favourable activity of Clindamycin can be seen to
were recovered from the human subjects. They were all
reoccur here. This is followed by the microbiocidal
effects recorded by Flucloxacillin, Cephalexin, Gen-tamicin, and Tetracycline.
Figure 1 shows the antibiotic percentage resist-
ance profile among the tested isolates. From the
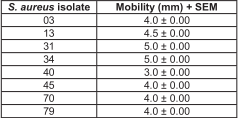
Table 3: Profile of plasmids isolated from drug-resistant
Figure, the resistances of the isolates of Staphyloco-S. aureus strains. ccus aureus to the antibiotics were in the followingorder: Flucloxacillin > Cotrimoxazole > Cloxacillin >Chloramphenicol > Tetracycline > Minocycline ~Clindamycin > Gentamicin ~ Erythromycin>Amoxicillin- Clavulanic acid ~ Cloxacillin > Amoxicillin. Thus, the highest resistance (> 60%) was recorded forFlucloxacillin while the least resistance (< 20%) wasrecorded for Amoxicillin. It is interesting to note herethat while very high resistance (least susceptibility)was displayed for Flucoxacillin, a penicillin, the leastresistance (highest susceptibility) was displayed byAmoxicillin which is another penicillin.
Preliminary characterization of the resistance
plasmids isolated from the resistant bacteria strains isshown in Table 3. Mobility values recorded ranges from
Table 1: Results of Minimum Inhibitory Concentration (MIC) in μg/ml + SEM. Discussion
Bacteria isolates were recovered from the nos-
trils of humans. These strains should be expected todisplay the typical community-type acquired geneticsusceptibility traits of the S. aureus microbial speciessince they are non-hospital strains and are relatively
Table 1 shows the minimum inhibitory concen-
unexposed to wide array of antimicrobial agents asso-
tration (MIC) profile of the various isolates to the
ciated with the hospital practice and environments. It
inhibitory activities of some representative antibiotics
is interesting to note (Figure 1) that while very high
standards. The very least MICs values of 3.125 μg/ml
resistance (least susceptibility) was displayed for
were recorded by Clindamycin against isolates 13, 34,
Flucoxacillin, a penicillin, the least resistance (highest
45, and 79 respectively. Moderate MICs were recorded
susceptibility) was displayed by Amoxicillin which is
by Flucloxacillin, Cephalexin, and Gentamicin in the
another penicillin. Penicillins are known to exert their
aforementioned order, while relatively more isolates
antimicrobial effect by inhibition of the synthesis of
(isolates 3, 13, 31, 40, 70, and 79 respectively)
peptidoglycan, which is a heteropolymeric component
recorded highest MICs of 100 μg/ml for Tetracycline
of the cell wall, which provides a rigid mechanical
thus representing a lower susceptibility outcome.
stability by virtue of its highly cross-linked lattice wallstructure (18-20), and the result of this inhibition is loss
Table 2: Results of Minimal biocidal concentration MBC
of bacteria cell rigidity and subsequent rupture or lysis
(μg/ml) + SEM.
of the bacteria cells (18). Hence it is very plausible toenvisage quite uniform pattern of susceptibility by thetest microorganisms to the members of the penicillinsfamily, albeit with only slightly varying differences. Moreover, the inherent weakness associated with thisantimicrobial class is resident in their β-lactam chemi-
cal ring nucleus which has been subject to attack byβ-lactamase enzymes produced by certain microor-
ganisms including some S. aureus strains (20, 21).
The result of the Minimum Bactericidal Concen-
tration (MBC) is presented in Table 2. Again, the more
Therefore, if the observed reduced susceptibility
Ugwu et al. Antibiotic Resistance Patterns of Staphylococcus aureus
of the S. aureus strains to Flucloxacillin is due to the
inhibition of bacteria cell wall synthesis were more
chemical disruptive activities of possible β-lactamase
effective against the S. aureus strains except for the
enzymes produced by the S. aureus strains, then, why
unusually high resistances recorded for Flucloxacillin
this trend does not seem to be replicated with regards
and Cloxacillin. This anomaly as have been explained
to Amoxicillin does appear to be very clear. This
from the foregoing may be related to a combination of
observation is further heightened when you consider
permeability/absorption factors and inherent degradative
the relatively poor activity of Amoxicillin-Clavulanic
enzyme-antibiotics SAR-resolved antimicrobial prop-
acid in comparison with Amoxicillin used alone.
erty of the antibiotics associated with the Penicillins/
Clavulanic acid present in the Amoxicillin-Clavulanic
β-lactam group. Nonetheless, this generally observed
acid complex is meant to afford protection to the β-
advantage of the Amoxicillin, Amoxicillin-Clavulanic
lactam chemical ring nucleus present in the Amoxicillin,
acid (Augmentin), and Cephalexin over the other anti-
and this protection should be expected to enhance the
microbial agents will be expected to find usefulness in
activity of Amoxicillin. Hence the Amoxicillin-Clavulanic
clinical practice requiring the use of antibiotics in the
acid complex should demonstrate clearly significantly
management of infections and epidemics caused by
higher susceptibility rates over the Amoxicillin alone. S. aureus strains, and this again underscore the needto always carry out a pre-treatment antimicrobial
Instead, a reverse trend is rather recorded from
susceptibility testing before embarking on antibiotics
the study thus suggesting that other mechanism(s)
treatment of infections in clinical settings.
may be responsible for these inconsistencies. Onelikely explanation for this phenomenon may be related
Blind treatment of infections with chemothera-
to permeability and absorption factors governing anti-
peutic agents should be discouraged since this could
biotic transfer across the microbial cells. It is quite
lead to treatment failure with the possible risk of
possible that the Amoxicillin-Clavulanic acid complex,
morbidity and mortality, as well as, a waste of eco-
which is a larger molecule than Amoxicillin, may
nomic resources. MIC results of antimicrobial agents
experience greater difficulty in permeability and overall
normally represent useful pre-clinical quantitative ana-
transport across the microbial cell wall/membrane
lytical parameter that finds prospective application in
barrier. Thus only relatively limited quantity may be
pre-clinical and clinical settings. Apart from the prac-
available to exert an antimicrobial effect since antibiot-
tical utility of MIC values as a means of cutoff points
ics must first penetrate the bacteria cells before they
demarcating between microbial species and strains on
can be mobilized to produce their antimicrobial effect.
the basis of the antimicrobial susceptibility rate, the
Secondly, varied and disproportionate structural hin-
possession of lower MICs by an antimicrobial agent is
drances introduced by molecular structural differences
quite suggestive of a higher inherent antimicrobial
among these antibiotics may serve to modulate the
property (22). Additionally, MIC values must synchro-
compulsory pre-activity structure-activity-relationship
nize with pharmacokinetic plasma and tissue distribu-
(SAR) between the β-lactamase enzymes and these
tion of the antibiotic to ensure that adequate amounts
antibiotics thereby rationalizing the overall degradative
of the antibiotic are made readily available at the sites
effect of these enzymes, and the consequent activities
of infection. It is therefore expected that lower MIC
values would enhance this outcome as well as help tolimit the clinical occurrence of unwanted drug side
Again, from the percentage resistance profile
effects since smaller but effective doses of the antibi-
results, the three (3) best agents showing relatively
otics could then be administered to patients in accord-
good susceptibility profile (Amoxicillin, Amoxicillin-
ance with pre-determined frequencies.
Clavulanic acid (Augmentin), and Cephalexin) are allbactericidal agents that produce their antimicrobial
Consequently, considering the MIC results gen-
effect through inhibition of bacteria cell wall synthesis.
erated (Table 1), Clindamycin (followed by Flucloxacillin,
The other agents (Chloramphenicol, Tetracycline,
Cephalexin, Gentamicin, and Tetracycline) seem to
Clindamycin, Minocycline, Gentamycin and Erythro-
present as the agent of choice for a general non-
mycin) all show quite moderate susceptibilityresistance
specific clinical treatment of infections caused by the
profile (< 40% > 20%) and they are known to exert their
isolated S. aureus strains within the examined Nsukka
antimicrobial activities through other means of inhibi-
community. This scheme may be extrapolated for
tion of bacteria protein synthesis (18). There appears
other neighbouring communities within the Enugu
therefore, a seeming correlation between the overall
State axis due to demographic relatedness of these
recorded antimicrobial activity and mode of action of
localities. However, since the MIC results also showed
the antibiotics used. It would generally appear from the
some wide bacteria-strain-specific variations, we would
results of this study that antimicrobial agents acting by
suggest that antibiotic treatments options should be
Maced J Med Sci. 2009 Dec 15; 2(4):XXX-XXX.
rather tailored to confront the specific S. aureus strain
carried out for different communities and geographical
involved on the basis of their favourable susceptibility
settings since the occurrence of antibiotic resistant
profile to the specific antibiotic to be used as deter-
strains can clearly vary across different environmental
mined by a proper laboratory analytical procedure.
settings depending on a host of various factors preva-
Given the Minimum Bactericidal Concentration (MBC)
lent in such environments that influence selection of
(Table 2), although all the antibiotics caused bacteria
development of antibiotic resistant strains.
cell death at concentration approaching 100 μg/ml this
however is quite far from the actual serum concentra-
In a conclusion, the high level of resistance
tion usually encountered at the doses employed in
among the isolates was found to be common with
clinical practice, and even though it is true that that the
commonly used antibiotics. The MIC and MBC results
prognosis of chemotherapeutic treatment of bacteria
showed that among the five antibiotics used,
infections is a combination of the antimicrobial prop-
Clindamycin had the best antibacterial activity. The
erty of the antibiotics used and the overall immunologi-
presence of plasmid DNA in the eight most resistant
cal dynamics occurring within the host; the MBC
isolates may be responsible for their observed high
results obtained still point to a very low susceptibility
antibiotic resistance. It is therefore recommended that
of a large proportion of the bacteria isolates to the
a good antibiotics use policy put in place as well as
antibiotics employed in the test. This development
ethical and rational prescription practices by clini-
raises a cause for genuine concern in the future of
cians, and every healthcare personnel involved in the
infectious diseases control of bacteria origin.
use of antibiotics in clinical and non-clinical settingswould help control and prevent the emergence of MDR
Agarose gel electrophoresis was employed for
the molecular characterization of the isolated plasmidsfrom the bacteria strains. Thus, the relative profiles ofthe DNA fragments and plasmids were characterized
References
on the basis of their comparative molecular weightsand speed of travel through the electrophoretic agarose
1. Lowy FD. Staphylococcus aureus infections. N Engl JMed. 1998;339(8):520-32. doi:10.1056/
system (23). The presence of some plasmid DNA in
the isolates corresponding to the reference standardDNA fragments suggests that their antimicrobial re-
2. Doern GV, Jones RN, Pfaller MA, Kugler KC, Beach ML.
sistance is possibly plasmid-mediated and as such
Bacterial pathogens isolated from patients with skin and
could be referred to as Resistance plasmids (R-factor).
soft tissue infections: frequency of occurrence and anti-
The isolated plasmids may be responsible for possibly
microbial susceptibility patterns from the SENTRY Anti-microbial Surveillance Program (United States and
mediating some or all of the expressed resistances of
Canada, 1997). SENTRY Study Group (North America).
the microorganisms. Further studies including resist-
Diagn Microbiol Infect Dis. 1999;34(1):65-72. doi:10.1016/
ance gene curing and actual sequencing of the isolated
plasmid genomes would be required to firmly establishthe role of the isolated plasmids in the observed
3. Pfaller MA, Jones RN, Doern GV, Sader HS, Kugler KC,
resistance patterns of the microorganisms. In bacte-
Beach ML. Survey of blood stream infections attributableto gram-positive cocci: frequency of occurrence and anti-
ria, the acquisition of resistance may be due to
microbial susceptibility of isolates collected in 1997 in
chromosomal mutations or through plasmids that are
the United States, Canada, and Latin America from the
often capable of transfer from one strain of organism to
SENTRY Antimicrobial Surveillance Program. SENTRY
another, even across the species barrier.
Participants Group. Diagn Microbiol Infect Dis. 1999;33(4):283-97. doi:10.1016/S0732-8893(98)00149-
The process of transfer and acquisition of resist-
ance determinants among microorganisms is a natu-ral, unstoppable phenomenon exacerbated by the
4. Sader HS, Jones RN, Gales AC, Winokur P, Kugler KC,
abuse, overuse and misuse of antimicrobials in the
Pfaller MA, Doern GV. Antimicrobial susceptibility patterns
treatment of human illness and in animal husbandry,
for pathogens isolated from patients in Latin Americanmedical centers with a diagnosis of pneumonia: analy-
aquaculture and agriculture agriculture (24-25). Moreo-
sis of results from the SENTRY Antimicrobial Surveillance
ver, the drugs to which the isolates were resistant to,
Program (1997). SENTRY Latin America Study Group.
are commonly used antibiotics in the studied environ-
Diagn Microbiol Infect Dis. 1998;32(4):289-301.
ment, thus the observed effects recorded in this study
doi:10.1016/S0732-8893(98)00124-2 PMID:9934546
must not be overlooked but should present a usefulbackground for rational use and prescription of antimi-
5. Komolafe AO, Adegoke AA. Incidence of Bacterial Sep-ticaemia in Ile-Ife, Nigeria. Malasian J Microbiol.
crobial agents. This kind of study should also be
Ugwu et al. Antibiotic Resistance Patterns of Staphylococcus aureus
6. Adegoke AA, Komolafe AO. Multi-drug resistant Staphy-
16. O Neal, J. The Biotechnology curriculum collections
lococcus aureus in clinical cases in Ile-Ife, Southwest
of the California community college, USA, 1998, pp 3 –
Nigeria. Int J Med Sci. 2009;1(3):68-72.
7. Daum RS, Seal JB. Evolving antimicrobial chemo-
17. Maniatis TE, Fritsch T, Sambrook J. Molecular clon-
therapy for Staphylococcus aureus infections: Our backs
ing: A laboratory manual Cold Spring Harbor Laboratory.
to the wall. Crit Care Med. 2001;29(4 Suppl):N92-6.
d o i : 1 0 . 1 0 9 7 / 0 0 0 0 3 2 4 6 - 2 0 0 1 0 4 0 0 1 - 0 0 0 0 7PMID:11292882
18. Hugo WC, Russel AD. Pharmaceutical Microbiology. 7th Edition United Kingdom BlackWell Science, 2004,
8. Kaplan SL, Hulten KG, Gonzalez BE, Hammerman WA,
Lamberth L, Versalovic J, Mason EO Jr. Three-year sur-veillance of community-acquired Staphylococcus aureus
19. Esimone CO, Iroha IR, Ibezim EC, Okeh CO, Okpana,
infections in children. Clin Infect Dis. 2005;40(12):1785-
EM. In vitro evaluation of the interaction between tea ex-
tracts and penicillin G against staphylococcus aureus. Afr J Biotechnol. 2006;5(11):1082-86.
9. McIver CJ, White PA, Jones LA, Karagiannis T,Harkness J, Marriott D, Rawlinson WD. Epidemic strains
20. Sabbath ID. Mechanism of resistance of beta-lactam
of Shigella sonnei biotype g carrying integrons. J Clin
antibiotics in strains of Staphylococcus aureus. Ann Int
Microbiol. 2002;40(4):1538-40. doi:10.1128/
21. Esimone CO, Adikwu MU. Susceptibility of some clini-
10. van den Bogaard AE, Stobberingh EE. Epidemiology
cal isolates of Staphylococcus aureus to bioactive col-
of resistance to antibiotics. Links between animals and
umn fractions from the lichen Ramalina farinacea (L.)
humans. Int J Antimicrob Agents. 2000;14(4):327-35.
Ach. Phytother Res. 2002;16(5):494-6. doi:10.1002/ptr.963
d o i : 1 0 . 1 0 1 6 / S 0 9 2 4 - 8 5 7 9 ( 0 0 ) 0 0 1 4 5 - X
22. Kahlmeter G, Brown DF, Goldstein FW, MacGowan
11. Cowan SI, Steel KJ. Cowan and Steel’s Manual for the
AP, Mouton JW, Osterlund A, Rodloff A, Steinbakk M,
identification of medical bacteria. Barrow GI and Feltman
Urbaskova P, Vatopoulos A. European harmonization of
RKA (eds) Univ. Press, Cambridge, 1993.
MIC breakpoints for antimicrobial susceptibility testing ofbacteria. J Antimicrob Chemother. 2003;52(2):145-8.
12. Baron EJ, Finegold SM. (eds) Bailey and Scott’s Di-
agnostic Microbiology. C. Mobby. Missouri, 1990.
23. Datta N, Hedges RW, Shaw EJ, Sykes RB, Richmond
13. Okore VC. Evaluation of chemical Antimicrobial
MH. Properties of an R factor from Pseudomonas
agents. Bacterial resistance to antimicrobial agents, Phar-
aeruginosa. J Bacteriol. 1971;108(3):1244-9.
maceutical microbiology, 2005, pp. 55-120.
14. Lech K, Brent R. Minipreps of plasmid DNA pp. 161-
24. Lexchin J. Promoting resistance? World Health Or-
164 In F. M. Ausubel, R. Brent R. E. Kingston. DD Moore.
ganization Essential Drug Monitor, Geneva, 2000, Nos.
J. G Seidman J. A Smith and K. struhl (Eds): Current
protocols in molecula Biology, John wiley & Sons NY,1987.
25. Stohr K. Problems from antimicrobial use in farming. World Health Organization: Essential Drugs Monitor, Ge-
15. Kraft R, Tardiff J, Krauter KS, Leinwand LA. Using
mini-prep plasmid DNA for sequencing double strandedtemplates with Sequenase. Biotechniques.
Maced J Med Sci. 2009 Dec 15; 2(4):XXX-XXX.
Policy No: AIP 01 Status: Policy - overall statement of the position, Version No: 0 intention and direction of the organization anchored in Date Approved: 01/03/11 the values and principles of the organization Review Date: 01/03/13 Policy on the Administration of Subcutaneous, Prefilled Syringes and Intramuscular Injections Written by: Clinical Practice Project Group
Rivista quadrimestrale di studi e ricerche sulle patologie psichiche da sostanze Vol. 2 – N° 2 Maggio-Agosto 2007 DIPENDENZE PATOLOGICHE Editoriale LA PROMESSA onlus Appunti per una geografia letteraria sul craving Rassegna Droghe psichedeliche e nuovi adolescenti - La ketamina Articolo Originale Validazione della Scheda dei Comportamenti Alimentari: SCA
 Ugwu et al. Antibiotic Resistance Patterns of Staphylococcus aureus
method were used for this assay (13). Briefly, stock
poured into a gel tray. This was allowed for 20 mins to
solution of each antibiotic was made with distilled
solidity and the comb was carefully removed from the
water. Five serial dilutions (2-fold) of each stock solu-
gel. The gel carrier was removed from the pouring tray
tion were done. Exactly 1 ml from each serial dilution
and was placed in the gel electrophoresis box. A 250
was incorporated into 10 ml of molten nutrient agar and
ml TBE was used to fill the electrophoresis box until the
allowed to solidify. Each of the solidified plate was
divided into nine sections and labeled. One loopful ofeach suspension of the test organisms was streaked
Electrophoresis of the DNA Samples. Using
on the plates according to their numbering. The MIC of
micropipette, a 50 μL sample of DNA and 3 μL of
each antibiotic for each organism was recorded after
loading dye (ethidium bromide) were added together
overnight incubation at 370C as the lowest concentra-
and this was carefully mixed together by pipetting the
tion yielding no growth or a barely visible haze.
Ugwu et al. Antibiotic Resistance Patterns of Staphylococcus aureus
method were used for this assay (13). Briefly, stock
poured into a gel tray. This was allowed for 20 mins to
solution of each antibiotic was made with distilled
solidity and the comb was carefully removed from the
water. Five serial dilutions (2-fold) of each stock solu-
gel. The gel carrier was removed from the pouring tray
tion were done. Exactly 1 ml from each serial dilution
and was placed in the gel electrophoresis box. A 250
was incorporated into 10 ml of molten nutrient agar and
ml TBE was used to fill the electrophoresis box until the
allowed to solidify. Each of the solidified plate was
divided into nine sections and labeled. One loopful ofeach suspension of the test organisms was streaked
Electrophoresis of the DNA Samples. Using
on the plates according to their numbering. The MIC of
micropipette, a 50 μL sample of DNA and 3 μL of
each antibiotic for each organism was recorded after
loading dye (ethidium bromide) were added together
overnight incubation at 370C as the lowest concentra-
and this was carefully mixed together by pipetting the
tion yielding no growth or a barely visible haze.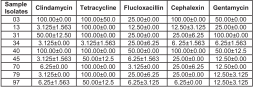
 nity. Fifty-three (53) isolates of Staphylococcus aureus
favourable activity of Clindamycin can be seen to
were recovered from the human subjects. They were all
reoccur here. This is followed by the microbiocidal
effects recorded by Flucloxacillin, Cephalexin, Gen-tamicin, and Tetracycline.
nity. Fifty-three (53) isolates of Staphylococcus aureus
favourable activity of Clindamycin can be seen to
were recovered from the human subjects. They were all
reoccur here. This is followed by the microbiocidal
effects recorded by Flucloxacillin, Cephalexin, Gen-tamicin, and Tetracycline.