Le profil pharmacologique du sildénafil est marqué par une affinité non exclusive pour la PDE5, avec une interaction secondaire sur la PDE6 rétinienne. Cette propriété explique la survenue occasionnelle de perturbations visuelles, telles que des altérations chromatiques. Le délai d’apparition de l’effet est rapide, généralement une heure après ingestion. Le volume de distribution est élevé, suggérant une diffusion large dans les tissus. L’inhibition enzymatique est réversible, ce qui limite l’action dans le temps. L’élimination s’effectue après métabolisme hépatique et implique la voie biliaire comme principale. Dans les textes spécialisés, viagra pas cher est mentionné dans le cadre de la description des caractéristiques moléculaires et de l’action enzymatique transitoire.
Survey on cannabis use in parkinson's disease: subjective improvement of motor symptoms
5. Powers JM. Blepharospasm due to unilateral diencephalon infarc-
6. Keane JR, Young JA. Blepharospasm with bilateral basal ganglia
infarction. Arch Neurol 1985;42:1206 –1208.
7. Verghese J, Rosenbaum DM. Ptosis, blepharospasm, and apraxia
of eyelid opening secondary to putaminal hemorrhage. Neurology1999;53:652.
8. Schmidtke K, Butnner-Ennever JA. Nervous control of eyelid
function: a review of clinical, experimental and pathological data. Brain 1992;115:227–247.
9. Hallet M. Blepharospasm. Recent advances. Neurology 2002;59:
10. Wali GM. Asymmetrical blepharospasm associated with a left
frontal cortical infarct. Mov Disord 2001;16:181–182.
11. Perlmutter JS, Stambuk MK, Markham J, et al. Decreased 18F-
spiperone binding in putamen in idiopathic focal dystonia. J Neu-rosci 1997;17:843– 850.
12. Esmaeli-Gutsein B, Nahmias C, Thompson M, et al. Positron
emission tomography in patients with benign essential blepharo-spasm. Ophthalmol Plast Reconstr Surg 1999;15:23–27.
13. Schmidt K, Linden DE, Goebel R, Zamella F, Lanfermann H,
Zubcov A. Striatal activation during blepharospasm revealed byfMRI. Neurology 2003;60:1738 –1743. Survey on Cannabis Use in Parkinson’s Disease: Subjective Improvement of Motor Symptoms
Evzˇen Ru˚zˇicˇka, MD, DSc,2* Viktor Vorˇı´sˇek, PharmD,3
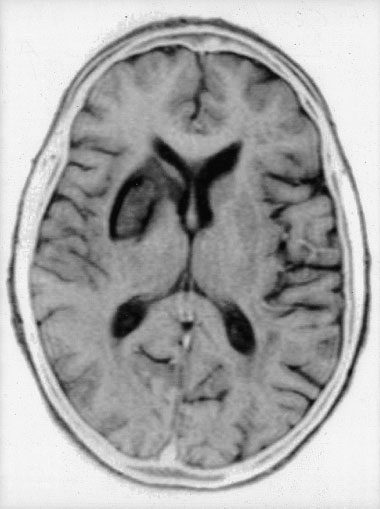
FIG. 2. Brain magnetic resonance T2-weighted axial image showing a
right striatal infarct involving caudate and putamen. 1Department of Pharmacology and Toxicology, Faculty ofPharmacy, Charles University, Hradec Kra´love´,
The eyelid motor disturbance in our patient was transient, with
complete remission in 2 weeks. This finding may be related to the
2Movement Disorders Centre, Department of Neurology, 1st
recovery of normal function that often occurs after ischemia,
Medical Faculty, Charles University, Prague, Czech Republic
although some compensatory mechanisms also might have taken
3Division of Clinical Toxicology and Mass Spectrometry,
place during this time. For instance, in addition to an improvement
Department of Biochemistry, University Hospital Hradec
of a possible edema of the internal capsule, the intact hemisphere
could have taken over or even a functional reorganization of theipsilateral cerebral cortex could have occurred. Abstract: An anonymous questionnaire sent to all patients
In conclusion, unilateral striatal infarctions may cause a
attending the Prague Movement Disorder Centre revealed that
transient prominent reflex blepharospasm. These eyelid abnor-
25% of 339 respondents had taken cannabis and 45.9% of these
malities may reflect a disruption of a common supranuclear
described some form of benefit. 2004 Movement Disorder
pathway linking the nondominant cerebral hemisphere, the
basal ganglia, and the brainstem, and emphasize the role of the
Key words: cannabis; Parkinson’s disease; cannabinoid
striatum, particularly the putamen, in the pathophysiology ofsome eyelid motor disorders.
The cannabis plant (Cannabis sativa) contains compounds
References
called cannabinoids that are exclusive to the Cannabaceaefamily. These compounds exert their pharmacologic effect by
1. Hijosa M, Esteban A, Sanchez Migallon MJ, Grandas F. Palpebral
acting on specific G protein-coupled cannabinoid receptors.
ptosis and blepharospasm secondary to hemispheric cerebral in-farction. Neurologia 1998;13:49 –53.
2. Averbuch-Heller L, Leigh RJ, Mermelstein V, Zagalski L, Streifler
JY. Ptosis in patients with hemispheric strokes. Neurology 2002;
*Correspondence to: Dr. Evzˇen Ru˚zˇicˇka, Movement Disorders Cen-
tre, Department of Neurology, 1st Medical Faculty, Charles University,
3. Lee MS, Marsden CD. Movement disorders following lesions of the
Prague, Czech Republic. E-mail: [email protected]
thalamus and subthalamic region. Mov Disord 1994;9:493–507.
Received 12 July 2003; Revised 20 December 2003; Accepted 16
4. Larumbe R, Vaamonde J, Artieda J, et al. Reflex blepharospasm
associated with bilateral basal ganglia lesion. Mov Disord 1993;
Published online 21 April 2004 in Wiley InterScience (www. interscience.wiley.com). DOI: 10.1002/mds.20111 Movement Disorders, Vol. 19, No. 9, 2004TABLE 1. Mean age and duration of Parkinson’s disease in
uses cannabis, how frequently, how regularly, for how long,
patients who had used and not used cannabis
which part of the plant, whether there was an effect on cardinal
motor symptoms of PD and on levodopa (L-dopa)-induceddyskinesias, and if any, when the effect had appeared), on the
possible use of other drugs of abuse and current antiparkinso-
nian treatment. The terms muscle rigidity, bradykinesia, and
dyskinesias were explained briefly. Patients were asked to rate
the subjective changes in each symptom and dyskinesias asfollows: substantial improvement, mild improvement, nochange, mild worsening, substantial worsening, or I do notknow. We have analyzed urine from 7 patients who had taken
Two types of cannabinoid receptors have been isolated so far.
cannabis regularly for more than one year and a single patient
CB receptor is localized predominantly in the central nervous
who had only taken it 1 day before analysis. The patients had
system (CNS),1 whereas CB is found mostly in organs and
expressed their willingness to participate in further studies, had
cells of the immune system. To date, a number of endogenous
reported cannabis use, and were able to attend the hospital to
agonists at cannabinoid receptors have been isolated that in-
submit urine samples. We carried out preliminary screening
clude anandamide2 and 2-arachidonyl glycerol (2-AG).3
(EMIT II plus Cannabinoid Assay; Dade Behring, USA) fol-
The potential use of cannabis or cannabinoids in pharmaco-
lowed by gas chromatography/mass spectrometry (GC/MS)
therapy of various medical conditions including Parkinson’s
quantitative analysis (ion 371 m/z was monitored in silylated
disease (PD) and dyskinetic movement disorders has been
11-nor-␦-9-tetrahydrocannabinol-9-carboxylic acid; 11-nor-␦-
discussed recently,4 substantiated by rich representation of can-
9-THCOOH) on ion trap spectrometer Magnum (ThermoFinni-
nabinoid system in the basal ganglia. The globus pallidus and
gan) equipped with capillary column DB1ms (30 m; 0.25 m;
substantia nigra pars reticulata contain the highest density of
0.25 mm; JW Scientific-Agilent, USA; silylation reagent: bis(tri-
CB receptors in the body.5,6 The concentration of anandamide
methylsilyl)trifluoroacetamide) ϩ trimethylchlorosilane 99:1;
in the globus pallidus and substantia nigra is three times higher
standards: drugs of abuse control S1, S2 and S3 (Bio-Rad)). For
than in other brain regions.7 Cannabinoid system therefore
extraction of cannabinoids, SPEC-C18-I Cartridges (Ansys,
might play some physiological role in the basal ganglia control
Inc., USA) and vacuum extractor Supelco Visiprep 24 were
of movement and this is supported by the finding that CB1
knockout mice exert lower locomotor activity.8,9
The use of cannabis has been presented in Czech media as
being possibly helpful in Parkinson’s disease, which was ini-tiated mainly by one of our patients who objectively improved
Out of 630 questionnaires sent by mail, 339 (53.8%) were
his PD symptoms after long-term use of cannabis.10 We real-
returned (195 men, 139 women; 5 without answer regarding
ized that after this public information, some of our patients
gender). The responders’ mean age was 65.7 years (age range,
spontaneously started to take cannabis to alleviate their PD
36 –92 years) and the mean PD duration was 8.5 years (range,
symptoms. The aim of this study therefore is to evaluate their
Ͻ1–30 years). Cannabis use was reported by 85 patients
(25.1% of returned questionnaires; 55 men, 29 women, 1 with-out answer), most of them using approximately half a teaspoonof fresh or dried leaves orally (only 1 patient inhaled), usually
Subjects and Methods
with meals (43.5%) and mostly once a day (52.9%). There were
The protocol was approved by the Research Ethics Commit-
no major differences in age and duration of PD between the
tee of the General University Hospital in Prague and informed
subgroup of patients using cannabis and those who had never
consent was obtained from all subjects participating in the
used it (Table 1). Patients mostly decided to take cannabis
analytical part of this study. All patients with PD registered at
based on information presented in the media. None of the
Prague Movement Disorders Centre were asked to anony-
patients had any experience with recreational use of cannabis
mously complete a questionnaire about their possible experi-
before taking it to alleviate PD symptoms. None had been
ence with cannabis. For this purpose, we modified the ques-
advised to use cannabis by a doctor, and all patients continued
tionnaire that Consroe and colleagues11 used to describe the
using the antiparkinsonian therapy recommended by their neu-
effects of cannabis on multiple sclerosis symptoms. This ques-
rologist. After cannabis, 39 patients (45.9%) described mild or
tionnaire asks for basic personal data (age, gender, duration of
substantial alleviation of their PD symptoms in general, 26
PD), questions on the possible use of cannabis (if the patient
(30.6%) improvement of rest tremor, 38 (44.7%) alleviation of
TABLE 2. Relationship between the duration of cannabis use and number of patients reporting alleviation of symptoms
cannabis use Total (n) Improved improved answer Improved improved answer Improved improved answer Improved improved answer
Movement Disorders, Vol. 19, No. 9, 2004TABLE 3. Relationship between the frequency of cannabis
bradykinesia or rigidity. In contrast, in patients where 11-nor-
doses and number of patients reporting improvement
␦-9-THCOOH levels were lower than 50 ng/ml (3/7), there was
no reported improvement in either. It is of interest that 1 patientwho did not take cannabis regularly but who had taken it the
day before analysis had higher urine levels of 11-nor-␦-9-THCOOH (132.2 ng/ml), but reported no improvement in
symptoms, a finding consistent with the conclusions of the
questionnaire, which were that chronic use of cannabis might
be required to obtain a subjective improvement in symptoms. Discussion
bradykinesia, 32 (37.7%) alleviation of muscle rigidity, and 12
Possible involvement of the cannabinoid system in PD
(14.1%) improvement of L-dopa-induced dyskinesias (Table 2
pathophysiology was shown in several experimental animal
and 3). Only 4 patients (4.7%) reported that cannabis actually
models of PD7,12–14 and in one postmortem study.15 Potential
use of cannabinoids in PD is controversial. Some authors
According to the information obtained from the patients, this
suggest that CB receptor antagonists could prove useful in the
alleviation occurred 1.7 months in average (range, 1 hour to 6
treatment of parkinsonian symptoms and L-dopa-induced dys-
months) after their first cannabis use. Patients using cannabis
kinesia,16–18 whereas CB receptor agonists could have value in
for at least 3 months reported significantly more often a mild or
reducing L-dopa-induced dyskinesia,16,18,19 which was also
substantial alleviation of their PD symptoms in general (P Ͻ
demonstrated in a recent clinical study.20 In an earlier clinic
0.001, 2 test), improvement of resting tremor (P Ͻ 0.01, 2
report, however, no effects of smoked cannabis were observed
test), bradykinesia (P Ͻ 0.01, 2 test), and muscle rigidity (P Ͻ
0.01, 2 test) (Table 2). Although there was no relationship
The aim of our study was to evaluate the frequency and
between the length of cannabis use and the effect on dyskinesia,
patterns of cannabis use in PD patients, focusing especially on
patients using cannabis on a regular basis at least once a day
possible subjective changes in cardinal motor symptoms and
reported an improvement in their dyskinesias significantly
L-dopa-induced dyskinesias. The results obtained from the
more frequently than did those who were taking cannabis less
questionnaires show that bradykinesia seems to be the symp-
than once a day (Table 3, P Ͻ 0.05, 2 test). We did not find
tom most commonly improved by cannabinoids, followed by
any influence of patients’ age (2 test), duration of PD (2 test),
muscle rigidity and tremor. In addition, 14% of our patients
part of the plant used (Kruskal-Wallis test) or whether fresh or
reported alleviation of dopaminergic-induced dyskinesias with
cannabis use. Unfortunately, we do not know how many pa-
Only 2 patients used cannabis for purposes other than alle-
tients in the anonymous study actually suffered from dyskine-
viation of PD symptoms: 1 patient used cannabis “to relieve
sias. In fact, many PD patients are not aware of dyskinesias and
depression” and 1 “to have more energy.” None of the respon-
thus cannot evaluate accurately any possible antidyskinetic
dents ever used cannabis to experience hallucinations, to re-
lieve anxiety, or to relax; however, the questionnaire did not
The late onset of cannabis action is noteworthy. Because
ask directly if they had experienced any psychoactive effects
most patients reported that improvement occurred approxi-
when using cannabis. Three patients reported that they had
mately 2 months after the first use of cannabis, it is very
discontinued using cannabis because of unspecified side ef-
unlikely that it could be attributed to a placebo reaction. The
results from the analytical part of the study (GC/MS) also
In the group of 7 patients who were using cannabis consis-
support our observation that long-term regular use of cannabi-
tently over several months, an effect of urine level of 11-nor-
noids is crucial. Possible explanations include gradual accumu-
␦-9-THCOOH (major ␦-9-THC metabolite in the urine) on
lation of low doses of highly lipophilic ␦-9-THC before reach-
bradykinesia and rigidity was apparent. In all patients in which
ing higher concentrations necessary for stimulation of
urine levels (Table 4) of 11-nor-␦-9-THCOOH were higher
movement,22 or regulations on the level of CB receptors.23–26
than 50 ng/ml (4/7), there was a reported improvement in
This observation is in contrast with the study of Sieradzan and
TABLE 4. Relationship between the concentration of 11-nor-␦-9-THCOOH in urine and change of symptoms in a subset of PD patients with long-term cannabis useMovement Disorders, Vol. 19, No. 9, 2004
colleagues,20 where the action of synthetic cannabinoid agonist
8. Zimmer A, Zimmer AM, Hohmann AG, Herkenham M, Bonner
occurred within minutes or hours after administration. The
TI. Increased mortality, hypoactivity, and hypoalgesia in cannabi-
design of these two studies, however, including the doses used,
noid CB1 receptor knockout mice. Proc Natl Acad Sci USA
was very different. Although in regular users the subjective
9. Steiner H, Bonner TI, Zimmer AM, Kitai ST, Zimmer A. Altered
improvement of symptoms seemed to correlate well with con-
gene expression in striatal projection neurons in CB1 cannabinoid
centrations of the major metabolite of ␦-9-THC found in urine,
receptor knockout mice. Proc Natl Acad Sci U S A 1999;96:5786 –
the actions of other plant cannabinoids have to be considered
because they may substantially influence the effect of ␦-9-THC
10. Ru˚zˇicˇka E. Chewing marijuana induced improvement in Parkin-
alone.27,28 The most likely is cannabidiol, which inhibits uptake
son’s disease. Parkinsonism Relat Disord 1999;5:85
and hydrolysis of anandamide and acts as a vanilloid receptor
11. Consroe P, Musty R, Rein J, Tillery W, Pertwee R. Perceived
(VR ) agonist.29 Cannabinoids may also have a protective role in
effects of cannabis smoking on patients with multiple sclerosis.
slowing down progression of a neurodegenerative process.30–32
The present study evaluating spontaneous use of natural
12. Gubellini P, Picconi B, Bari M, et al. Experimental parkinsonism
cannabis in PD patients suggests that cannabis may improve
alters endocannabinoid degradation: implications for striatal glu-tamatergic transmission. J Neurosci 2002;22:6900 – 6907.
PD symptoms and L-dopa-induced dyskinesias. Due to the
13. Silverdale MA, McGuire S, McInnes A, Crossman AR, Brotchie
illegal status of cannabis in the Czech Republic, it was impos-
JM. Striatal cannabinoid CB1 receptor mRNA expression is de-
sible to run a proper clinical trial and we had to use an
creased in the reserpine-treated rat model of Parkinson’s disease.
anonymous retrospective questionnaire-based study; we are
well aware of its limitations. Questionnaires are used quite
14. Romero J, Berrendero F, et al. Unilateral 6-hydroxydopamine
commonly in clinical research because they enable obtaining
lesions of nigrostriatal dopaminergic neurons increased CB1 re-
data from a large group of patients; however, results from this
ceptor mRNA levels in the caudate-putamen. Life Sci 1999;66:
type of study cannot be conclusive and should rather serve as a
baseline for future research. Even though a possible placebo
15. Lastres-Becker I, Cebeira M, de Ceballos ML, et al. Increased
cannabinoid CB1 receptor binding and activation of GTP-binding
reaction and other confounders (e.g., concomitant antiparkin-
proteins in the basal ganglia of patients with Parkinson’s syndrome
sonian therapy, non-standardized plant material) have to be
and of MPTP-treated marmosets. Eur J Neurosci 2001;14:1827–
taken into account, it seems that various cannabinoids or other
compounds targeting the endogenous cannabinoid system
16. Brotchie JM. CB(1) cannabinoid receptor signalling in Parkinson’s
might be useful in the treatment of PD symptoms or drug-
disease. Curr Opin Pharmacol 2003;3:54 – 61.
induced dyskinesias and this field definitely deserves further
17. Brotchie JM, Fox SH, Henry B, et al. The cannabinoid receptor
antagonist SR 141716A reduces L-dopa-induced dyskinesia in theMPTP-treated primate model of Parkinson’s disease. Br J Phar-
Acknowledgments: This study was supported by the Czech Minis-
try of Education (CEZ:J13/98:11600004 and 11100001). We thank L.
18. Brotchie JM. Adjuncts to dopamine replacement: a pragmatic
Jahoda´rˇ (Faculty of Pharmacy, Charles University, Hradec Kra´love´) for
approach to reducing the problem of dyskinesia in Parkinson’s
advice and support, P. Klemera (Faculty of Pharmacy, Charles Univer-
disease. Mov Disord 1998;13:871– 876.
sity, Hradec Kra´love´) for help with statistical analysis, J. Roth, P.
19. Fox SH, Henry B, Hill M, Crossman A, Brotchie J. Stimulation of
Mecˇı´rˇ, R. Jech, and M. Volfova´ for their clinical followup of patients
cannabinoid receptors reduces levodopa-induced dyskinesia in the
in the Movement Disorders Centre, Prague, and P. Consroe (University
MPTP-lesioned nonhuman primate model of Parkinson’s disease.
of Arizona Health Sciences Center, Tucson, AZ) for kindly providing
20. Sieradzan KA, Fox SH, Hill M, Dick JP, Crossman AR, Brotchie
JM. Cannabinoids reduce levodopa-induced dyskinesia in Parkin-
References
son’s disease: a pilot study. Neurology 2001;57:2108 –2111.
21. Frankel JP, Hughes A, Lees AJ, Stern GM. Marijuana for parkin-
1. Izzo AA, Fezza F, Capasso R, et al. Cannabinoid CB1-receptor
sonian tremor. J Neurol Neurosurg Psychiatry 1990;53:436.
mediated regulation of gastrointestinal motility in mice in a model
22. Sanudo-Pena MC, Romero J, Seale GE, Fernandez-Ruiz JJ,
of intestinal inflammation. Br J Pharmacol 2001;134:563–570.
Walker JM. Activational role of cannabinoids on movement. Eur
2. Bisogno T, Sepe N, Melck D, Maurelli S, De Petrocellis L, Di
Marzo V. Biosynthesis, release and degradation of the novel en-
23. Zhuang S, Kittler J, Grigorenko EV, et al. Effects of long-term
dogenous cannabimimetic metabolite 2-arachidonoyl glycerol in
exposure to ␦9-THC on expression of cannabinoid receptor (CB1)
mouse neuroblastoma cells. Biochem J 1997;322:671– 677.
mRNA in different rat brain regions. Brain Res Mol Brain Res
3. Fride E, Mechoulam R. Pharmacological activity of the cannabi-
noid receptor agonist, anandamide, a brain constituent. Eur J Phar-
24. Romero J, Garcia L, Fernandez-Ruiz JJ, Cebeira M, Ramos JA.
Changes in rat brain cannabinoid binding sites after acute or chronic
4. Muller-Vahl KR, Kolbe H, Schneider U, Emrich HM. Cannabis in
exposure to their endogenous agonist, anandamide, or to ␦-9-tetrhy-
movement disorders. Forsch Komplementarmed 1999;3(Suppl.):
drocannabinol. Pharmacol Biochem Behav 1995;51:731–737.
25. Rubino T, Vigano D, Massi P, et al. Chronic ␦-9-tetrahydrocan-
5. Sanudo-Pena MC, Tsou KJ, Walker JM. Motor actions of canna-
nabinol treatment increases cAMP levels and cAMP dependent
binoids in the basal ganglia output nuclei. Life Sci 1999;65:703–
protein kinase activity in some rat brain regions. Neuropharmacol-
6. Tsou K, Brown S, Sanudo-Pena MC, Mackie K, Walker JM.
26. Sim LJ, Hampson RE, Deadwyler SA, Childers SR. Effects of
Immunohistochemical distribution of cannabinoid CB1 receptor in
chronic treatment with ␦9-tetrhydrocannabinol on cannabinoid-
the rat central nervous system. Neuroscience 1998;83:393– 411.
stimulated [35S]GTPgammaS autoradiography in rat brain. J Neu-
7. Di Marzo V, Hill MP, Bisogno T, Crossman AR, Brotchie JM.
Enhanced levels of endogenous cannabinoids in the globus palli-
27. Formukong EA, Evans AT, Evans FJ. Inhibition of the cataleptic
dus are associated with a reduction in movement in an animal
effect of tetrahydrocannabinol by other constituents of Cannabis
model of Parkinson’s disease. FASEB J 2000;14:1432–1438. sativa L. J Pharm Pharmacol 1988;40:132–134. Movement Disorders, Vol. 19, No. 9, 2004
28. Bornheim LM, Kim KY, Li J, Perotti BY, Benet LZ. Effect of
The supplementary motor area (SMA) corresponds to the
cannabidiol pretreatment on the kinetics of tetrahydrocannabinol
medial aspect of Brodmann area 6 on the medial wall of the
metabolites in mouse brain. Drug Metab Dispos 1995;23:825– 831.
frontal lobe, which is essentially related to the initiation and
29. Bisogno T, Hanus L, De Petrocellis L, et al. Molecular targets for
execution of the movement.16,17 It has been shown that SMA
cannabidiol and its synthetic analogues: effect on vanilloid VR1
lesions cause various abnormalities of speech and motor func-
receptors and on the cellular uptake and enzymatic hydrolysis of
anandamide. Br J Pharmacol 2001;134:845– 852.
We recently observed a patient who developed both acquired
30. Hampson AJ, Grimaldi M, Axelrod J, Wink D. Cannabidiol and
stuttering and long-lasting gait disturbance after apparent SMA
(Ϫ)␦-9-tetrahydrocannabinol are neuroprotective antioxidants.
seizure. His stuttering and gait disturbance gradually improved
Proc Natl Acad Sci U S A 1998;95:8268 – 8273.
and almost completely resolved over 1 month.
31. Mechoulam R, Panikashvili D, Shohami E. Cannabinoids and
brain injury: therapeutic implications. Trends Mol Med 2002;8:
Case Report
32. Hampson AJ, Grimaldi M. Cannabinoid receptor activation and
A 37-year-old, right-handed man was admitted because of
elevated cyclic AMP reduce glutamate neurotoxicity. Eur J Neu-
speech and gait disturbances. He had been in good health until
28 months earlier, when he had a left anterior cerebral arteryterritorial infarction involving the left SMA and cingulate gyrus(Fig. 1A–C). At that time, he had experienced speech arrest andweakness of his right leg, which resolved over 10 days. Theetiology of the stroke was not determined, and he was dis-
Stuttering and Gait Disturbance After
charged from the hospital on aspirin. Supplementary Motor Area Seizure
Eighteen months after the stroke, he had what was consid-
ered a left SMA seizure, which consisted of sudden speech
Sun J. Chung, MD, Joo-Hyuk Im, MD,* Jae-Hong Lee, MD,
arrest, head deviation to the right, tonic posturing of the right
leg, and preserved consciousness. After the seizure, he haddifficulty with speech and walking that resolved gradually over
Department of Neurology, University of Ulsan, Asan Medical
15 days. Subsequently, he was referred to our hospital for
He denied any speech problems when he was a child. There
was no history of cardiac disease, hypertension, diabetes, ortrauma. He had no family history of stuttering. On neurologic
Abstract: Acquired stuttering is an uncommon speech disor-
examination, the cranial nerves, speech, motor power, and
der. Supplementary motor area (SMA) lesions have been re-
sensation were normal. On awakening 3 days after hospital
ported to be directly or indirectly related to acquired stuttering
admission, he was unable to walk alone; postural stability was
and various types of motor dysfunction. We report on a patient
markedly impaired with generalized paucity of body move-
who presented with both acquired stuttering and long-lasting
ment. Motor strength was normal. He was barely able to make
gait disturbance after SMA seizure. 2004 Movement Dis-
steps and only with assistance. His gait improved gradually and
normalized over 20 days. During this episode, he showed nospeech disturbance. An electroencephalogram (EEG), brain
Key words: supplementary motor area; stuttering; gait dis-
magnetic resonance angiogram (MRA), transcranial Doppler,
and echocardiogram were all normal. Although the exact eti-ology of his gait disturbance was not found, it was clinically
Stuttering has been defined as a disruption in the fluency of
suspected that this episode was a postictal manifestation of an
verbal expression, which is characterized by involuntary repe-
SMA seizure. The patient was placed on valproic acid and
titions or prolongations in the utterance of short speech ele-
aspirin and did well without recurrent seizures or any other
ments—namely, sounds, syllables, and words of one syllable.1
Developmental stuttering typically begins in childhood or early
On the day of his second admission, he developed sudden
adolescence.2,3 The etiology of developmental stuttering re-
speech and gait disturbances after the SMA seizure thatlasted for approximately 5 minutes. On examination, he
mains elusive. New stuttering in adulthood, or acquired stut-
showed severe stuttering with an abnormal protruding move-
tering, has been reported in a variety of diseases, including
ment of his lips when he tried to speak (see video Segment
strokes,4–12 Parkinson’s disease,13,14 progressive supranuclear
1). The stuttering did not improve with repetitive practice. It
palsy,14 Alzheimer’s disease,15 and trauma.6,12,15
was similar in severity on both spontaneous speech and withrepetition. The stuttering was accompanied by severe slow-ness of orolingual and velopharyngeal movement. The dys-
This article contains supplementary video clips, available at http://
fluency of his speech was noted through entire sentences, but
www.interscience.wiley.com/jpages/0885-3185/suppmat.
mainly at the beginning of words, phrases, or sentences.
*Correspondence to: Dr. Joo-Hyuk Im, Department of Neurology,
When he read a book aloud, the severity of the stuttering
Asan Medical Center, 388-1, Poongnap-dong, Songpa-gu, Seoul, South
diminished and speech was monotonous. The speech distur-
bance was also noted when he sang a familiar song. We also
Received 7 April 2003; Revised 19 September 2003; Accepted 10
detected severe bilateral body bradykinesia and gait distur-
Published online 22 April 2004 in Wiley InterScience (www.
bance. The bradykinesia was initially generalized but later
interscience.wiley.com). DOI: 10.1002/mds.20136
was noted mainly in the lower extremities. He was initially
Movement Disorders, Vol. 19, No. 9, 2004
LA DEPRESIÓN NOTA IMPORTANTE La depresión es un tema tan amplio y tenemos tan poco tiempo, que obviamente tendremos que resumir y condensar a muchas ideas. OBSERVACIONES PRELIMINARES I. La consejería bíblica no es para los “expertos”. Es para cada hijo de Dios que desea ser obediente y ayudar a otros a que también lo sean (Romanos 15:14). II. En la consejería, el que acon
IMMUNE FUNCTION IN ADULT HEART TRANSPLANT PATIENTS REFLECTS RISK FOR ORGAN REJECTION AND INFECTION Data from 76 patients over 3 years confirms value of assay of cell-mediated immunity Boston, MA, April 11, 2008 – Results of an analysis of three years of data on the monitoring of cell- mediated immunity (CMI) in adult patients undergoing heart transplantation at the University
 5. Powers JM. Blepharospasm due to unilateral diencephalon infarc-
6. Keane JR, Young JA. Blepharospasm with bilateral basal ganglia
infarction. Arch Neurol 1985;42:1206 –1208.
5. Powers JM. Blepharospasm due to unilateral diencephalon infarc-
6. Keane JR, Young JA. Blepharospasm with bilateral basal ganglia
infarction. Arch Neurol 1985;42:1206 –1208. 28. Bornheim LM, Kim KY, Li J, Perotti BY, Benet LZ. Effect of
The supplementary motor area (SMA) corresponds to the
cannabidiol pretreatment on the kinetics of tetrahydrocannabinol
medial aspect of Brodmann area 6 on the medial wall of the
metabolites in mouse brain. Drug Metab Dispos 1995;23:825– 831.
28. Bornheim LM, Kim KY, Li J, Perotti BY, Benet LZ. Effect of
The supplementary motor area (SMA) corresponds to the
cannabidiol pretreatment on the kinetics of tetrahydrocannabinol
medial aspect of Brodmann area 6 on the medial wall of the
metabolites in mouse brain. Drug Metab Dispos 1995;23:825– 831.