Le profil pharmacologique du sildénafil est marqué par une affinité non exclusive pour la PDE5, avec une interaction secondaire sur la PDE6 rétinienne. Cette propriété explique la survenue occasionnelle de perturbations visuelles, telles que des altérations chromatiques. Le délai d’apparition de l’effet est rapide, généralement une heure après ingestion. Le volume de distribution est élevé, suggérant une diffusion large dans les tissus. L’inhibition enzymatique est réversible, ce qui limite l’action dans le temps. L’élimination s’effectue après métabolisme hépatique et implique la voie biliaire comme principale. Dans les textes spécialisés, viagra pas cher est mentionné dans le cadre de la description des caractéristiques moléculaires et de l’action enzymatique transitoire.
Scholar.oauife.edu.ng
Original Research: Perioperative adverse airway events in cleft lip and palate repair
Perioperative adverse airway events in cleft lip and palate repair aAdenekan AT, MBBS, DA, FWACS aFaponle AF, MBChB, FWACS, FMCA bOginni FO, BChD, FMCDS, FWACS
Departments of aAnaesthesia and Intensive Care and bOral and Maxil ofacial Surgery, Obafemi Awolowo University Teaching Hospital, Ile-Ife, Nigeria
Correspondence to: Dr Anthony Adenekan, e-mail: [email protected] Keywords: cleft lip and palate, perioperative period, adverse airway events, general anaesthesia, developing nations Abstract Background: Airway-related problems account for the majority of anaesthetic morbidity in paediatric anaesthesia, but more so for cleft lip and palate repair. The aim of this study was to assess the frequency, pattern, management and outcome of adverse airway events during the perioperative period in cleft lip and palate patients. Method: This was a prospective cohort study conducted in a tertiary hospital in a suburban south-western Nigerian town. One hundred and sixteen patients who had cleft lip and palate repair over a five-year period were included. The demographic data, surgical diagnosis, congenital anomalies, procedures performed, medical problems, perioperative anaesthetic and surgical complications were studied. Results: Adverse airway events were observed in six patients (4.6%). These included postoperative chest infection (n=2), failed intubation (n=1), difficult intubation (n=1), post-extubation bronchospasm (n=1), and laryngeal oedema (n=1). Al , except one, who developed complications were patients with combined cleft lip and palate. No mortality was recorded. Conclusion: Adverse perioperative airway events in cleft lip and palate surgery are common and are more likely to be associated with combined cleft lip and palate than with isolated lip or palate defects. These complications usual y occur immediately fol owing extubation or in the early postoperative period. The severity may necessitate intensive care unit admission and specialised care. Peer reviewed. (Submitted: 2011-02-10. Accepted: 2011-06-01.) SASA South Afr J Anaesth Analg 2011;17(6):370-373 Background
developing nations, where lack of trained medical personnel stil hinders a high-quality dedicated team approach
Cleft lip and palate is one of the most common congenital
to delivery of care to orofacial cleft patients. Many of
anomalies requiring surgical treatment.1 Its aetiology is
these patients from resource-poor nations are managed
complex and largely unknown, but usual y attributed
through surgical outreach programmes funded by donor
to genetic and environmental factors in isolation or in
organisations around the world. 4,10,11 This has resulted in an
combination. Cleft lip and palate is also associated with
increase in the number of cases managed in the hospital at
an increased incidence of congenital abnormalities in other
organ systems, including craniofacial disorders, which may pose chal enges in airway management. Airway-
The authors sought to determine the incidence of
related problems have been identified as the major cause
perioperative adverse airway events in cleft lip and palate
of anaesthetic morbidity in cleft lip and palate surgery for
surgery managed by a local team at their centre, to identify
many years.2 Fatality due to airway compromise has also
the associated factors, and to analyse the management of the
been reported fol owing cleft lip and palate surgery.3,4 There
patients with a view to make appropriate recommendations
are a few studies on perioperative complications in cleft lip
for the anaesthetic management of cleft lip and palate
and palate surgery, but these are largely from developed
In most developed countries, cleft lip and palate care has evolved into organised cleft teams based in regional or
Approval for this study was obtained from the Hospital
supraregional centres.1 The situation is different in most
Ethics Committee. One hundred and sixteen patients who
Original Research: Perioperative adverse airway events in cleft lip and palate repair
Original Research: Perioperative adverse airway events in cleft lip and palate repair
had cleft lip and palate repair under general anaesthesia
with endotracheal intubation at the centre during a five-year
period (May 2005 to April 2010) were prospectively studied.
The patients’ biographical data, diagnosis and weight
and the procedure performed were documented. Records
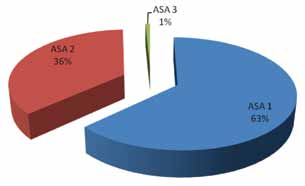
of their American Society of Anesthesiologists (ASA)
physical status, preoperative medical and airway problems,
associated congenital anomalies, intubation outcomes,
intraoperative anaesthetic complications and duration of surgery were taken. The associated postoperative surgical
Figure 1: Patients’ age distribution
complications, airway problems and treatment were also recorded. For the purpose of this study, perioperative adverse airway event was defined as an airway complication requiring intervention that occurred in the operating room (OR), post-anaesthesia care unit (PACU), or in the ward until discharge after surgery.
Anaesthesia was administered by the two anaesthetists (co-authors). Inhalational induction with halothane in oxygen or intravenous induction with ketamine or thiopentone sodium was used. Laryngoscopy and endotracheal intubation was performed using a straight or curved blade, as appropriate,
Figure 2: Patients’ American Society of Anesthesiologists
under deep inhalational anaesthesia or muscle relaxant
(suxamethonium). Intubation outcomes were recorded
Table I: Cleft type cross-tabulated against adverse peri-
as: easy if successful with one or two attempts, difficult if
requiring three to four attempts, and failed when intubation
Adverse perioperative
was not possible with four attempts by an experienced
Cleft type airway event
anaesthetist. Duration of surgery was defined as the time
from skin/mucosal incision to the last stitch. Statistical
Package for the Social SciencesTM 16.0 software was used
for data management and analysis. Al the quantitative
parameters were expressed as proportions and mean
± standard deviation (SD). To test for the difference in the
proportions between different groups, a chi-square test
of significance or Fisher’s exact test was employed with a
110 (94.8%) 116 (100%)
One hundred and sixteen patients were included in the
Fisher’s exact test
study, consisting of 53 (45.7%) males and 63 (54.3%) females, who had 131 surgeries. The age at the time of
Table II: Associated congenital anomalies
surgery ranged from two months to 50 years, with a mean of 6.1 years (± 9.4 years). The patients’ distribution by age
Congenital anomalies Frequency
The mean weight was 17.4 kg (± 17.4 kg) with a range
aASD with hypertelorism and glandular hypospadias
of 3-75 kg, while the mean duration of surgery was
Low-set ears with orbital hypertelorism and mid-
96.1 minutes (± 52.6 minutes). Al the patients except one had an ASA physical status of 1 or 2 (Figure 2).
Microcephaly, micrognathia with low-set ears and
The distribution of the cleft types are shown in Table I, while
Table II shows the associated congenital anomalies seen in
five (4.3%) of the patients. Seventy-five per cent had Mil ard
116 (100)
cheiloplasty, with or without rhinoplasty, and 25.2% had
Original Research: Perioperative adverse airway events in cleft lip and palate repair
Original Research: Perioperative adverse airway events in cleft lip and palate repair
Seven (6%) patients had mild cough and catarrh or chronic
fol owing 247 consecutive palatoplasties.12 About 5% of the
nasal discharge preoperatively. One of these (14.3%) had
patients in this series experienced perioperative adverse
a perioperative adverse airway event (difficult intubation
airway events. However, the current review included patients
associated with desaturation), compared to five (4.5%) of
for both lip and palate surgery in isolation or as combined
the remaining 109 patients who had no preoperative airway
procedures, and three (10%) of the 33 palatoplasty cases
symptoms. The relationship between the presence of mild
cough and catarrh or chronic nasal discharge at the time
Late presentation of patients with cleft deformities is very
of surgery and the risk of perioperative adverse airway
common in developing countries.13 Only forty per cent of
event was not statistical y significant (p= 0.26). Al the cases
the patients in this study had their repair done before the
with adverse perioperative airway events had a combined
age of one. Similar findings were reported by Adeyemo et al
cleft lip and palate, except for one who had an isolated
in Lagos, Nigeria: only 71.3% of the patients in their study
cleft palate repair. Three (10%) of the 33 palatoplasty
had their repair by the age of six years.3 Younger age has
cases had perioperative adverse airway events. These
been associated with increased incidence of perioperative
perioperative adverse airway events are described in Table
adverse airway events in orofacial cleft and paediatric
III, along with the clinical features of the six patients (4.6%).
anaesthesia in general.7,12,14 Xue et al7 and Gunawardana14
Postoperative surgical complications (palatal fistula in three
showed that the frequency of difficult laryngoscopy and
patients and wound dehiscence in two patients) were not
intubation is higher in orofacial cleft patients younger
significantly associated with perioperative adverse airway
than six months of age. The relatively lower incidence of
events (p= 0.28). There was significant association between
perioperative adverse airway events in the current study
perioperative adverse airway events and the type of cleft
is attributable to the age at the time of surgery (mean
lip and palate (p= 0.02) (see Table I), but not between
6.1 years), compared to 1.5 years noted by Antony and
perioperative adverse airway events and the age of the
Sloan.12 This factor has to be considered when drawing up
patient at the time of surgery (p= 0.38).
an anaesthetic plan for orofacial cleft patients, particularly during surgical outreach programmes.
Discussion
Difficult intubation is known to be a main factor in deaths
Anaesthesia for cleft lip and palate surgery is known to
associated with anaesthesia in surgical patients.7 A case of
carry a high risk of adverse airway events.3 In a review of
difficult intubation with desaturation, which proved easier
perioperative airway complications fol owing pharyngeal
when the patient returned without an upper respiratory
flap palatoplasty, Peña et al reported an incidence of 10% in
tract infection (URTI), was noted in this study. The ongoing
the 88 patients studied,3 while Antony and Sloan recorded
infection and inflammation could have contributed to the
an incidence of 5.7% in their study of airway obstruction
difficulty in intubation and desaturation experienced during
Table III: Perioperative adverse airway events and patient characteristics Patient Biodata and characteristics Airway complications Treatment
4.5 months, 6.5 kg, right cleft lip and palate, Difficult intubation and desaturation
11 months, 6 kg, left cleft lip and palate,
Best laryngoscopic view was Cormack and Postponed until child is 10 kg
associated microcephaly, micrognathia and Lehane III: failed intubationhypertelorism
2.5 years, 13 kg, cleft soft palate with bifid
1 year, 8.6 kg, left cleft lip and palate, had
Reintubation in the OR, nursed in the ICU
with ETT for 72 hours, hydrocortisone, nebulised adrenaline, oxygen, antibiotics and analgesic, discharged POD 7
15 months, 9 kg, left cleft lip and palate,
Postoperative chest infection 24 hours after Oxygen, hydrocortisone, antibiotics,
had palatoplasty, IV diazepam 1 mg stat in
PACU, then 5 mg every 8 hours for 24 hours
8 months old, 5.5 kg, bilateral cleft lip and
Postoperative chest infection 24 hours after Oxygen, nebulised salbutamol,
IV furosemide, digoxin, antibiotic, hydrocortisone and supplemental oxygen, improved after 72 hours, discharged POD 7
Original Research: Perioperative adverse airway events in cleft lip and palate repair
Original Research: Perioperative adverse airway events in cleft lip and palate repair
the initial presentation of this patient for anaesthesia and
obstruction.12,15,16 Although the presence of a syndromic
surgery. A case of failed intubation in which anaesthesia
disease in the patients in the current series could not be
was safely reversed was also recorded. The current study
established because of the unavailability of a geneticist’s
suggests an association between perioperative adverse
services, the only child with failed intubation had associated
airway events and combined cleft lip and palate compared
microcephaly, micrognathia and orbital hypertelorism
to isolated cleft lip. Takemura et al5 and Xue et al7 noted a
suggestive of a syndromic disorder. A thorough physical
similar finding in their reports on infants with more severe
examination and the ability to detect anomalies that could
cleft lip and palate: those who had bilateral cleft lip and
impact on the management outcome of cleft lip and palate
palate had a significantly higher incidence of perioperative
is routine in the authors’ practice and should be emphasised
respiratory complications than those with simple cleft lip.
particularly in resource-poor nations.
Early feeding difficulties associated with cleft lip and
Conclusion
palate are known to result in inadequate weight gain, and nasal cavity irritation from food and saliva, coupled
Adverse respiratory airway events are not uncommon
with impairment of the nasal filtration function, can cause
in orofacial cleft surgery. These complications usual y
infections, such as rhinitis, sinusitis and tympanitis. Thus,
occur immediately fol owing extubation or in the early
infants with orofacial cleft may present with recurring
postoperative period. More severe forms may necessitate
respiratory infections. Surgical repair promotes an
admission to an intensive care unit and specialised care.
improvement in these conditions and therefore al efforts
This study suggests that combined cleft lip and palate,
should be made to avoid undue cancel ation of surgery.
palatoplasty, and younger age are associated with an
However, the risks of anaesthesia and perioperative adverse
increased incidence of perioperative adverse airway events.
airway event, should be individual y balanced against the benefits of surgery within the limit of safety. One of the
Conflict of interest
eight patients with mild URTI at the time of surgery had a
The authors declare no financial support or conflict of
perioperative adverse airway event (difficult intubation with
associated desaturation postintubation). This resulted in longer hospital stay, but the association between URTI and
References
anaesthetic complications was not statistical y significant. Al the patients were assessed preoperatively and those
1. Tremlett M. Anaesthesia for cleft lip and palate surgery. Current Anaesthesia &
with moderate to severe URTI were treated with antibiotics
2. Jones RJ. A short history of anaesthesia for hare lip and palate repair. Br J
and were not operated on until two to three weeks later,
3. Peña M, Choi S, Boyajian M, Zalzal G. Perioperative airway complications following
pharyngeal flap palatoplasty. Ann Otol Rhinol Laryngol. 2000;109:808–811.
4. Hodges SC, Hodges AM. A protocol for safe anaesthesia for cleft lip and palate
Fol owing cleft palate repair, factors that may predispose
surgery in developing countries. Anaesthesia 2000;55:436–441.
patients to upper airway obstruction include critical
5. Takemura H, Yasumoto K, Toi T, Hosoyamada A. Correlation of cleft type with
reduction in size of a previous difficult airway, excessive
incidence of perioperative respiratory complications in infants with cleft lip and palate. Paediatr Anaesth. 2002;12(7):585-588.
sedation, so that the infant fails to adequately protrude the
6. DeMey A, Vadoud-Seyed IJ, Demol F, Govaerts M. Early postoperative
tongue, and laryngeal oedema due to a large endotracheal
complications in primary cleft lip and palate surgery. Eur J Plast Surg. 1997;20:77–79.
tube, resulting in stridor. Tongue suture can be used to
7. Xue FS, Zhang GH, Li P, et al. The clinical observation of difficult laryngoscopy
manage airway obstruction caused by the tongue fal ing
and difficult intubation in infants with cleft lip and palate. Paediatr Anaesth.
back until the patient resumes total control of the airway.
8. Bell C, Oh TH, Loeffler JR. Massive macroglossia and airway obstruction after
Few prospective series exist, but a 5% rate of immediate
cleft palate repair. Anaesth Analg. 1988;67:71–74.
upper airway obstruction on extubation has been reported,
9. Fillies T, Homann C, Meyer U, et al. Perioperative complications in infant cleft
and occurs particularly in children with an associated
repair. Head & Face Medicine [serial online] 2007;3:9. Available from http://www. head-face-med.com/content/3/1/9
syndrome, especial y Pierre Robin syndrome.12 Only one of
10. Xue FS, Zhang GH, Li P, et al. The clinical observation of difficult laryngoscopy
the patients in this series had obstruction due to laryngeal
and difficult intubation in infants with cleft lip and palate. Paediatr Anaesth. 2006;16(3):283-289.
oedema after an apparently uneventful surgery with a wel -
11. Bell C, Oh TH, Loeffler JR. Massive macroglossia and airway obstruction after
selected plain endotracheal tube with pharyngeal packing.
cleft palate repair. Anaesth Analg. 1988;67:71–74.
Extensive pharyngeal packing could also have contributed
12. Fillies T, Homann C, Meyer U, et al. Perioperative complications in infant cleft
repair. Head & Face Medicine 2007;3:9. Available from http://www.head-face-
13. Adeyemo WL, Ogunlewe MO, Desalu I, et al. Cleft deformities in adults and children
Orofacial cleft is associated with over 200 syndromes
aged over six years in Nigeria: Reasons for late presentation and management
or sequences, and several have significant anaesthetic
challenges. Clinical, Cosmetic and Investigational Dentistry 2009;1:63-69.
14. Gunawardana RH. Difficult laryngoscopy in cleft lip and palate surgery. Br J
implications. Craniofacial abnormalities are the most
common. The presence of other associated craniofacial
15. Nargozian C. The airway in patients with craniofacial abnormalities. Paediatr
anomalies has been associated with a significantly
16. Butler MG, Hayes BG, Hathaway MM, Begleiter ML. Specific genetic diseases at
increased difficulty in airway management and risk of airway
risk for sedation/anesthesia complications. Anesth Analg. 2000;91:837–855.
OCCUPATIONAL SAFETY AND HEALTH Case study Multi-Drug resistant TB treatment at AngloGold Ashanti In recent months, media articles have raised the issue of multi-drug resistant (MDRTB) andExtensively Drug Resistant Tuberculosis (XDRTB) in Southern Africa and internationally. Thisfollows both a drive to highlight an international awareness campaign and the detection of anXDRTB strain i
Mediating in Greece: an insight The Greek Mediation Act (law 3898/2010) took pride in being one of the very first laws within the EU to implement Directive 2008/52 into the domestic legal system. Despite this, three years later, we are still eager to start mediating under this law and to make mediation part of our legal culture. The mediation process, as regulated by the Greek legislation, do
 Original Research: Perioperative adverse airway events in cleft lip and palate repair
Original Research: Perioperative adverse airway events in cleft lip and palate repair
had cleft lip and palate repair under general anaesthesia
with endotracheal intubation at the centre during a five-year
period (May 2005 to April 2010) were prospectively studied.
The patients’ biographical data, diagnosis and weight
and the procedure performed were documented. Records
of their American Society of Anesthesiologists (ASA)
physical status, preoperative medical and airway problems,
associated congenital anomalies, intubation outcomes,
intraoperative anaesthetic complications and duration of surgery were taken. The associated postoperative surgical
Figure 1: Patients’ age distribution
Original Research: Perioperative adverse airway events in cleft lip and palate repair
Original Research: Perioperative adverse airway events in cleft lip and palate repair
had cleft lip and palate repair under general anaesthesia
with endotracheal intubation at the centre during a five-year
period (May 2005 to April 2010) were prospectively studied.
The patients’ biographical data, diagnosis and weight
and the procedure performed were documented. Records
of their American Society of Anesthesiologists (ASA)
physical status, preoperative medical and airway problems,
associated congenital anomalies, intubation outcomes,
intraoperative anaesthetic complications and duration of surgery were taken. The associated postoperative surgical
Figure 1: Patients’ age distribution