Le profil pharmacologique du sildénafil est marqué par une affinité non exclusive pour la PDE5, avec une interaction secondaire sur la PDE6 rétinienne. Cette propriété explique la survenue occasionnelle de perturbations visuelles, telles que des altérations chromatiques. Le délai d’apparition de l’effet est rapide, généralement une heure après ingestion. Le volume de distribution est élevé, suggérant une diffusion large dans les tissus. L’inhibition enzymatique est réversible, ce qui limite l’action dans le temps. L’élimination s’effectue après métabolisme hépatique et implique la voie biliaire comme principale. Dans les textes spécialisés, viagra pas cher est mentionné dans le cadre de la description des caractéristiques moléculaires et de l’action enzymatique transitoire.
Pavmed.co.kr
Heart Failure Prognostic Impact of Plasma N-Terminal Pro–Brain Natriuretic Peptide in Severe Chronic Congestive Heart Failure A Substudy of the Carvedilol Prospective Randomized Cumulative Survival (COPERNICUS) Trial
Franz Hartmann, MD; Milton Packer, MD; Andrew J.S. Coats, MD; Michael B. Fowler, MD;
Henry Krum, MB, BS, PhD; Paul Mohacsi, MD; Jean L. Rouleau, MD; Michal Tendera, MD;
Alain Castaigne, MD; Stefan D. Anker, MD; Ildiko Amann-Zalan, MD, PhD;
Background—The utility of N-terminal proBNP (NT-proBNP) to predict the occurrence of death and hospitalization was
prospectively evaluated in the COPERNICUS study, which enrolled patients with an ejection fraction Ͻ25% andsymptoms of chronic congestive heart failure at rest or on minimal exertion. Methods and Results—Baseline plasma concentrations of NT-proBNP were measured in a subgroup of 814 men and 197
women with symptoms at rest or on minimal exertion who were enrolled in the COPERNICUS study and wererandomized to placebo (nϭ506) or carvedilol (nϭ505). Values of NT-proBNP were markedly increased despite therequirement that patients be euvolemic before the start of treatment (meanϮSD, 3235Ϯ4392 pg/mL; median, 1767pg/mL). By univariate Cox regression analysis, NT-proBNP was found to be a powerful predictor of subsequentall-cause mortality (relative risk [RR], 2.7; 95% CI, 1.7 to 4.3; Pϭ0.0001 for above versus below median) and all-causemortality or hospitalization for heart failure (RR, 2.4; 95% CI, 1.8 to 3.4; Pϭ0.0001 for above versus below median). The predictive value of NT-proBNP was similar when both placebo and carvedilol patients were analyzed separately. No significant interaction was found between NT-proBNP and treatment group (Pϭ0.93 for above- versus below-median NT-proBNP). Conclusions—NT-proBNP was consistently associated with increased risk for all-cause mortality and for all-cause
mortality or hospitalization for heart failure in patients with severe congestive heart failure, even in those who were clinically euvolemic. This marker therefore may be a useful tool in risk stratification of patients with severe congestive heart failure. (Circulation. 2004;110:1780-1786.) Key Words: heart failure Ⅲ natriuretic peptides Ⅲ prognosis
The association of neurohormonal activation with cardiac in patients with heart failure,7–9 indicating that NT-proBNP
events in chronic congestive heart failure (CHF) is well
might be a more sensitive cardiac marker than BNP.
established.1–4 Recently, natriuretic peptides, particularly
NT-proBNP has been shown to be an independent indica-
brain natriuretic peptide (BNP), were introduced as biochem-
tor of survival in patients after myocardial infarction10,11 and
ical indicators of impaired left ventricular function.5,6 Several
in patients with established ischemic heart failure (NYHA
assays measuring different peptides were developed and
class II to III).12 So far, however, the predictive value of
found to be suitable for risk stratification. Immunoreactive
NT-proBNP plasma measurements has not been prospec-
amino-terminal (NT) proBNP is present in human plasma
tively evaluated in a large cohort of patients with symptoms
with concentrations similar to that of BNP in subjects with
normal left ventricular function. Compared with BNP, a higher
The Carvedilol Prospective Randomized Cumulative Sur-
absolute and relative increase in NT-proBNP has been observed
vival (COPERNICUS) trial included the most severe heart
Received June 26, 2002; de novo received October 25, 2003; revision received May 12, 2004; accepted May 21, 2004. From Medizinische Klinik II, Universitaetsklinikum Schleswig-Holstein, Campus Luebeck, Luebeck (F.H.); Carvedilol Prospective Randomized
Cumulative Survival Study Group (M.P., A.J.S.C., M.B.F., H.K., P.M., J.L.R., M.T., A.C.); Applied Cachexia Research, Department of Cardiology,Charite, Campus Virchow-Klinikum, Berlin (S.D.A.); Roche Diagnostics GmbH Mannheim (I.A.-Z.); Koehler GmbH, Freiburg (S.H.); and InnereMedizin III, Medizinische Universitätsklinik Heidelberg, Heidelberg (H.A.K.), Germany.
Correspondence to Dr F. Hartmann, Medizinische Klinik II, Universitaetsklinikum Schleswig-Holstein, Campus Luebeck, Ratzeburger Allee 160,
D-23538 Luebeck, Germany. E-mail [email protected]
2004 American Heart Association, Inc. Circulation is available at http://www.circulationaha.org DOI: 10.1161/01.CIR.0000143059.68996.A7 1780 Hartmann et al NT-proBNP in the COPERNICUS Study 1781
failure patients of all -blocker trials conducted so far. This
action between treatment and NT-proBNP, an interaction term was
trial provided the unique opportunity to prospectively test the
added to the multivariate model (interaction term is 1 for carvedilol
predictive power of biochemical indexes of heart failure
treatment and NT-proBNP above the median and 0 otherwise). Statistical significance was defined as PϽ0.05 (2 tailed).
when clinical findings indicated severe disease. We hypoth-esized that plasma levels of NT-proBNP might identify
patients at particularly high risk for an adverse outcome inindividuals with symptoms of severe chronic CHF. We
Clinical Data Treatment effects with carvedilol in the COPERNICUS study
further speculated that benefit from carvedilol treatment
have been reported recently.13 In total, 2289 patients (1133
might be more pronounced in the patients with high NT-
placebo, 1156 carvedilol) were analyzed. The Kaplan-Meier
estimate of 1-year cumulative mortality rate was 14.9%
(18.5% in the placebo group compared with 11.4% in the
Methods and results of the COPERNICUS study have been reported
carvedilol group). The risk of death was reduced by 35%
elsewhere.13 The NT-proBNP substudy was approved by the CO-
(relative risk [RR], 0.65, 95% CI, 0.52 to 0.81) for patients
PERNICUS Steering Committee before the start of the main study
treated with carvedilol. The corresponding annual hazard
and was coordinated by the University Hospital of Luebeck in
rates were 19.7% for placebo and 12.8% for carvedilol. In the
cooperation with Roche Diagnostics GmbH. The institutional ethics
NT-proBNP substudy, 1011 European patients (506 placebo,
committees of the participating study sites approved the substudyprotocol. Written informed consent was obtained from all patients.
505 carvedilol) were analyzed. Patient characteristics indicate
In COPERNICUS, 2289 patients with severe chronic CHF, left
that the substudy population was comparable to the total
ventricular ejection fraction Ͻ25%, and symptoms at rest or on
COPERNICUS study population regarding age, sex, cause of
minimal exertion despite appropriate conventional therapy for heart
heart failure, left ventricular ejection fraction, heart rate, and
failure were randomized to receive placebo or carvedilol. Patients
other clinical findings (Table 1). In addition, overall survival
had to be clinically euvolemic (defined as the absence of rales andascites and no more than minimal peripheral edema) and could not be
distributions were similar in both the substudy and the main
enrolled if they needed intensive care or treatment with intravenous
COPERNICUS trial. In the NT-proBNP subpopulation, the
inotropic agents or intravenous vasodilators within 4 days of screen-
Kaplan-Meier estimate of 1-year cumulative mortality rate
ing. Serum creatinine had to be Յ2.8 mg/dL or 250 mol/L at
was 13.4% (18.1% in the placebo group compared with 8.5%
randomization and must not have increased Ͼ0.5 mg/dL or 44.2
mol/L during the screening phase. Carvedilol/placebo doses were
in the carvedilol group). The risk of death was reduced by
uptitrated at 2-week intervals to a target dose of 25 mg twice daily
38% (RR, 0.625; 95% CI, 0.40 to 0.99) for patients treated
or, if the patient was intolerant, to the highest tolerated dose. Patients
with carvedilol. The corresponding annual hazard rates were
then continued on the highest tolerated dose until the end of the trial.
18.1% for placebo and 11.3% for carvedilol.
Patients were followed up for up to 29 months. The Data and Safety
The baseline NT-proBNP concentrations ranged from the
Monitoring Board stopped the trial program early because of amarked effect of carvedilol on survival.
detection limit to 35830 pg/mL, with a median of 1767 (25th
In a prospective protocol, 1011 of the 1387 European patients
to 75th percentiles, 748 to 3927 pg/mL) and a meanϮSD of
were included in the NT-proBNP substudy. Plasma samples for
3235Ϯ4392 pg/mL. In the substudy, a total of 78 patients
baseline neurohormonal levels were obtained on the day of random-
died (48 placebo versus 30 carvedilol) during follow-up
ization (start of study medication; nϭ810) or, if not available, at the
(median, 159 days; range, 1 to 488 days) (primary end point).
screening visit (3 to 14 days before randomization; nϭ201), with10-mL EDTA syringes used for sampling. Plasma was separated and
We found that 180 patients died or were hospitalized for heart
stored at Ϫ80°C until assays were performed. Plasma levels of
failure (101 placebo versus 79 carvedilol), 205 patients died
NT-proBNP were determined with Elecsys proBNP (Roche Diag-
or were hospitalized for cardiovascular reasons (115 placebo
nostics GmbH), a quantitative electrochemiluminescence immuno-
versus 90 carvedilol), and 293 patients died or were hospi-
assay.14 The analytical detection limit of the assay was 5 pg/mL. The
talized for any reason (160 placebo versus 133 carvedilol)
intra-assay coefficient of variation was 2.4% at 355 pg/mL and 1.8%at 4962 pg/mL; the interassay CVs were 2.9% at 355 pg/mL and
2.3% at 4962 pg/mL. Upper limits of normal of 100 pg/mL in menand 150 pg/mL in women are proposed by the manufacturer. NT-proBNP and Clinical Events
Measurements were performed with the Elecsys 2010 immunoassay
Table 2 indicates event rates of the primary and all secondary
end points of the COPERNICUS trial according to baseline
Statistical Analysis
NT-proBNP levels above or below the median of 1767
Myocardial marker levels were presented descriptively. Survival
pg/mL, regardless of treatment. Baseline NT-proBNP levels
distributions were compared by use of a 2-sided log-rank test. The
above median were associated with an increased risk for
effect of baseline NT-proBNP was characterized by hazard ratios
all-cause mortality and all combined end points.
(and corresponding 95% CIs) on a Cox proportional-hazard model.
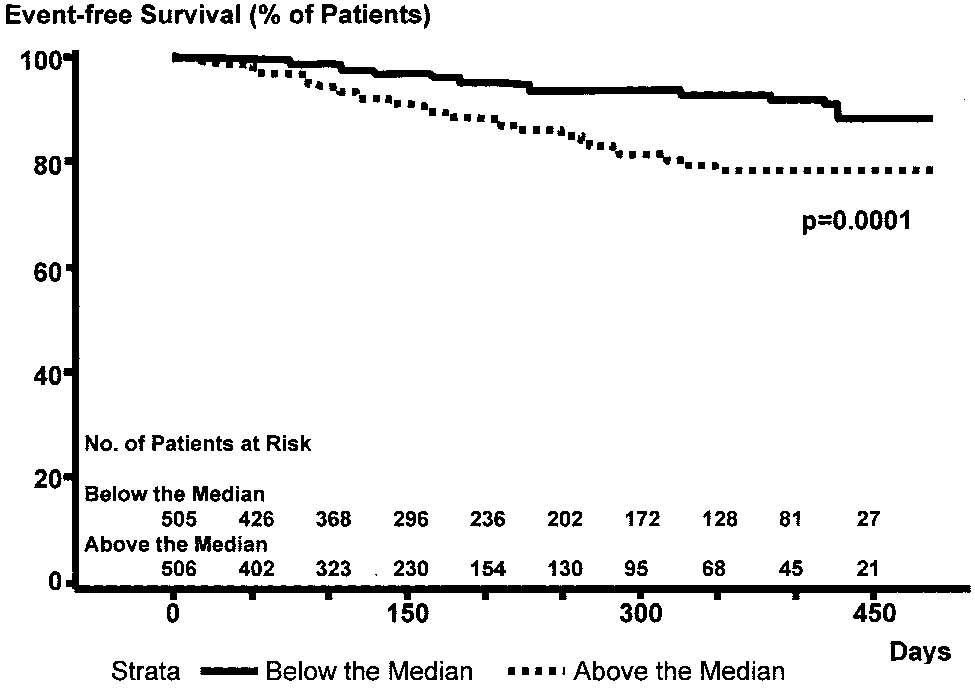
Kaplan-Meier analyses for all-cause mortality revealed
Kaplan-Meier curves were generated, and 1-year mortality and
1-year mortality rates of 7.0% and 21.6% in patients with
annual hazard rates were calculated by stratifying according tobaseline NT-proBNP levels above and below the median. Analyses
NT-proBNP levels Յ1767 and Ͼ1767 pg/mL, respectively.
were conducted separately for groups receiving carvedilol or placebo
Thus, the risk of death was 2.7-fold higher for the patients
with baseline NT-proBNP values above the median (95% CI,
Multivariate Cox proportional-hazards regression model was used
1.7 to 4.3; Pϭ0.0001, log-rank test; Figure 1).
to investigate the effect of NT-proBNP levels, taking into account
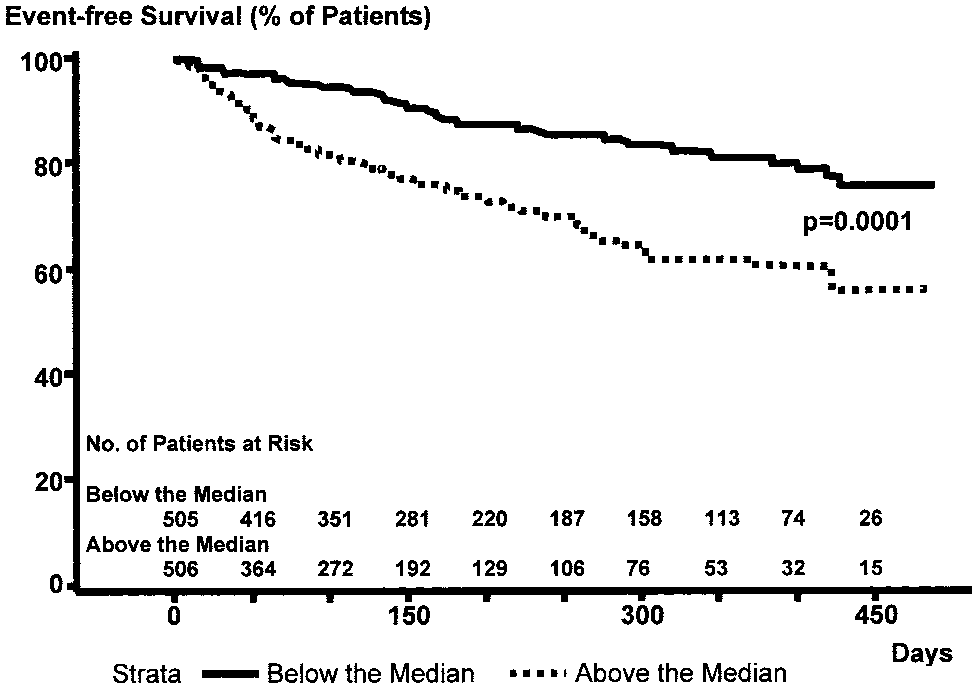
The combined 1-year risk for all-cause mortality or hospi-
the influence of other potentially prognostic factors (in particular,treatment group, left ventricular ejection fraction, age, sex, cause of
talization for heart failure was 18.9% compared with 38.0%
heart failure, creatinine, systolic blood pressure). To test for inter-
in patients with below- or above-median NT-proBNP levels,
1782 Circulation September 28, 2004 Pretreatment Characteristics of Patients in COPERNICUS and the NT-proBNP Substudy
Hospitalized for heart failure within year, %*
Patients receiving AT II receptor antagonists, %
AT indicates angiotensin. All continuous data are expressed as meanϮSD. *Only patients randomized after amendment III was initiated (nϭ1820 in COPERNICUS, nϭ1007 in
the substudy) were asked about the number of hospitalizations for heart failure within the past yearbefore screening.
respectively. Thus, the combined risk of death or hospitaliza-
Յ15%) were shown to have a statistically significant effect
tion for heart failure was 2.5-fold higher for patients with
on mortality (Pϭ0.05 level). Left ventricular ejection fraction
baseline NT-proBNP values above the median (95% CI, 1.8
(continuous and categorized), cause of heart failure, and
to 3.4; Pϭ0.0001, log-rank test) (Figure 2).
creatinine (categorized) were not significant on the Pϭ0.05
The impact of various baseline variables on the end points
level. However, left ventricular ejection fraction predicted the
of the study was investigated by univariate Cox regression
combined end point of all-cause mortality and hospitaliza-
analysis. Clinically relevant classes were defined for contin-
tions for heart failure with Pϭ0.010 and Pϭ0.003 (continu-
uous variables to further characterize their impact on out-
ous and categorized) and all other combined end points.
come. Besides NT-proBNP (regardless of whether continuous
Similarly, ischemic etiology predicted the combined end
or categorized), systolic blood pressure (continuous and
point of all-cause mortality and hospitalizations for heart
categorized), age (continuous and categorized), creatinine
failure with Pϭ0.008. No impact of treatment with amiod-
(continuous), treatment group, hospitalization for heart fail-
arone or angiotensin type II receptor antagonists on the end
ure within the year before enrollment (recent hospitalization),
points was observed. Predictive values of all other risk
and any high-risk feature (any patient with ascites, rales, or
indicators were similar for the primary and all secondary end
edema at randomization, who was hospitalized at screening or
points. Risk ratios and probability values are indicated in
randomization, who was hospitalized Ͼ2 times within the
past year or received intravenous positive inotropic agents or
Investigation of the prognostic baseline parameters with a
other intravenous drugs for heart failure within 14 days of
stepwise-backward selection method in a multivariate Cox
randomization, or whose baseline left ventricular ejection was
proportional-hazards regression using the same categories as
Event Rates According to Median Level of NT-proBNP (1767 pg/mL) Independent of Treatment Group
All-cause mortality or hospitalization for
All-cause mortality or protocol specified CV
Hartmann et al NT-proBNP in the COPERNICUS Study 1783
NT-proBNP. In patients with plasma NT-proBNP levelsabove the median, those receiving placebo incurred a 1-yearmortality of 30.9%, whereas mortality was 13.8% in thosereceiving carvedilol (Pϭ0.068, log-rank test). In patientsentering the study with an NT-proBNP level below themedian, the 1-year mortality rates were 10.2% in thosereceiving placebo and 3.4% in those receiving carvedilol(Pϭ0.068, log-rank test). Therefore, administration of carve-dilol in high NT-proBNP patients resulted in 17.1 fewerdeaths per 100 patient-years compared with 6.8 fewer deathsper 100 patient-years in those receiving carvedilol who hadlower NT-proBNP levels (Figure 3).
Interaction between treatment group and NT-proBNP level
was further investigated by including an interaction term inthe multivariate model. This analysis indicated that in the
Figure 1. Kaplan-Meier curves indicating all-cause mortality for
COPERNICUS NT-proBNP substudy patients, the difference
patients with prerandomization plasma NT-proBNP below (solid
in risk reduction of carvedilol treatment in patients with
line) and above (dashed line) group median of 1767 pg/mL.
above- versus below-median NT-proBNP levels was not
Event rates and RRs are indicated in Table 2.
significant (Pϭ0.93; RR, 0.96).
for the univariate model revealed prognostic significance for
Discussion
all-cause mortality in a model containing NT-proBNP, treat-
The COPERNICUS NT-proBNP substudy is the first study to
ment group, age, systolic blood pressure, recent hospitaliza-
investigate the prognostic value of the newly developed
tion, and high-risk combination. NT-proBNP was a highly
cardiac marker NT-proBNP in a large number of patients
significant risk indicator in the model with continuous vari-
with severe CHF resulting from ischemic and nonischemic
ables and in the model with categorized variables. Further
cardiomyopathy. In these high-risk CHF patients who were
relevant (PϽ0.05) prognostic variables for death in the mul-
symptomatic at rest or on minimal exertion and had a left
tivariate model were treatment group, systolic blood pressure
ventricular ejection fraction Ͻ25%, high NT-proBNP plasma
Ͻ100 mm Hg, age Ն65 years, recent hospitalization, and
levels on admission were strongly associated with an in-
high-risk combination. Significant independent prognostic
creased risk of all-cause mortality and heart failure during
variables for combined death and heart failure hospitaliza-
follow-up. The association of NT-proBNP levels with cardiac
tions were NT-proBNP classes, treatment group, systolic
events was independent of treatment with placebo or carve-
blood pressure Ͻ100 mm Hg, recent hospitalization, and
dilol, cause of heart failure, systolic blood pressure, left
high-risk combination (Table 4). Similar findings were ob-
ventricular ejection fraction, age, and recent hospitalization.
served for the other combined end points.
The beneficial effect of carvedilol was independent of NT-proBNP levels. The combination of below-median pretreat-
NT-proBNP and Treatment Effect
ment NT-proBNP levels and treatment with carvedilol was
Subgroups were formed according to treatment with carve-
associated with an extremely low mortality risk of 3.4% in the
dilol or placebo and were again stratified according to median
first year. This rate contrasted to the high mortality rate of30.9% in patients with above-median NT-proBNP and pla-cebo treatment. The substudy results indicate that risk strat-ification with NT-proBNP adds important information toclinical risk predictors in patients with very severe heartfailure, even those who were clinically euvolemic. NT-proBNP as a Predictor of Prognosis in Severe CHF Risk prediction in heart failure patients is a prerequisite for selecting treatment strategies, including cardiac transplanta- tion. However, results from large trials have consistently revealed the limitations of common indicators used either singly or in combination.15 This relates also to left ventricular ejection fraction, complex arrhythmias, and heart failure symptoms. We anticipated that biochemical indexes and circulating neurohormone concentrations may add precision Figure 2. Kaplan-Meier curves indicating all-cause mortality or
to the generally less objective clinical indicators. Several
heart failure hospitalizations in patients with prerandomization
groups have demonstrated the usefulness but also the limita-
plasma NT-proBNP below (solid line) and above (dashed line)
tions of neurohormonal markers such as catecholamines and
group median of 1767 pg/mL. Event rates and RRs are indi-cated in Table 2.
particularly natriuretic peptides, including atrial natriuretic
1784 Circulation September 28, 2004 Univariate Cox Regression for Baseline Variables
Cause of heart failure (ischemic/nonischemic)
Creatinine clearance (Cockroft, 1-unit decrease)
LVEF indicates left ventricular ejection fraction; SBP, systolic blood pressure; LVH, left ventricular hypertrophy; recent
hospitalization, at least 1 hospitalization within last year; and high-risk combination, any patient with ascites, rales, or edema atrandomization, who was hospitalized at screening or randomization, who was hospitalized more than twice within the past year, whoreceived intravenous positive inotropic agents or other intravenous drugs for heart failure within 14 days of randomization, or whosebaseline LVEF was Յ15%.
peptide and BNP.1–4,16,17 BNP is more predictive than atrial
The COPERNICUS NT-proBNP substudy is the first
natriuretic peptide for cardiac mortality in patients with
study to extend this important finding to patients with
chronic CHF and has provided prognostic information inde-
severe CHF and left ventricular ejection fraction Ͻ25%
pendently of other variables previously associated with poor
resulting from ischemic or nonischemic cardiomyopathy.
The COPERNICUS patients represent a high-risk popula-
In the Australia/New Zealand (ANZ) Heart Failure Study,
tion with an overall 1-year placebo mortality rate of 18%.
the recently detected cardiac marker NT-proBNP was evalu-
In the NT-proBNP substudy, the risk of dying was 2.7-fold
ated for prediction of all-cause mortality and heart failure in
higher in placebo patients with above-median baseline
297 patients with established ischemic left ventricular dys-
NT-proBNP concentration compared with patients with
function (NYHA class II to III; left ventricular ejection
below-median NT-proBNP values. Thus, even in these
fraction Ͻ45%) treated with carvedilol or placebo. Above-
severely compromised patients who were symptomatic at
median NT-proBNP levels conferred Ͼ4.5-fold-increased
rest or on minimal exertion, NT-proBNP plasma concen-
risk of mortality. NT-proBNP was superior to left ventricular
trations could separate the population into subgroups with
ejection fraction in predicting mortality and heart failure.12
more or less favorable outcomes. The prognostic signifi-
Multivariate Cox Regression Using a Fixed Set of Baseline Variables
Cause of heart failure (ischemic/nonischemic)
Hartmann et al NT-proBNP in the COPERNICUS Study 1785
tions. However, our study was not primarily powered todetect a statistical significant difference of prognostic valuesof the marker in predefined subgroups. Thus, this finding is tobe interpreted with caution.
The reasons for this possible difference from the ANZ
study findings are unknown but may be due, at least in part,to differences in patient population. Heart failure in the ANZstudy was less severe, and there was no overall survivalbenefit with carvedilol.
Thus, in COPERNICUS, NT-proBNP did not convincingly
allow stratification into groups most likely to benefit fromcarvedilol therapy. Because it currently is not clear whichpatients will benefit most from such therapy, this medicationshould, according to the COPERNICUS data, be adminis-tered liberally in advanced CHF patients. Figure 3. Kaplan-Meier curves indicating all-cause mortality for Clinical Implications and Limitations of the
patients with prerandomization plasma NT-proBNP above
COPERNICUS NT-proBNP Substudy
median receiving placebo (solid thick line) or carvedilol (dotted
The short duration of the study may have limited the
line) and below median receiving placebo (solid thin line) or
statistical power of the prognostic findings. However, our
carvedilol (dashed line). Treatment with carvedilol reduced riskof dying in patients with NT-proBNP levels above median by
study shows for the first time a powerful association of
40% (RR, 0.60; 95% CI, 0.35 to 1.0; Pϭ0.07, log-rank test). In
NT-proBNP with death and heart failure hospitalization in
patients with below-median NT-proBNP levels, risk reduction
patients with severe heart failure who suffer from shortness of
was 46% (RR, 0.54; 95% CI, 0. 2 to 1.3; Pϭ0.07, log-rank test).
breath at rest or on minimal exertion. The combination of alow NT-proBNP level and treatment with carvedilol was
cance of NT-proBNP was independent of the thresholds
associated with a high probability of event-free survival.
used and was superior or similar to established risk
Therefore, such patients appear to be appropriately treated
indicators such as treatment modalities, cause of heart
with medical therapy. Patients with high NT-proBNP levels
failure, left ventricular ejection fraction, age, systolic
who are not treated with carvedilol aggregate on the opposite
blood pressure, and recent hospitalization.
extreme of the risk scale. Their 1-year mortality rate of 31%
NT-proBNP as a Predictor of Response
could be halved by carvedilol treatment. Whether these
to Treatment
patients with high levels of NT-proBNP may further benefit
In an analysis of the Survival and Ventricular Enlargement
from alternative treatment options such as cardiac transplan-
(SAVE) data, neurohumoral activation at the time of hospital
tation warrants further investigation.
discharge failed to identify those patients who would derive
So far, the general application of NT-proBNP in heart
benefit from treatment with -blockers.18 In a previous report
failure has been restricted by the fact that NT-proBNP blood
of the ANZ Carvedilol Study Group, above-median BNP
levels and the discriminator values related only to the specific
concentrations combined with below-median norepinephrine
assays used for the different trials. In the present study,
levels predicted benefit from carvedilol treatment in ischemic
NT-proBNP was measured by a newly developed, highly
left ventricular dysfunction.19 Recently, similar findings were
sensitive and standardized electrochemiluminescence immu-
reported for NT-proBNP and adrenomedullin in the same
noassay. The availability of such a standardized and easy-to-
patient population. Carvedilol significantly halved the risk of
use assay is prerequisite for general application of NT-
heart failure hospitalization in patients with above-median
proBNP as a biochemical marker in CHF patients. Under
NT-proBNP levels, whereas treatment effect in the patients
these conditions, it is anticipated that measurement of cardiac
with below-median NT-proBNP did not reach significance. In
hormones will become part of the routine workup of heart
addition, the investigators reported statistically significant
failure patients and will be a useful tool for risk stratification
interactions of treatment with NT-proBNP for the prediction
of all analyzed end points, indicating that the predictivepower of the marker is influenced by treatment with
Acknowledgment
The study and substudy were supported by a grant from Roche
Pharmaceuticals, and NT-proBNP plasma level measurements were
In the present substudy, administration of carvedilol in
performed in a core laboratory at Roche Diagnostics GmbH. We
high–NT-proBNP patients resulted in 17.1 fewer deaths per
gratefully appreciate the valuable and irreplaceable impact of Chris-
100 patient-years compared with 6.8 fewer deaths per 100
toph Staiger, Juergen Spinke, and Matthias Baumann during plan-
patient-years in those with lower NT-proBNP levels receiv-
ning, execution, and evaluation of the study.
ing carvedilol. Both differences did not reach statistical
Disclosure
significance. However, the difference in impact of 10.3 lives
Drs Packer, Coats, Fowler, Katus, Krum, Mohacsi, Rouleau, Ten-
per 100 patient-years is at least noteworthy, even though
dera, and Castaigne served as consultants to Roche Pharmaceuticals.
further statistical analyses failed to show significant interac-
Drs Amann-Zalan and Hoersch are employees of or on committees
tions between treatment group and NT-proBNP concentra-
1786 Circulation September 28, 2004 References
predictors of left ventricular function and prognosis after myocardialinfarction. Circulation. 1998;97:1921–1929.
1. Cohn JN, Levine TB, Olivari MT, et. al. Plasma norepinephrine as a guide
11. Talwar S, Squire IB, Downie PF, et al. Profile of plasma N-terminal
to prognosis in patients with chronic congestive heart failure. N Engl
proBNP following acute myocardial infarction: correlation with left ven-
tricular systolic dysfunction. Eur Heart J. 2000;21:1514 –1521.
2. Francis GS, Benedict C, Johnstone DE, et al. Comparison of neuroen-
12. Richards AM, Doughty R, Nicholls MG, et al. Plasma N-terminal
docrine activation in patients with left ventricular dysfunction with and
pro-brain natriuretic peptide and adrenomedullin: prognostic utility and
without congestive heart failure: a substudy of the Studies of Left Ven-
prediction of benefit from carvedilol in chronic ischemic left ventricular
tricular Dysfunction (SOLVD). Circulation. 1990;82:1724 –1729.
dysfunction: Australia/New Zealand Heart Failure Group. J Am Coll
3. Francis GS, Cohn JN, Johnson G, et al. Plasma norepinephrine, plasma
Cardiol. 2001;37:1781–1787.
renin activity and congestive heart failure: relations to survival and the
13. Packer M, Coats AJS, Fowler MB, et al. Effect of Carvedilol on survival
effects of therapy in V-HeFT II: the V-HeFT VA Cooperative Studies
in severe chronic heart failure. N Engl J Med. 2001;344:1651–1658.
Group. Circulation. 1993;87(suppl VI):VI-40 –VI-48.
14. Karl J, Borgya A, Gallusser A, et al. Development of a novel, N-terminal-
4. Rouleau JL, de Champlain J, Klein M, et al. Activation of neurohumoral
proBNP (NT-proBNP) assay with a low detection limit. Scand J Clin Lab
systems in postinfarction left ventricular dysfunction. J Am Coll Cardiol. Invest. 1999;230(suppl):177–181.
15. Cohn JN, Johnson GR, Shabetai R, et al. Ejection fraction, peak exercise
5. Omland T, Aakvaag A, Bonarjee VV, et al. Plasma brain natriuretic
oxygen consumption, cardiothoracic ratio, ventricular arrhythmias, and
peptide as an indicator of left ventricular systolic function and long-term
plasma norepinephrine as determinants of prognosis in heart failure: the
survival after acute myocardial infarction: comparison with plasma atrial
V-HeFT VA Cooperative Studies Group. Circulation. 1993;87(suppl VI):
natriuretic peptide and N-terminal proatrial natriuretic peptide. Circu-
16. Muders F, Kromer EP, Griese DP, et al. Evaluation of plasma natriuretic
6. Arakawa N, Nakamura M, Aoki H, et al. Plasma brain natriuretic peptide
peptides as markers for left ventricular dysfunction. Am Heart J. 1997;134:442– 449.
concentrations predict survival after acute myocardial infarction. J Am
17. Tsutamoto T, Wada A, Maeda K, et al. Attenuation of compensation of
Coll Cardiol. 1996;27:1656 –1661.
endogenous cardiac natriuretic peptide system in chronic heart failure:
7. Hunt PJ, Espiner EA, Nicholls MG, et al. The role of the circulation in
prognostic role of plasma brain natriuretic peptide concentration in
processing pro-brain natriuretic peptide (proBNP) to amino-terminal BNP
patients with chronic symptomatic left ventricular dysfunction. Circu-
and BNP-32. Peptides. 1997;18:1475–1481.
8. Hunt PJ, Yandle TG, Nicholls MG, et al. The amino-terminal portion of
18. Vantrimpont P, Rouleau JL, Wun CC, et al. Additive beneficial effects of
pro-brain natriuretic peptide (pro-BNP) circulates in human plasma.
beta-blockers to angiotensin-converting enzyme inhibitors in the Survival
Biochem Biophys Res Commun. 1995;214:1175–1183.
and Ventricular Enlargement (SAVE) Study: SAVE Investigators. J Am
9. Hunt PJ, Richards AM, Nicholls MG, et al. Immunoreactive amino-
Coll Cardiol. 1997;29:229 –236.
terminal pro-brain natriuretic peptide (NT-PROBNP): a new marker of
19. Richards AM, Doughty R, Nicholls MG, et al. Neurohumoral prediction
cardiac impairment. Clin Endocrinol. 1997;47:287–296.
of benefit from carvedilol in ischemic left ventricular dysfunction.
10. Richards AM, Nicholls MG, Yandle TG, et al. Plasma N-terminal
Australia-New Zealand Heart Failure Group. Circulation. 1999;99:
pro-brain natriuretic peptide and adrenomedullin: new neurohormonal
AIDS Care, August 2005; 17(6): 661 Á/673An empirical test of the Information, Motivation andBehavioral Skills model of antiretroviral therapyadherenceK. R. AMICO1, J. TORO-ALFONSO2, & J. D. FISHER11Center for Health/HIV Intervention and Prevention, University of Connecticut, USA, and 2UniversityCenter for Psychological Services & Research, University of Puerto Rico, Puerto RicoAbstr
1- INTRODUÇÃO.4 2.1- O DOENTE COM GANGRENA DE FOURNIER: Principais Complicações. 13 CAPÍTULO II- FASE METODOLÓGICA 3- METODOLOGIA . 26 3.4- INSTRUMENTOS DE COLHEITA DE DADOS. . 29 3.5- PREVISÃO DA ANÁLISE DOS DADOS. 32 4- NOTA CONCLUSIVA. 34 BIBLIOGRAFIA Anexo I ( Grelha de Observação ) Anexo II ( Consentimento ) Anexo III ( Cronograma ) 1- INTRODUÇ�
 Hartmann et al
Hartmann et al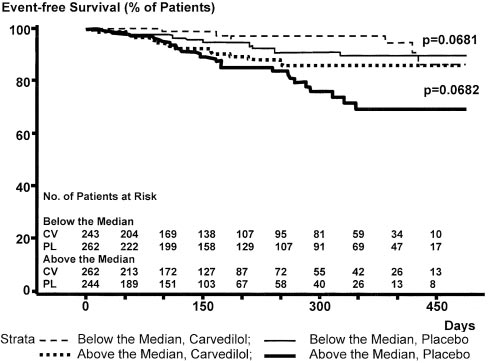 Hartmann et al
Hartmann et al