Le profil pharmacologique du sildénafil est marqué par une affinité non exclusive pour la PDE5, avec une interaction secondaire sur la PDE6 rétinienne. Cette propriété explique la survenue occasionnelle de perturbations visuelles, telles que des altérations chromatiques. Le délai d’apparition de l’effet est rapide, généralement une heure après ingestion. Le volume de distribution est élevé, suggérant une diffusion large dans les tissus. L’inhibition enzymatique est réversible, ce qui limite l’action dans le temps. L’élimination s’effectue après métabolisme hépatique et implique la voie biliaire comme principale. Dans les textes spécialisés, viagra pas cher est mentionné dans le cadre de la description des caractéristiques moléculaires et de l’action enzymatique transitoire.
Mtdna.or.kr
Int J Colorectal Dis (2011) 26:1127–1134DOI 10.1007/s00384-011-1213-9
β-catenin and Her2/neu expression in rectal cancer:association with histomorphological response to neoadjuvanttherapy and prognosis
Uta Drebber & Martin Madeja & Margarete Odenthal & Inga Wedemeyer &Stefan P. Mönig & Jan Brabender & Elfriede Bollschweiler & Arnulf H. Hölscher &Paul M. Schneider & Hans P. Dienes & Daniel Vallböhmer
Accepted: 11 April 2011 / Published online: 3 May 2011
contained less than 50% vital tumor cells (n=14) and by
Background Neoadjuvant treatment strategies have been
Cologne grading system when resected specimens
developed to improve survival of patients with advanced
contained less than 10% vital tumor cells (n=15). Intra-
rectal cancer. Since mainly patients with major histopath-
tumoral β-catenin (nuclear/membranous) and Her2/neu
ological response benefit from this therapy, predictive and
(cytoplasmatic/membranous) expression was determined
prognostic markers are needed. We examined the associa-
by immunohistochemistry in pre- and post-therapeutic
tion of β-catenin and Her2/neu protein expression with
specimens and correlated with clinicopathologic parameters.
histopathologic response to neoadjuvant radiochemotherapy
Results A significant association was detected between pre-
and prognosis in patients with locally advanced rectal
therapeutic membranous β-catenin levels and response:
patients with a lower β-catenin protein expression showed
Methods Fifty-four patients (33 male; 21 female; median
significantly more often a major response compared with
age 60.4 years) with locally advanced rectal cancer were
patients having high intratumoral protein levels (p=0.011).
included in this study. All patients received a neoadjuvant
In addition, patients with a higher Her2/neu protein
radiochemotherapy (50.4 Gy, 5-FU) followed by surgical
expression showed a significant survival benefit compared
resection. Histomorphologic regression was evaluated by
with patients having low intratumoral protein levels (5-year
Dworak and Cologne staging system. Major response was
survival rate: 81% vs. low 41%; p=0.023).
defined by Dworak classification when resected specimens
Conclusions The pre-therapeutic β-catenin and Her2/neuprotein expression seem to be valuable predictive andprognostic markers in the multimodality treatment of
U. Drebber (*) M. Madeja M. Odenthal I. Wedemeyer
H. P. DienesInstitute of Pathology, University Hospital Cologne,Kerpener Str. 62,
Keywords Rectal cancer . Neoadjuvant therapy . Response
prediction . Prognosis . β-catenin . Her2/neu
S. P. Mönig J. Brabender E. Bollschweiler A. H. HölscherD. Vallböhmer
Department of General, Visceral and Cancer Surgery,University Hospital Cologne,
Rectal cancer has an incidence of over 70,000 patients
every year in Germany and leads to a mortality rate of
nearly 30,000 patients a year. A neoadjuvant “short-term”
or conventional chemoradiation is usually applied in
Department of Visceral and Transplantation Surgery,
rectal cancer patients falling into UICC (international
union against cancer) stages II and III [
with postoperative treatment, preoperative chemoradio-
Int J Colorectal Dis (2011) 26:1127–1134
therapy is associated with improved local control and
study. There were 33 male and 21 female with a median age
reduced toxicity ]. Histopathological evaluation of
of 60.4 years. None of the included patients received prior
tumor regression in the surgical specimen after preopera-
radiotherapy and/or chemotherapy. All patients received a
tive chemoradiotherapy is believed to be an objective
neoadjuvant radiochemotherapy (50.4 Gy, 5-FU) followed
prognostic factor allowing the identification of patients,
by surgical therapy. Restaging was done 2 to 3 weeks
who have minor or major benefit from multimodal therapy
following completion of radiochemotherapy, and surgical
–In fact, patients with major histological response
therapy was performed in all study patients. Pathological
to therapy have a significantly improved overall survival
examination before surgery comprised tumor typing and
]. However, only a subgroup of patients treated with
grading. The scientific protocol was approved by the local
preoperative chemoradiotherapy responds to treatment
]. The other subgroup consists of non-responders, who donot benefit from the therapy and who might be treated
Histomorphologic grading of tumor regression
differently. Currently, the selection of patients for neo-adjuvant preoperative therapy mainly depends on clinical
Morphologic assessment of tumor regression was per-
parameters including the stage of the disease. However,
formed by an objective histopathologic examination as
most of these parameters do not have a predictive impact
described previously by a staff pathologist who was blinded
on the therapy response. Thus, one major issue is the
for all other clinical data (U.D.) ]. The resected speci-
implication of prognostic molecular factors predicting
mens were fixed in formalin (10%), embedded in paraffin,
histopathological response to treatment.
and cut into slices (5 μm). The sections were stained with
Mutation and inactivation of the adenomatous polyposis
hematoxylin and eosin and used for both histopathological
coli tumor suppressor gene is a major event in early
staging according to the tumor–node–metastasis classifica-
colorectal carcinogenesis leading to stimulation of the Wnt/
tion system (Union Internationale Contre Le Cancer, 6th
β-catenin pathway which plays a central role in colorectal
edition, 2002 [and histomorphologic evaluation of the
tumor development ]. Overexpression of β-catenin
leads to stimulation of the Wnt/β-catenin pathway and
The extent of histomorphologic regression was evaluated
aberrant target gene expression with increase of cell
by two classification systems by using all available tumor
The proto-oncogene Her2/neu encodes a transmembrane
tyrosine kinase receptor and is normally expressed in
1. Grading system by Dworak: This grading system
epithelial cells –Overexpression has been described
divides into five categories: grade 0, no regression;
in various different tumors, including breast, lung, and
grade 1, dominant tumor mass with obvious fibrosis
colorectal cancer. This is a consequence of amplification of
and/or vasculopathy in 25% or less of the tumor
the Her2-gene which normally presents as a single copy in
mass; grade 2, dominantly fibrotic changes with few
normal cells. Amplification and overexpression result in
tumor cells or groups in 26–50% of the tumor mass
cellular proliferation. The significance of Her2/neu over-
(easy to find); grade 3, very few (difficult to find
expression and its impact on progression and prognosis of
microscopically) tumor cells in fibrotic tissue with or
without mucous substance; i.e., more than 50% of
In the present study, we determined the protein
tumor regression; grade 4, no tumor cells, only
expression of β-catenin and Her2/neu in advanced rectal
fibrotic mass (total regression or response). Regres-
cancer before and after multimodality treatment and
sion grades 3 and 4 were combined to major
correlated the intratumoral protein expression with
histomorphologic response (MaHR) and grades 0–2
clinicopathological parameters including the histopatho-
constituted minor histopathologic response (MiHR)
logical response in order to characterize molecular
2. Cologne grading system: This grading system divides
into four categories: grade 1, >50% vital residual tumorcells (VRTC); grade 2, 10% to 50% vital residual tumor
cells; grade 3, near complete regression with <10%VRTC; grade 4, complete regression (pathologic
complete remission and ypT0) according to the classi-fication described by Schneider et al. [Regression
Between 1996 and 2006, 54 patients with locally advanced
grades 3 and 4 were combined to MaHR and grades 1
rectal cancer (uT3/4Nx) were included in this retrospective
and 2 constituted MiHR as reported previously ].
Int J Colorectal Dis (2011) 26:1127–1134
staining, stromal staining was not considered. The degree ofexpression of all the markers was estimated by semiquan-
The investigation comprises immunohistochemical analyses
titative evaluation and described in percentage. The scores
of tumor tissue of pre-therapeutic biopsies and post-
used were 0, 0–5%; 1, 5–30%; 2, 30–60%, and 3, >60%. β-
catenin staining was analyzed in case of a positive nuclear
Immunohistochemical stainings were performed apply-
or membranous signal and Her2/neu in case of membranous
ing the DAKO EnVision System (DAKO, Hamburg,
Germany) according to manufacturer's instructions. β-catenin was detected by the β-catenin-specific monoclonalantibody from Becton-Dickinson Transduction Laboratories
(Heidelberg, Germany) (dilution, 1/100). Her2/neu wasdetected by a polyclonal antibody (DAKO, Hamburg,
Correlation analysis between the β-catenin or Her2/neu
protein expression and outcome parameters was assessed
Formalin-fixed and paraffin-embedded tissue was cut
using non-parametric tests using SPSS for Windows,
and deparaffinized according to standard histological
version 17.0G (Chicago, Illinois, USA). The Wilcoxon test
techniques. Pretreatment was performed in a microwave
was used for paired samples in the comparison of pre- and
using citrate buffer (pH 6.0) for 2×4 min at 600 W.
post-therapeutic protein expressions. The significance of
Endogenous peroxidase activity was blocked by methanol
the association between the dichotomized protein expres-
hydrogen peroxide (1 ml H2O2 30% ad 100 ml methanol).
sion and the clinical and histopathologic parameters was
Subsequently, primary antibodies were incubated in a
computed with the χ2 test and the Fisher's exact test when
humidity chamber overnight at 6°C. Secondary antibody
necessary. Kaplan–Meier analysis was used to determine
was incubated for 30 min at room temperature followed by
the probability of survival stratified for the histopathologic
DAKO Envsion and horseradish peroxidase 3-amino-9-
tumor regression and the post-therapeutic protein expres-
ethylcarbazole system for signal detection. Finally, the
sion. The level of significance is given for two-sided testing
nuclei were counterstained with hematoxylin and the tissues
Semiquantitative analysis All slides were evaluated by a
pathologist who had no access to patient data and clinicalstatus. Scoring was exclusively restricted to tumor cell
Clinical data of the study patients are summarized in Table
Int J Colorectal Dis (2011) 26:1127–1134
Histomorphologic regression grading and survival
Resected tumor tissues of 54 patients were evaluated. Fortypatients (74%) showed a minor histologic response and 14(26%) showed a major histologic response when using thegrading system by Dworak. In addition, 39 patients (72%)showed a minor histologic response and 15 (28%) showed amajor histologic response when using the Cologne gradingsystem. Kaplan–Meier survival curves demonstrated nocorrelation between major and minor histopathologicresponse (p=0.699; p=0.776; Table
There were 54 pre-therapeutic endoscopic biopsies andsurgical specimens available for the evaluation of nuclearand membranous β-catenin expression.
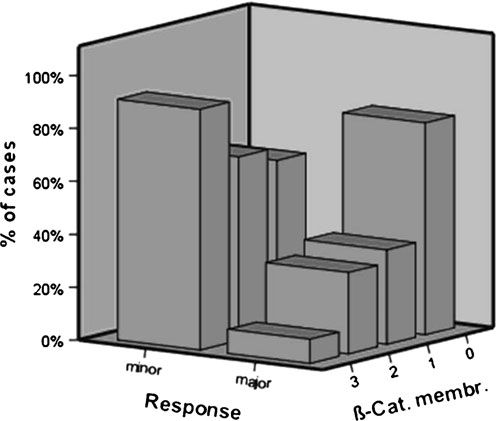
Fig. 1 Membranous β-catenin-expression within tumor cells in pre-therapeutic biopsies before neoadjuvant chemotherapy. Tumor regres-
Pre-therapeutic nuclear β-catenin expression Twenty two
sion is shown according to Cologne grading, data for Dworak grading
(40.7%) biopsies showed β-catenin expression grade 0, 22
(40.7%) biopsies showed grade 1, 6 (11.1%) biopsiesshowed grade 2, and 4 (7.4%) biopsies showed grade 3.
grade 0, 10 (20.4%) surgical specimens showed grade 1, 13
Pre-therapeutic membranous β-catenin expression Five
(26.5%) surgical specimens showed grade 2, and 12
(9.3%) surgical specimens revealed grade 0, 14 (25.9%)
(24.5%) surgical specimens showed grade 3.
revealed grade 1, 13 (24.1%) revealed grade 2, and 22surgical specimens showed grade 3 membranous β-catenin
Post-therapeutic membranous β-catenin expression Twenty
(40.8%) surgical specimens revealed grade 0, 7 (14.3%)grade 1, 6 (12.2%) revealed grade 2, and 16 (32.7%)
Post-therapeutic nuclear β-catenin expression Fourteen
surgical specimens showed grade 3 membranous β-catenin
(28.6%) surgical specimens showed β-catenin expression
Table 2 Pre- and post-therapeutic membranous β-catenin protein expression and clinicopathological parameters (data of the nuclear β-cateninexpression is not shown)
Int J Colorectal Dis (2011) 26:1127–1134
Regulation of β-catenin and Her2/neu protein expressionduring neoadjuvant therapy
There were 54 pre-therapeutic endoscopic biopsies andsurgical specimens available for the evaluation of cytoplas-
β-catenin and Her2/neu protein expression levels 0 to 3
matic and membranous Her2/neu expression.
were dichotomized into two categories: low-protein expres-sion (grades 0 and 1) and high-protein expression (grades 2
Pre-therapeutic cytoplasmatic Her2/neu expression Ten
and 3). There were 49 paired pretreatment biopsies and
(18.5%) biopsies showed Her2/neu expression grade 0, 9
(16.7%) biopsies showed grade 1, 12 (22.2%) biopsiesshowed grade 2, and 23 (42.6%) biopsies showed grade 3
Nuclear β-catenin expression Twelve (24.5%) cases
expressed downregulation, 24 (49.0%) expressed upregula-tion, and no difference in β-catenin protein expression was
Pre-therapeutic membranous Her2/neu expression Twenty
observed in 13 (26.5%) cases, respectively. The change in
seven (50.0%) biopsies revealed grade 0, 12 (22.2%)
nuclear β-catenin protein expression during neoadjuvant
revealed grade 1, 8 (14.8%) revealed grade 2, and 7
therapy was not statistically significant (p=0.075).
(13.0%) biopsies showed grade 3 membranous Her2/neuexpression.
Membranous β-catenin expression Twenty-six (53.1%)cases expressed downregulation, 9 (18.4%) expressed upre-
Post-therapeutic cytoplasmatic Her2/neu expression Eigh-
gulation, and no difference in β-catenin protein expression
teen (36.7%) surgical specimens showed Her2/neu ex-
was observed in 14 (28.5%) cases, respectively. The change in
pression grade 0, 8 (16.3%) surgical specimens showed
membranous β-catenin protein expression during neoadju-
grade 1, 10 (20.4%) surgical specimens showed grade 2,
vant therapy was not statistically significant (p=0.637).
and 13 (26.5%) surgical specimens showed grade 3(Table ).
Cytoplasmatic Her2/neu expression Twenty-five (51%)cases demonstrated downregulation, eleven (22.4%) dem-
Post-therapeutic membranous Her2/neu expression Thirty
onstrated upregulation, and no difference in Her2/neu
six (73.5%) surgical specimens revealed grade 0, 8 (16.3%)
protein expression was observed in 13 (26.6%) cases,
showed grade 1, 2 (4.1%) showed grade 2, and 3 (6.1%)
respectively. The change in cytoplasmatic Her2/neu protein
surgical specimens showed grade 3 membranous Her2/neu
expression during neoadjuvant therapy was not statistically
Table 3 Pre- and post-therapeutic cytoplasmatic Her2/neu protein expression and clinicopathological parameters (data of the membranous Her2/neu expression is not shown)
Int J Colorectal Dis (2011) 26:1127–1134
Membranous Her2/neu expression Twenty (40.8%) cases
biopsies and clinical/histopathologic parameters including
demonstrated downregulation, 10 (20.4%) demonstrated
histologic type, cT, ypT, ypN, grading, and histomorpho-
upregulation, and no difference in Her2/neu protein
logic regression grade and survival did not show any
expression was observed in 19 (38.8%) cases, respectively.
significant association (data not shown).
The change in membranous Her2/neu protein expressionduring neoadjuvant therapy was not statistically significant(p=0.131).
In this study, we performed a comprehensive analysis in 54
Pre-therapeutic β-catenin and Her2/neu protein expression
rectal cancer patients undergoing preoperative radiochemo-
therapy followed by surgical resection. We analyzed thepathological and clinical implications of tumor regression
Analysis of the correlation between dichotomized protein
and expression of β-catenin and Her2/neu before and after
expression of β-catenin and Her2/neu in pre-therapeutic
biopsies and clinical/histopathologic parameters including
Grading of histological changes in the resected specimen
histologic type, ypT, ypN, and grading did not show any
is a method to assess treatment response to preoperative
therapy. These changes include cytologic alterations of
However, a significant association was detected between
residual tumor and fibrotic changes at the site of previous
pre-therapeutic membranous β-catenin levels and response:
tumor. Whether regression grading is a prognostic factor in
patients with a lower β-catenin protein expression showed
rectal cancer has still to be clarified and is discussed
significantly more often a major response compared with
controversially. In our study, we used 4-point grading
patients having high intratumoral protein levels (p=0.04;
systems to assess the extent of tumor regression to
Table ; Fig. using the Cologne grading system while
discriminate major responders from minor responders [
there was a trend with the Dworak grading (p=0.09).
]. We found that tumor regression did not have a
In addition, a significant association was detected
significant influence on survival. Rödel et al. described in
between pre-therapeutic cytoplasmatic Her2/neu levels and
a series of 385 patients that a higher grade of tumor
survival: patients with a higher Her2/neu protein expression
regression predicted a better survival [Rosenberg et al.
showed a significant survival benefit compared with
found a significant improvement of overall survival for
patients having low intratumoral protein levels (5-year
histopathological tumor responders In contrast to these
survival rate: high, 81% vs. low 41%, p=0.023; Fig.
results, Jakob et al. did not see a significant influence oftumor regression on disease-free survival, merely an
Post-therapeutic β-catenin and Her2/neu protein expression
association of tumor regression with early treatment
efficacy is described ]. In a recent study, Lindebjerg etal. described that the combined assessment of lymph node
Analysis of the correlation between dichotomized protein
status and tumor response has a strong prognostic value in
expression of β-catenin and Her2/neu in post-therapeutic
locally advanced rectal cancer ]. Thus, pathologicallyassessed tumor response may be used as a surrogate endpoint for early determination of treatment efficacy ].
β-Catenin is considered as a potential oncogene in
sporadic colorectal cancer [, ]. The intracellulardistribution of β-catenin is of great importance for thedifferent functions of β-catenin and the subsequent behav-ior of tumor cells []. Previous data regarding anassociation of β-catenin expression with clinical andpathological parameters were contradictory. Our studyassessed a possible association of pre- and post- therapeuticnuclear/membranous β-catenin protein expression withhistomorphologic response and survival in patients withadvanced rectal cancer. We were able to demonstrate thatpre-therapeutic membranous β-catenin levels were signifi-cantly associated with major response to treatment. Patients
Fig. 2 Kaplan–Meier curves based on cytoplasmatic Her2/neu
with low pre-therapeutic intratumoral protein levels showed
expression within tumor cells in pre-therapeutic biopsies beforeneoadjuvant chemotherapy
significantly more often major response than patients
Int J Colorectal Dis (2011) 26:1127–1134
having high protein levels. However, the analysis between
our study, the change in membraneous and cytoplasmatic
dichotomized protein expression of membranous/nuclear β-
Her2/neu expression before and after therapy was not
catenin and clinical/histopathologic parameters including
histologic typing, cT, ypT, ypN, and grading did not show
In conclusion, in our study, a low pre-therapeutic
any significant association in our study. Several studies
membranous β-catenin protein expression in our cohort of
have demonstrated that immunostaining for β-catenin has
patients with advanced rectal cancer treated with neo-
shown increased membraneous/cytoplasmatic staining in
adjuvant radiochemotherapy was associated more often
85% of colorectal cancers and increased nuclear staining in
with a major histological response. Patients with a higher
20–26% of tumors [Our study shows similar results
cytoplasmatic Her2/neu protein expression showed a
with strong membraneous staining in 64% (score 2 and 3)
significant survival benefit compared with patients having
and strong nuclear staining in 18% (score 2 and 3).
low cytoplasmatic protein expression. There was no
Different conclusions have been reached regarding β-
correlation of the regulation of β-catenin and Her2/neu
catenin expression as a prognostic marker in colorectal
protein expression during neoadjuvant therapy with clinical
carcinoma. In our study, there was no correlation between
and histopathological data. Whether our results represent a
β-catenin immunostaining and survival. Fernebro et al.
causal relationship, a surrogate phenomenon, or even a
reported a correlation of loss of membranous β-catenin
statistical bias can only be determined in larger trials.
staining and distant metastases and the reduced/absentmembranous β-catenin expression as an independent
This work was supported by Cologne University
prognostic marker in colorectal carcinoma [In anearlier study, Günther et al. did not find any associationbetween the nuclear overexpression of β-catenin and the
development of metachronous metastases ]. Moreover,Baldus et al. did not find correlations between nuclear β-
1. Bosset JF, Calais G, Daban A, Berger C, Radosevic-Jelic L,
catenin expression and important clinicopathological vari-
Maingon P, Bardet E, Pierart M, Briffaux A (2004) Preoperative
ables [Little is known about the regulation of β-catenin
chemoradiotherapy versus preoperative radiotherapy in rectal
expression before and after neoadjuvant therapy. In our
cancer patients: assessment of acute toxicity and treatmentcompliance. Report of the 22921 randomised trial conducted by
study, the change in nuclear and membraneous β-catenin
the EORTC Radiotherapy Group. Eur J Cancer 40:219–224
expression before and after therapy was not statistically
2. Kim JS, Hur H, Kim NK, Kim YW, Cho SY, Kim JY, Min BS,
Ahn JB, Keum KC, Kim H, Sohn SK, Cho CH (2009) Oncologic
Her2neu is a therapeutic target in a variety of malignan-
outcomes after radical surgery following preoperative chemo-radiotherapy for locally advanced lower rectal cancer: abdomi-
cies. Her2 overexpression in breast cancer is known to be
noperineal resection versus sphincter-preserving procedure. Ann
associated particularly with aggressive disease and poor
prognosis [In addition to its well-established role in
3. Minsky BD (2009) Is preoperative chemoradiotherapy still the
breast cancer, Her2 overexpression and amplification has
treatment of choice for rectal cancer? J Clin Oncol 27:5115–5116
4. Pasetto LM (2005) Preoperative versus postoperative treatment for
also been demonstrated in subsets of numerous other
locally advanced rectal carcinoma. Future Oncol 1:209–220
human cancers and is associated with poorer prognosis in
5. Roh MS, Colangelo LH, O'Connell MJ, Yothers G, Deutsch M,
many of these tumors [Our results with staining for
Allegra CJ, Kahlenberg MS, Baez-Diaz L, Ursiny CS, Petrelli NJ,
HER 2 in colorectal carcinoma are consistent with other
Wolmark N (2009) Preoperative multimodality therapy improvesdisease-free survival in patients with carcinoma of the rectum:
reports in the literature. In the pre-therapeutic biopsies, we
found a membranous staining in 27% of the biopsies (score
6. Sauer R, Becker H, Hohenberger W, Rodel C, Wittekind C,
2 and 3). Kluftinger et al. detected weak and moderate
Fietkau R, Martus P, Tschmelitsch J, Hager E, Hess CF, Karstens
staining in 38% of the cases ]. Natali and coworkers
JH, Liersch T, Schmidberger H, Raab R (2004) Preoperativeversus postoperative chemoradiotherapy for rectal cancer. N Engl
demonstrated membranous staining in 29% of colorectal
tumors []. In line with Kluftinger et al., our data
7. Sebag-Montefiore D, Stephens RJ, Steele R, Monson J, Grieve R,
demonstrate no association between positive staining and
Khanna S, Quirke P, Couture J, de Metz C, Myint AS, Bessell E,
clinical/histopathologic parameters, including histologic
Griffiths G, Thompson LC, Parmar M (2009) Preoperativeradiotherapy versus selective postoperative chemoradiotherapy in
type, cT, ypT, ypN, and grading ]. However, we found
patients with rectal cancer (MRC CR07 and NCIC-CTG C016): a
a significant association between pre-therapeutic cytoplas-
multicentre, randomised trial. Lancet 373:811–820
matic Her2/neu levels and survival: patients with a higher
8. Guillem JG, Chessin DB, Cohen AM, Shia J, Mazumdar M,
Her2/neu protein expression showed a significant survival
Enker W, Paty PB, Weiser MR, Klimstra D, Saltz L, Minsky BD,Wong WD (2005) Long-term oncologic outcome following
benefit compared with patients having low intratumoral
preoperative combined modality therapy and total mesorectal
protein levels. Little is known about the regulation of
excision of locally advanced rectal cancer. Ann Surg 241:829–
Her2/neu expression before and after neoadjuvant therapy. In
Int J Colorectal Dis (2011) 26:1127–1134
9. Rosenberg R, Nekarda H, Zimmermann F, Becker K, Lordick F,
24. Rödel C, Martus P, Papadoupolos T, Fuzesi L, Klimpfinger M,
Hofler H, Molls M, Siewert JR (2008) Histopathological
Fietkau R, Liersch T, Hohenberger W, Raab R, Sauer R, Wittekind
response after preoperative radiochemotherapy in rectal carci-
C (2005) Prognostic significance of tumor regression after
noma is associated with improved overall survival. J Surg
preoperative chemoradiotherapy for rectal cancer. J Clin Oncol
10. Horisberger K, Hofheinz RD, Palma P, Volkert AK, Rothenhoefer
25. Jakob C, Liersch T, Meyer W, Baretton GB, Schwabe W, Hausler
S, Wenz F, Hochhaus A, Post S, Willeke F (2008) Tumor response
P, Kulle B, Becker H, Aust DE (2006) Prognostic value of
to neoadjuvant chemoradiation in rectal cancer: predictor for
histologic tumor regression, thymidylate synthase, thymidine
surgical morbidity? Int J Colorectal Dis 23:257–264
phosphorylase, and dihydropyrimidine dehydrogenase in rectal
11. Fearon ER, Vogelstein B (1990) A genetic model for colorectal
cancer UICC Stage II/III after neoadjuvant chemoradiotherapy.
12. de Lau W, Barker N, Clevers H (2007) WNT signaling in the
26. Lindebjerg J, Spindler KL, Ploen J, Jakobsen A (2009) The
normal intestine and colorectal cancer. Front Biosci 12:471–491
prognostic value of lymph node metastases and tumour regression
13. Kitisin K, Mishra L (2006) Molecular biology of colorectal
grade in rectal cancer patients treated with long-course preoper-
cancer: new targets. Semin Oncol 33:S14–S23
ative chemoradiotherapy. Colorectal Dis 11:264–269
14. Yang VW (1999) The molecular genetics of colorectal cancer.
27. Brabletz T, Kirchner T (2003) Morphogenetic aspects of colorectal
15. Su LK, Vogelstein B, Kinzler KW (1993) Association of the APC
28. Savas B, Ensari A, Percinel S, Kuzu I, Kuzu MA, Bektas M,
tumor suppressor protein with catenins. Science 262:1734–1737
Cetinkaya H, Kursun N (2007) The significance of beta-catenin,
16. Rubinfeld B, Souza B, Albert I, Muller O, Chamberlain SH,
E-cadherin, and P-cadherin expressions in neoplastic progression
Masiarz FR, Munemitsu S, Polakis P (1993) Association of the
of colorectal mucosa: an immunohistochemical study. Acta
APC gene product with beta-catenin. Science 262:1731–1734
17. Ochs AM, Wong L, Kakani V, Neerukonda S, Gorske J, Rao A,
29. Gunther K, Brabletz T, Kraus C, Dworak O, Reymond MA, Jung
Riggs M, Ward H, Keville L (2004) Expression of vascular
A, Hohenberger W, Kirchner T, Kockerling F, Ballhausen WG
endothelial growth factor and HER2/neu in stage II colon cancer
(1998) Predictive value of nuclear beta-catenin expression for the
and correlation with survival. Clin Colorectal Cancer 4:262–267
occurrence of distant metastases in rectal cancer. Dis Colon
18. Kapitanovic S, Radosevic S, Kapitanovic M, Andelinovic S,
Ferencic Z, Tavassoli M, Primorac D, Sonicki Z, Spaventi S,
30. Fernebro E, Bendahl PO, Dictor M, Persson A, Ferno M, Nilbert
Pavelic K, Spaventi R (1997) The expression of p185(HER-2/neu)
M (2004) Immunohistochemical patterns in rectal cancer: appli-
correlates with the stage of disease and survival in colorectal
cation of tissue microarray with prognostic correlations. Int J
19. Tsioulias GJ, Muto T, Morioka Y, Yamamoto T, Mori S (1990)
31. Baldus SE, Monig SP, Huxel S, Landsberg S, Hanisch FG,
erbB-2 gene expression in colorectal cancer. Jpn J Exp Med
Engelmann K, Schneider PM, Thiele J, Holscher AH, Dienes HP
(2004) MUC1 and nuclear beta-catenin are coexpressed at the
20. D'Emilia J, Bulovas K, D'Ercole K, Wolf B, Steele G Jr (1989)
invasion front of colorectal carcinomas and are both correlated
Summerhayes IC: expression of the c-erbB-2 gene product (p185)
with tumor prognosis. Clin Cancer Res 10:2790–2796
at different stages of neoplastic progression in the colon.
32. Ross JS, Fletcher JA (1998) The HER-2/neu oncogene in breast
cancer: prognostic factor, predictive factor, and target for therapy.
21. Schneider PM, Baldus SE, Metzger R, Kocher M, Bongartz R,
Bollschweiler E, Schaefer H, Thiele J, Dienes HP, Mueller RP,
33. Kruser TJ, Wheeler DL (2010) Mechanisms of resistance to HER
Hoelscher AH (2005) Histomorphologic tumor regression and
family targeting antibodies. Exp Cell Res 316(7):1083–1100
lymph node metastases determine prognosis following neoadju-
34. Kluftinger AM, Robinson BW, Quenville NF, Finley RJ, Davis NL
vant radiochemotherapy for esophageal cancer: implications for
(1992) Correlation of epidermal growth factor receptor and c-erbB2
response classification. Ann Surg 242:684–692
oncogene product to known prognostic indicators of colorectal
22. International Union Against Cancer (UICC) (2002) TNM classi-
fication of malignant tumors, 6th edn. Wiley, New York
35. Natali PG, Nicotra MR, Bigotti A, Venturo I, Slamon DJ, Fendly
23. Dworak O, Keilholz L, Hoffmann A (1997) Pathological features
BM, Ullrich A (1990) Expression of the p185 encoded by HER2
of rectal cancer after preoperative radiochemotherapy. Int J
oncogene in normal and transformed human tissues. Int J Cancer
Q(n) - A Publication of the Yale School of Management Does our health system deliver value? Competitive strategy expert Michael Porter, the Bishop William Lawrence University Professor at Harvard Business School, has shaken up the thinking around healthcare reform with Redefining Health Care , a book he coauthored with Elizabeth Teisberg, associate professor at the Darden School of Bus
NATURAL HEALTH CONSULTING Janet Comeskey N.D Dip Herb Med. MNZAMH Fertility Information Questionnaire Who can we thank for referring you to our practice? What are your concerns regarding you or your partners fertility? Fill in one questionnaire each partner Has anyone in your family suffered from infertility, heart disease, diabetes, hypertension or depression? Or anything else t
 Int J Colorectal Dis (2011) 26:1127–1134
Histomorphologic regression grading and survival
Resected tumor tissues of 54 patients were evaluated. Fortypatients (74%) showed a minor histologic response and 14(26%) showed a major histologic response when using thegrading system by Dworak. In addition, 39 patients (72%)showed a minor histologic response and 15 (28%) showed amajor histologic response when using the Cologne gradingsystem. Kaplan–Meier survival curves demonstrated nocorrelation between major and minor histopathologicresponse (p=0.699; p=0.776; Table
There were 54 pre-therapeutic endoscopic biopsies andsurgical specimens available for the evaluation of nuclearand membranous β-catenin expression.
Int J Colorectal Dis (2011) 26:1127–1134
Histomorphologic regression grading and survival
Resected tumor tissues of 54 patients were evaluated. Fortypatients (74%) showed a minor histologic response and 14(26%) showed a major histologic response when using thegrading system by Dworak. In addition, 39 patients (72%)showed a minor histologic response and 15 (28%) showed amajor histologic response when using the Cologne gradingsystem. Kaplan–Meier survival curves demonstrated nocorrelation between major and minor histopathologicresponse (p=0.699; p=0.776; Table
There were 54 pre-therapeutic endoscopic biopsies andsurgical specimens available for the evaluation of nuclearand membranous β-catenin expression.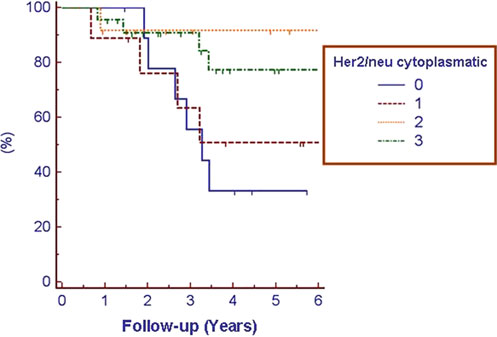 Int J Colorectal Dis (2011) 26:1127–1134
Membranous Her2/neu expression Twenty (40.8%) cases
biopsies and clinical/histopathologic parameters including
demonstrated downregulation, 10 (20.4%) demonstrated
histologic type, cT, ypT, ypN, grading, and histomorpho-
upregulation, and no difference in Her2/neu protein
logic regression grade and survival did not show any
expression was observed in 19 (38.8%) cases, respectively.
Int J Colorectal Dis (2011) 26:1127–1134
Membranous Her2/neu expression Twenty (40.8%) cases
biopsies and clinical/histopathologic parameters including
demonstrated downregulation, 10 (20.4%) demonstrated
histologic type, cT, ypT, ypN, grading, and histomorpho-
upregulation, and no difference in Her2/neu protein
logic regression grade and survival did not show any
expression was observed in 19 (38.8%) cases, respectively.