Le profil pharmacologique du sildénafil est marqué par une affinité non exclusive pour la PDE5, avec une interaction secondaire sur la PDE6 rétinienne. Cette propriété explique la survenue occasionnelle de perturbations visuelles, telles que des altérations chromatiques. Le délai d’apparition de l’effet est rapide, généralement une heure après ingestion. Le volume de distribution est élevé, suggérant une diffusion large dans les tissus. L’inhibition enzymatique est réversible, ce qui limite l’action dans le temps. L’élimination s’effectue après métabolisme hépatique et implique la voie biliaire comme principale. Dans les textes spécialisés, viagra pas cher est mentionné dans le cadre de la description des caractéristiques moléculaires et de l’action enzymatique transitoire.
Dietary silicon intake is positively associated with bone mineral density in men and premenopausal women of the framingham offspring cohort
JOURNAL OF BONE AND MINERAL RESEARCH Volume 19, Number 2, 2004 Published online on December 16, 2003; doi: 10.1359/JBMR.0301225 2004 American Society for Bone and Mineral Research
Dietary Silicon Intake Is Positively Associated With Bone Mineral Density
in Men and Premenopausal Women of the Framingham Offspring Cohort
Ravin Jugdaohsingh,1,6 Katherine L Tucker,2,6 Ning Qiao,2 L Adrienne Cupples,3 Douglas P Kiel,4 and Jonathan J Powell1,5
ABSTRACT: The role of dietary silicon in bone health in humans is not known. In a cross-sectional, population-based study (2847 participants), associations between dietary silicon intake and BMD were investigated. Dietary silicon correlated positively and significantly with BMD at all hip sites in men and premenopausal women, but not in postmenopausal women, suggesting that increased silicon intake is associ- ated with increased cortical BMD in these populations. Introduction: Osteoporosis is a burgeoning health and economic issue. Agents that promote bone formation are widely sought. Animal and cellular data suggest that the orthosilicate anion (i.e., dietary silicon) is involved in bone formation. The intake of silicon (Si, ϳ30 mg/day) is among the highest for trace elements in humans, but its contribution to bone health is not known. Materials and Methods: In a cross-sectional, population-based study, we examined the association between silicon intake and bone mineral density (BMD) in 1251 men and 1596 pre- and postmenopausal women in the Framingham Offspring cohort (age, 30 – 87 years) at four hip sites and lumbar spine, adjusting for all potential confounding factors known to influence BMD and nutrient intake. Results: Silicon intake correlated positively with adjusted BMD at four hip sites in men and premenopausal women, but not in postmenopausal women. No significant association was observed at the lumbar spine in any group. Categorical analysis by Si intake, or energy-adjusted Si intake, supported these findings, and showed large differences in BMD (up to 10%) between the highest (Ͼ40 mg Si/day) and lowest (Ͻ14 mg Si/day) quintiles of silicon intake. A significant association at the lumbar spine in men was also observed. Further analyses indicated that some of the effects seen for moderate consumption of alcoholic beverages on BMD might be attributed to Si intake. Conclusions: These findings suggest that higher dietary silicon intake in men and younger women may have salutary effects on skeletal health, especially cortical bone health, that has not been previously recognized. Confirmation of these results is being sought in a longitudinal study and by assessment of the influence of silicon intake on bone markers in this cohort. J Bone Miner Res 2004;19:297–307. Published online on December 16, 2003; doi: 10.1359/JBMR.0301225 Key words: silicon, bone mineral density, bone formation, dietary intake, beer INTRODUCTION
SILICON, AS THE soluble silicate anion [orthosilicic acid;
*Preliminary results from this study were presented at the 23rd
tant in bone formation in both animal and cellular
Annual Meeting of the American Society for Bone and Mineral
models.(1–4) In 1972, Carlisle(2) and, Schwarz and Milne(3)
Research in Phoenix, Arizona, October 12–16, 2001, and an abstractwas published (Tucker KL, Kiel DP, Powell JJ, Qiao N, Hannan MT,
showed in independent animal studies that silicon defi-
Jugdaohsingh R 2001 Dietary silicon and bone mineral density: The
ciency had profound negative influences on skeletal devel-
Framingham Study. J Bone Miner Res 16:S1;S510). The final data of
opment. The development of both extracellular matrix (col-
this manuscript were presented at the International Bone Mineral
lagen) and bone mineral (hydroxy-apatite) was suboptimal
Society meeting in Osaka, Japan, June 3–7, 2003, and an abstract wasalso published (Jugdaohsingh R, Tucker KL, Kiel DP, Qiao N, Powell,
with silicon depletion.(2,3) Although silicate transporters
JJ 2003 Silicon intake is a major dietary determinant of bone mineral
have been identified in lower organisms with high silicon
density in men and pre-menopausal women of the Framingham Off-
requirements,(5) as have silicate responsive and controlling
spring cohort. Bone 32:S192).
proteins,(6,7) considerably less is known about this ion in
The authors have no conflict of interest.
1Gastrointestinal Laboratory, The Rayne Institute, St Thomas’ Hospital, London, United Kingdom; 2Jean Mayer U.S. Department of
Agriculture Human Nutrition Research Centre on Aging, Tufts University, Boston, Massachusetts, USA; 3Department of Biostatistics,Boston University School of Public Health, Boston, Massachusetts, USA; 4Harvard Medical School Division on Aging, HRCA Researchand Training Institute, Boston, Massachusetts, USA; 5MRC Human Nutrition Research, Elsie Widdowson Laboratory, Cambridge, UnitedKingdom; 6These authors contributed equally. JUGDAOHSINGH ET AL.
mammalian species, especially in humans. In particular, the
MATERIALS AND METHODS
complexities of aqueous silicate chemistry and silicon anal-
ysis have inhibited detailed mechanistic studies with phys-iological levels of silicon. Nonetheless, low levels of ortho-
Subjects in this study were participants in the Framing-
silicic acid, at typical plasma concentrations after ingestion
ham Osteoporosis Study, drawn from the Framingham Off-
of silicon-containing foods, stimulate human osteoblasts
spring cohort. The original population-based Framingham
and osteoblast-like cells to secrete type I collagen and other
Heart Study was initiated in 1948 to examine the risk factors
markers involved in bone cell maturation and bone forma-
for heart disease.(18) The Original cohort constituted a two-
tion.(4) Soluble silicate may stabilize aqueous hydroxy-
thirds sampling of the households in Framingham, MA.(18)
radical species,(8) and some have suggested silicate involve-
The Offspring cohort was established in 1971 and consists
of the children (and their spouses) of the Original cohort
pathway(9) during type I collagen formation. Others have
members. Members return every 4 years for a physicalexamination and to complete a series of questionnaires and
suggested a structural role in the cross-linking and stabili-
tests. In the fifth (1991–1995) and sixth (1995–1999) study
zation of collagen and glycoaminoglycans.(10) Further stud-
visits (or examination cycles), there were 3799 participants
ies are required at the molecular and mechanistic level, but
(1605 men and 1813 women, 30 – 87 years of age), of which
the finding that orthosilicic acid stimulates human osteo-
1251 men and 1596 women had completed two semiquan-
blasts is important and consistent with the few small studies
titative food frequency questionnaires (FFQ) and had BMD
in human subjects(11,12) and the numerous studies in
measurements performed between 1996 and 2001. All par-
ticipants with dietary intake data and BMD measurement
The average daily dietary intake of silicon in the West-
were included in this study; otherwise, there were no ex-
ern world is about 20 –50 mg/day, although it is lower in
clusion criteria (i.e., for bone diseases, other diseases,
women (24 Ϯ 12 mg/day at the age of 26 –39 years) than
women with premature menopause or bilateral ovariectomy,
men (37 Ϯ 23 mg/day at the age of 26 –39 years), and
or subjects on treatments for bone diseases or other dis-
decreases with age (ϳ0.1 mg lower for each year after
eases). The study was approved by the Institutional Review
26 –39 years of age).(13,14) Recently, we demonstrated
Board for Human Research at Boston University (Boston,
that common silicon-rich foods effectively deliver bio-
MA, USA) and the Hebrew Rehabilitation Center for Aged
available silicon after their ingestion by human volun-
(Boston, MA, USA). Written informed consent was ob-
teers.(13) Phytolithic (plant-based) silicates seem to un-
dergo hydrolysis, forming orthosilicic acid, in the
gastrointestinal tract, because soluble orthosilicic acid,but not polysilicate, is well absorbed in human sub-
Dietary silicon intake and major food contributors to Si
jects.(15) Major sources of dietary Si in the Western world
intake in this population have been previously described by
are cereals/grains and their products (e.g., breakfast ce-
the authors.(13) Usual dietary intake, in the Offspring cohort,
reals, bread, beer), some fruits and vegetables (e.g., ba-
was assessed using the Willett semiquantitative 126-item
nanas, raisins, beans, lentils), and unfiltered drinking
FFQ.(19) This questionnaire has been validated for many
water.(13) It seems likely that food preparation in the
nutrients and in several populations.(19) Before the fifth
Western world has reduced our silicon exposure in recent
(1991–1995) and sixth (1995–1999) study visits, question-
times,(16) especially due to the treatment of drinking
naires were mailed to the subjects, who were asked to
water, the processing of cereals, and possibly the hydro-
complete them based on their pattern of intake over the
ponic growth of vegetables.(17) As for all nutrients, how-
previous year and to bring them to their appointments(visits). A completed FFQ was available from both study
ever, individual dietary habits mostly dictate our expo-
visits. The average intake from the two questionnaires was
used. Completed questionnaires were excluded, as previ-
We showed recently that the silicon content of foods is a
ously reported,(13,20) if calculated energy intakes were be-
proxy for silicon absorption in human subjects,(13) so the
low 2.51 MJ/day, above 16.74 MJ/day for women and 17.57
aims of this study were, first, to determine the relationship
MJ/day for men, or if more than 12 food items were left
between dietary Si intake and bone mineral density (BMD)
blank. Processing of the forms to obtain total daily energy
(adjusting for all potential confounders known to affect
intakes and food intake was carried out at Harvard Univer-
BMD and nutrient intake, with and without the inclusion of
alcohol intake) and to assess whether the relationship holdsacross different bone sites, gender, and menopausal status.
We also examined the association between sex-specific
Silicon values per 100 g edible portion of each of the 278
quintiles of Si intake and BMD to investigate the possibility
food items in the FFQ were obtained from a previous review
of nonlinear relationships. Second, we determined whether
by Pennington.(14) The Si contents of composite foods were
or not the positive relation between the moderate ingestion
calculated from the individual components of the food.
of alcoholic beverages and BMD, observed in this cohort,
However, where values for reported Si levels of foods
could be explained by Si intake. We hypothesized that there
varied between laboratories by 3-fold or more, additional
would be a positive association between silicon intake and
analyses were made independently by the authors (King’s
College London), and with the exception of liquor (0.13 Ϯ
SILICON AND BMD
0.04 mg/100 g; range, 0.06 – 0.21 mg/100 g), beer (2.06 Ϯ
of calcium (mg) and/or vitamin D supplements (IU) was
0.70 mg/100 g; range, 0.96 –3.94 mg/100 g), and orange
obtained from the supplement section of the FFQ. Estrogen
juice (0.01 Ϯ 0.01 mg/100 g; range, 0.0004 – 0.25 mg/100
use in women was defined as those currently receiving
g), our data correlated highly (r ϭ 0.82; n ϭ 28) with those
estrogen therapy at the time of BMD measurements, with
of Varo (extensively cited by Pennington(14)). Therefore, as
continuous use for Ն1 year.(24) Information on the use of
reported previously,(13) we chiefly used the values of Varo
other osteoporosis medication (e.g., bisphosphonates, selec-
with our values for orange juice, beer, and liquor, in the
tive estrogen receptor modulators, calcitonin) was obtained
database. These values (mg Si/100 g food) were entered into
during the course of the bone density measurements (1996 –
a database program in the Dietary Assessment and Epide-
2001). Other drugs that may affect BMD (corticosteroids,
miology Research Program at Tufts University (Boston,
thyroxine) were not included in the models. Total energy
MA, USA) and corrected for the weight of each food item
intake in calories (converted to Joules), total protein intake
reported for each individual participant. Because the Si
(g), dietary calcium intake (mg), dietary vitamin D intake
content of foods was recorded on a dry weight basis, levels
(IU), magnesium (mg) and potassium intake (mg), and
of Si in brown rice, white rice, and pasta were corrected by
intake of alcohol (see above) were averaged from the two
0.30, 0.39, and 0.30, respectively, based on United States
FFQs from the 1991–1995 and 1995–1999 study visits.
Department of Agriculture (USDA) published (raw to
Smoking status (current, past, or nonsmoker) was obtained
cooked) conversions.(21) The values (mg Si) for each food
at 1995–1999 study visit. Finally, to control for potential
item were summed to obtain total Si intake per person per
seasonal effects on BMD measures, a categorical variable
day in each of two study visits (1991–1995 and 1995–1999).
for time of BMD measurement was created.(20) July, Au-
The average silicon intake (mg/day) from the two visits was
gust, and September were coded as summer; October, No-
vember, and December as fall; January, February, andMarch as winter; and April, May, and June as spring.
Intake (servings per day, per week, or per month) of beer,
wine, and liquor were averaged from the two FFQs from the
All analyses were conducted separately for men and pre-
1991–1995 and 1995–1999 study visits. One serving of beer
and postmenopausal women and were performed with PC
represented one 356-ml glass, bottle, or can, while one
SAS for Windows (version 8.1; SAS Institute Inc., Cary,
serving of wine (red or white) represented one 4-oz glass
NC, USA). We initially investigated the association be-
(118 ml), and one serving of liquor represented one drink or
tween silicon intake and BMD (at the four hip sites and
lumbar spine) using Si as a continuous variable in thegeneral linear models. Because the distribution of silicon
intake was found to be skewed, the data were transformedby natural logarithm (ln). Measures of BMD at the hip sites
BMD was measured between 1996 and 2001, during the
and lumbar spine were regressed on the ln value of the
course of the sixth and seventh examination cycles, using
average silicon intake from the two exams. Adjustment was
DXA (Lunar DPX-L; Lunar Radiation Corp, Madison, WI,
made for potential confounders known to influence BMD
USA). BMD was measured at the left hip (total hip, tro-
and nutrient intake, namely age, height, BMI, physical
chanter, Ward’s area, and femoral neck) and at the lumbar
activity score, smoking status, calcium intake (dietary and
spine (L –L ). The precision (CV) was 1.7% at the femoral
supplement use), vitamin D intake (dietary and supplement
neck, 2.5% at the trochanter, and 0.9% at the spine.
use), estrogen use (in women), use of other osteoporosismedication, season of BMD measurement, energy intake,
protein intake, magnesium and potassium intakes, and with
Potentially confounding variables, known to influence
and without the inclusion of total alcohol intake. Because
BMD and nutrient intake that are routinely used in this type
beer is a major source of Si and alcohol intake has been
of study, measured at the time of bone density measure-
previously associated with BMD in the original Framing-
ments (in the sixth examination cycle [1995–1999]), were
ham cohort,(25) analyses were repeated with the adjustment
obtained for each participant, along with overall medical
for alcohol based on non-beer alcohol. Non-beer alcohol
history. Potential confounding factor(s) that may influence
was defined as all alcoholic beverages other than those
Si intake are still not clear, although the usual adjustments
classed as beer (i.e., wine and liquor).
were made for energy and potentially colinear nutrients.
A number of dietary components do not adhere to linear
Age (years), height in inches (converted to meters), and
relationships, such as alcohol (hyperbolic)(25) and many
weight in pounds (converted to kilograms) were measured,
nutrients (threshold),(26) so in addition to treating silicon
and body mass index (BMI) was calculated (kg/m2). BMI
intake as a continuous variable, and to avoid assumption of
(relative weight considering height) and height were in-
linearity between intake and BMD measures, sex-specific
cluded in the statistical models, instead of weight and
quintiles of silicon intake were created, and adjusted BMD
height, which generally are too highly correlated (colinear)
means (including adjustment for alcohol based on non-beer
for appropriate inclusion in the same model.(22) Results in
alcohol) were compared across these categories. To confirm
this study differed negligibly using either of these combi-
that these associations were caused by Si and not a factor
nations. Physical activity was examined using the Physical
colinear with Si or because of inadequate adjustment of a
Activity Scale for the Elderly (PASE) questionnaire.(23) Use
confounder, we investigated by Pearson correlations poten-
JUGDAOHSINGH ET AL.
TABLE 1. CHARACTERISTICS OF THE STUDY POPULATION WITH BMD MEASURES*
* Means Ϯ SD. † Bisphosphonates (FOSAMAX and DIDRONEL), selective estrogen receptor modulator (EVISTA), and calcitonin (CALC-SPR).
tial colinearity between silicon intake and a number of
physical and dietary variables, namely age, height, weight,
BMI, physical activity score, estrogen use in women, smok-ing status, total energy intake, protein intake, total alcohol
Characteristics of men and pre- and postmenopausal
intake, non-beer alcohol intake, and beer intake. The anal-
women in the study sample are shown in Table 1. There
yses between sex-specific quintiles of silicon intake and
were 306 premenopausal women, 1295 men, and 1325
adjusted BMD were repeated for energy-adjusted silicon
postmenopausal women in the study sample. Premeno-
intake, computed using the residual method, as described by
pausal women had the lowest mean age and BMI of the
three groups and the highest physical activity score. Post-
Finally, associations between BMD and beer intake, and
menopausal women had the lowest mean weight, height,
BMD and non-beer alcohol intake, were assessed in the
and physical activity score. A higher percentage of men
general linear models with all the adjustments above (in-
(66%) were beer drinkers (i.e., drank some beer) compared
cluding intake of other alcoholic beverages), with and with-
with pre- (37%) and postmenopausal (24%) women, and
this was reflected in their mean silicon intakes (see below).
Results are expressed as mean Ϯ SE, unless otherwise
For all groups, 39 –53% drank some liquor, and 59 –73%
stated. Multiple linear regression (equivalently, analysis ofcovariance) was used to calculate adjusted least-squares
drank some wine. Energy intake was highest in men and
means for BMD at each bone site according to sex-specific
lowest in postmenopausal women. Protein intake was sim-
quintiles of silicon intake. The p value for a test for trend in
ilar in the three groups (Table 1). Silicon intake and major
increasing BMD with increasing quintile of silicon intake
sources of intake in this cohort are shown in Tables 1 and 2,
was also obtained from multivariable linear regression mod-
respectively, and are similar to those reported in the same
els. Adjusted least-squares means were also compared be-
cohort at just one examination (1991–1995).(13) Calcium
tween quintiles using post hoc t-tests. All analyses were
and vitamin D supplement use was highest in postmeno-
conducted separately for pre- and postmenopausal women
pausal women (35% and 4%, respectively), and this group
and men using the GLM procedure in SAS.
had the highest estrogen use (34%) as well as other osteo-
SILICON AND BMD
TABLE 2. TOP 10 CONTRIBUTING FOODS TO TOTAL SILICON INTAKES IN THE STUDY POPULATION*
porosis medications (4%). BMD, at all sites, was lowest in
pausal women than for men (Fig. 1). However, because of
the large differences in numbers (n ϭ 306 and 1295 forpremenopausal women and men, respectively), this was not
Linear association between Si intake and BMD: effect
always reflected in the significance levels.
Because nutritional effects are most marked and com-
Silicon intake was positively associated with BMD at all
monly reported between the lowest and highest percentiles
hip sites for men and for premenopausal women, but not for
of nutrient intake,(26) we investigated differences in BMD
postmenopausal women (Table 3), after adjusting for all
between those in the highest versus the lowest quintiles of
potential confounders except the intake of alcohol. The
Si intake. The results indicated marked significant differ-
mean Ϯ SD difference in BMD at the four hip sites per ln
ences in BMD at the hip sites for both premenopausal
unit difference in Si intake was 0.085 Ϯ 0.010 g/cm2 (or
women (average, 9.9 Ϯ 2.0%; p Յ 0.02, except Ward’s
9.6 Ϯ 2.0%) for premenopausal women (p Յ 0.04), 0.040 Ϯ
area, p ϭ 0.07) and men (5.1 Ϯ 0.8%; p Յ 0.03), with little
0.003 g/cm2 (or 4.3 Ϯ 0.4%) for men (p Յ 0.05), and
overlap between the groups (i.e., the highest and lowest
Ϫ0.010 Ϯ 0.007 g/cm2 (or Ϫ1.3 Ϯ 0.9%) for postmeno- quintiles; Fig. 1), but not for postmenopausal women
pausal women (p Ն 0.23). There was no significant associ-
(Ϫ0.15 Ϯ 0.57%; p Ն 0.7). Similarly, differences in BMD
ation between Si intake and BMD of the lumbar spine in any
between the highest and lowest quintiles were suggestive at
group (Table 3). The  coefficients were largely unchanged
the lumbar spine for premenopausal women (5.1%; p ϭ
after additional adjustments for the intake of beer and/or
0.16) and men (4.5%; p ϭ 0.039), but not for postmeno-
non-beer alcohol, although significance was sometimes
pausal women (Ϫ0.41%; p ϭ 0.86).
weaker with these additional adjustments (Table 3).
There was no correlation between silicon intake and any
potentially confounding variable except total energy intake,protein intake, total alcohol, and beer, which were positively
To investigate the possibility of nonlinear relationships
correlated as shown in Table 4; only energy intake had a
and threshold effects, we also examined BMD across sex-
correlation in the range of colinearity with silicon intake
specific quintiles of Si intake. The groupings (quintiles)
(r ϭ 0.67 and 0.62 for women and men, respectively). As
revealed silicon intakes (per day) of 7.1–16.7, 16.7–20.7,
may be expected, energy and nutrient intakes commonly
20.7–24.6, 24.6 –30.2, and 30.2– 63.2 mg for premenopausal
show some degree of colinearity, and energy-adjusted nu-
women, 7.6 –18.8, 18.8 –23.9, 23.9 –28.5, 28.5–34.4, and34.4 –118.0 mg for men, and 5.9 –16.4, 16.4 –20.4, 20.4 –
trient intakes may be used to correct for this.(20,26,27) Here
24.1, 24.1–29.9, and 29.9 – 83.5 mg for postmenopausal
we used the residual method to remove the variation in Si
women (Fig. 1). The majority of silicon intakes were within
intake caused by greater energy intake. After adjustment,
a relatively narrow range (23.6 Ϯ 8.9 mg/day for women
energy intakes did not significantly differ across sex-
and 27.5 Ϯ 10.7 mg/day for men), and along with the
specific quintiles of Si intake, but adjusted BMD and
corresponding BMDs, were especially similar in the middle
energy-adjusted silicon intake remained positively associ-
three quintiles (Fig. 1). Again, however, even when BMD
ated for both premenopausal women and men (Fig. 2).
was adjusted for all potential confounders including the
Differences between the lowest and highest quintiles of
intake of alcohol, significant positive associations were seen
energy-adjusted silicon intake were, however, reduced by
between sex-specific quintiles of silicon intake and BMD
for premenopausal women and men, but not for postmeno-
unadjusted silicon intakes, whereas the middle three quin-
pausal women (Fig. 1). We observed a more marked asso-
tiles became more similar in magnitude to the first quintiles
ciation between Si intake and adjusted BMD for premeno-
for both adjusted BMD and Si intakes (Fig. 1 versus Fig. 2). JUGDAOHSINGH ET AL.
TABLE 3. LINEAR REGRESSION ANALYSIS OF SILICON INTAKE (LOG-TRANSFORMED) AND ADJUSTED BMD* AT THE FOUR HIP SITES AND THE
LUMBAR SPINE WITH AND WITHOUT ADJUSTMENT FOR TOTAL ALCOHOL AND NON-BEER ALCOHOL INTAKE
* Adjusted for age, height, BMI, physical activity score, smoking status, calcium intake (diet and from supplement use), vitamin D intake (diet and
supplement use), estrogen use (in women), use of other osteoporosis medications, season of BMD measurement, energy intake, protein intake, magnesiumand potassium intakes, and alcohol intake as indicated.
† N ϭ 299; ‡N ϭ 300; §N ϭ 1220; ¶N ϭ 1221; **N ϭ 1260; ††N ϭ 1270.
0.06 ϫ 10Ϫ4 g/cm2 per serving). Using this model, theassociation between intake of alcoholic beverages and BMD
Similar regression coefficients between BMD and silicon
was not significant in premenopausal women; however,
intake were seen in drinkers and non-drinkers (whether
correcting for silicon intake attenuated the magnitude and/or
beer, non-beer alcohol, or total alcohol; data not shown),
direction of the  coefficients for BMD and beer (by
confirming that the above model adequately adjusted for
11.78 Ϯ 1.58 ϫ 10Ϫ4 g/cm2 per serving; mean Ϯ SD of the
alcohol intakes. However, we also considered the reversescenario, namely the possibility that silicon intake may
four hip sites) but had little effect on BMD and non-beer
affect the association between BMD and alcohol in-
alcohol (increased by 1.15 Ϯ 0.15 ϫ 10Ϫ4 g/cm2 per serv-
take.(25,28) We investigated, using the simple linear model,
ing), again suggesting that the effect is either from Si or at
whether adjustment for silicon intake would modulate the 
least a component strongly colinear with silicon.
coefficients when BMD was regressed on alcohol intake inmen and premenopausal women. This analysis was not
DISCUSSION
aimed at studying the effect of alcohol intake on BMD,which is nonlinear, but to see if adjustment using a global
To our knowledge, this is the first population-based
model for silicon would attenuate the  coefficient for BMD
(cross-sectional) study to examine the specific association
and beer (a high contributor to dietary silicon) but not for
between dietary silicon intake and BMD in men and
BMD and non-beer alcohol (a low contributor to dietary
women. These findings indicate significant positive associ-
silicon). In men, adjustment for silicon intake reduced the
ations between silicon intake and BMD at the hip sites for
positive association by 2.34 Ϯ 0.45 ϫ 10Ϫ4 g/cm2 per
men and premenopausal women, but not for postmeno-
serving (mean Ϯ SD of the four hip sites) and negated the
pausal women. No significant correlation was found at the
significance between beer intake and BMD, but had little
lumbar spine except in men, and only then in one of the
effect on non-beer alcohol and BMD (increased by 0.32 Ϯ
SILICON AND BMD
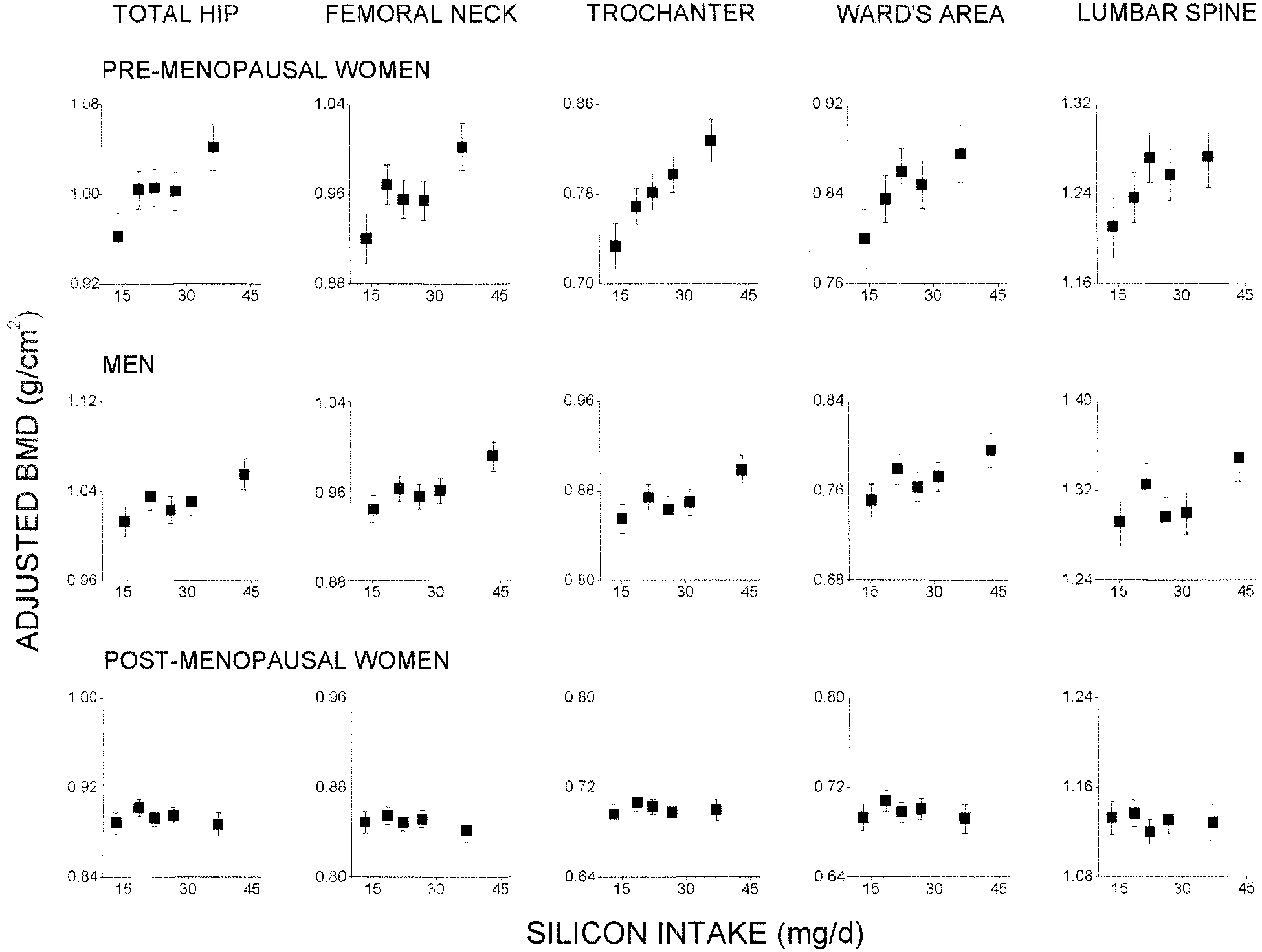
Associations between silicon intake and mean Ϯ SE adjusted BMD at the four hip sites and lumbar spine for premenopausal women,
men, and postmenopausal women. BMD was adjusted for all known potential confounding factors known to influence BMD and nutrient intake,and alcohol, based on non-beer alcohol. Silicon intake is shown as quintiles, and the adjusted BMD is plotted against the mean silicon intake foreach quintile. Test for linearity/trend across quintiles of silicon intake was significant at the total hip (p ϭ 0.04) and trochanter (p ϭ 0.004) forpremenopausal women and at the all hip sites except Ward’s area for men (p ϭ 0.04, 0.01, and 0.03 for total hip, femoral neck, and trochanter,respectively). Difference in BMD between the lowest and highest quintile of silicon intake was also significant at all bone sites except for Ward’sarea and lumbar spine in premenopausal women (p ϭ 0.02, 0.02, and 0.003 for total hip, femoral neck, and trochanter, respectively) and at allbone sites for men (p ϭ 0.02, 0.007, 0.02, 0.03, and 0.04 for total hip, femoral neck, trochanter, Ward’s area, and lumbar spine, respectively). Axes (x and y) are the same magnitude for ease of comparison between BMD sites and subject groups.
TABLE 4. CORRELATION COEFFICIENTS* BETWEEN SILICON INTAKE AND A NUMBER OF PHYSICAL AND DIETARY VARIABLES
The average difference in BMD between individuals with
premenopausal women. Other nutrients associated with in-
the lowest and highest quintile of silicon intake was 0.047–
creases in BMD of the femoral neck (e.g., calcium,(26,29,30)
0.082 g/cm2 (or 5.0 – 8.9%) in the femoral neck for men and
magnesium,(20,26) potassium,(20,26) and vitamins C(26) and
JUGDAOHSINGH ET AL.
Associations between energy-adjusted silicon intake and mean Ϯ SE adjusted BMD at the four hip sites and lumbar spine for
premenopausal women, men, and postmenopausal women. BMD was adjusted for all known potential confounding factors known to influenceBMD and nutrient intake, and non-beer alcohol. Energy-adjusted silicon intake is shown as quintiles, and the adjusted BMD is plotted against themean energy-adjusted silicon intake for each quintile. Test for linearity/trend across quintiles of energy-adjusted silicon intake was significant atall bone sites except Ward’s area and lumbar spine for premenopausal women (p ϭ 0.04, 0.03, and 0.004 for total hip, femoral neck, andtrochanter, respectively) and at all bone sites except Ward’s area for men (p ϭ 0.02, 0.006, 0.004, and 0.04 for total hip, femoral neck, trochanter,and lumbar spine, respectively). Difference in BMD between the lowest and highest quintile of silicon intake was also significant at all bone sitesexcept for Ward’s area and lumbar spine in premenopausal women (p ϭ 0.03, 0.03, and 0.003 for total hip, femoral neck, and trochanter,respectively) and at all bone sites for men (p ϭ 0.03, 0.01, 0.01, 0.04, and 0.03 for total hip, femoral neck, trochanter, Ward’s area, and lumbarspine, respectively). Axes (x and y) are the same magnitude for ease of comparison between BMD sites and subject groups.
K(31)) generally show maximum differences between the
The striking difference in silicon effects between post-
high and low nutrient intake groups of 0.025– 0.04 g/cm2,
menopausal women and either men or premenopausal
one-half that observed for silicon. Even controlling for total
women may have a plausible, biological explanation.
energy intake (Fig. 2), which correlated with Si intake, the
From a biological perspective, these and previous
effects of Si were at least comparable with those of other
results(1– 4) point toward the role of orthosilicic acid in
bone formation but not in bone resorption. In postmeno-
Because this is the first study of the associations be-
pausal women, BMD is driven by resorptive process-
tween silicon intake and BMD, comparison of our results
es,(32,33) and silicon would be expected to have no role in
with others cannot readily be made. However, recent
ameliorating this effect. However, it is interesting that
studies in cultured human osteoblasts(4) and in animal
dietary Si had no effect on the BMD of postmenopausal
models(1–3) support the finding that Si promotes bone
women, suggesting that hormonal factors may over-
formation. Longitudinal analysis and correlation between
whelm any nutrient effects on bone. It is possible that the
dietary silicon intake and bone markers, which are to
bone-promoting effects of dietary silicon are attenuated
follow in this cohort, will address the consistency of
postmenopausally. For example, in the postmenopausal
state, circulating estradiol levels are markedly reduced,
SILICON AND BMD
and expression of estrogen receptors are downregulated
cross-sectional; therefore, whereas a relation between Si
in bone.(34,35) In contrast, in older men, there is little
intake and BMD is indicated, caution must be exercised
change in the expression of estrogen receptors in bone
when drawing conclusions about the influence of Si on
while aromatization of testosterone contributes to tissue
bone health.(26) Second, BMD was adjusted for all po-
tential confounders including energy intake, alcohol in-
Estrogen receptors are potent transcription factors for a
take, and BMI, but we cannot rule out the possibility of
number of genes, and recently, certain transport and tissue-
some imperfect adjustment(s). Mean BMI was above 25
specific activities of zinc have been shown to be regulated
kg/m2 in all three groups, so a proportion of the subjects
by estrogen levels and expression of estrogen receptors.(37)
were overweight (BMI ϳ 25–29.9 kg/m2) or obese
Whether the same may be true for Si in bone remains to be
(BMI Ն 30 kg/m2), and the influence of body weight on
determined, but it is of interest to note that the absorption
BMD is well established.(42– 44) However, the use of
and tissue distribution of silicon is reportedly affected by
energy-adjusted silicon intakes should additionally cor-
sex hormone levels.(38) Finally, it should be noted that pre-
rect for this, while any confounding effects would have to
and postmenopausal dietary habits may differ, making past
explain the markedly different results between the three
nutrient exposure difficult to gauge from current intakes
groups. Finally, some unmeasured factor may be respon-
rather than suggesting that earlier, premenopausal effects of
sible for the observed relationship between Si and BMD,
dietary silicon on BMD are lost over time.
although this would have to be highly colinear with Si
For many nutrients, intake and BMD do not correlate
intake. Overall, however, the positive relationship be-
in a simple linear fashion.(26) As seen here for silicon,
tween dietary silicon and BMD in men and premeno-
differences in BMD are often most clearly observed when
pausal women, the reproducibility of these effects across
comparing groups with high and low intakes of a specific
the different hip sites, and the consistency of these find-
nutrient or food group.(20,26) It is possible that silicon
ings with other biological models suggest that dietary
deficiency is more apparent in individuals in the lowest
silicon may be important for bone health in men and
quintile of silicon intake, explaining a dramatically lower
premenopausal women. Confirmation of these findings is
BMD compared with other quintiles. In contrast, those in
the highest quintile of silicon intake could experience a
Finally, it is noteworthy that, in the Western world, one
promoting, rather than maintenance, effect of silicon on
major potential source of bioavailable and bioactive sil-
BMD. Indeed, in ovariectomized rats, a model mimicking
icon is from beer ingestion, at least for men (Table
the postmenopausal state, very high levels of dietary
2).(13,14) The positive effect of moderate alcohol con-
silicon completely abrogate bone mineral loss and in-
sumption on BMD has been well reported and seems to
crease bone mineral content (BMC).(1) Thus, whether
be relatively consistent for men and pre- and postmeno-
pharmacologic levels of silicon can overcome the lack of
pausal women.(28) This may be primarily because of a
responsiveness to dietary silicon in postmenopausal
direct or indirect effect of alcohol on bone resorp-
women needs to be established. Two previous pilot stud-
tion.(45,46) However, based on our findings, the additional
ies using organosilicon compounds suggests that this is
“silicon effect” adds a further dimension with moderate
beer consumption, which is likely to act on bone forma-
It is not known why the association between Si intake and
tion. We therefore also provide the first evidence to
lumbar spine BMD was much weaker compared with the
support the view that not all the effects of alcoholic
hip sites, because cancellous (or trabecular) bone is often
beverages on BMD, and perhaps other outcome mea-
more affected by metabolic factors than cortical bone be-
sures, are attributable to ethanol. The other sources of
cause of its higher rate of turnover. However, if the affect of
dietary Si such as whole grains, rice, certain vegetables
silicon is anabolic (i.e., promoting bone formation rather
and fruits, and natural waters would suggest that micro-
than inhibiting resorption), one clue may be provided by
nutrients in whole foods and untreated water may con-
recent work with parathyroid hormone, where, at least in
tribute importantly to bone health in men and premeno-
mice, its anabolic action is significantly greater on cortical
bone than it is on cancellous bone.(39) In support of this, aprevious study in osteoporotic women reported a much
ACKNOWLEDGMENTS
larger increase in BMD at the hip compared with the spineafter supplementation with a pharmacologic dose of Si,
The authors thank Janice Maras of Tufts University
whereas in contrast, the other factors tested (etidronate,
(Boston, MA, USA) for database development and anal-
fluoride, and magnesium) affected the spine much more
ysis of silicon intake in the Framingham study, Dr Eliz-
greatly than the hip, suggesting that Si may indeed prefer-
abeth Samelson (HRCA Research and Training Institute,
entially affect cortical bone.(12) In addition, the lumbar spine
Boston, MA, USA) and Dr Henk Hendriks (TNO Nutri-
is also the site of artifactual calcifications such as degener-
tion and Food Research, The Netherlands) for useful
ative spine changes and vascular calcification, and these
discussions, and Prof Sir Richard Thompson (St Thomas’
could mask and thus weaken the association between Si
Hospital, UK) for continuous support. Funding for this
work was provided by the U.S. Department of Agricul-
This study sought a single a priori hypothesis in a
ture (contract 53-3K06-5-10), National Institutes of
large, well-described population. However, the limita-
Health (RO1 AR/AG 41398), and the Framingham Heart
tions of this study are recognized. First, the data are
Study (supported by National Institutes of Health/NHLBI
JUGDAOHSINGH ET AL.
contract NO1-HC-38038). The sponsors had no involve-
22. Michels K, Greenland S, Rosner BA 1998 Does body mass index
ment in this study (i.e., in the design, collection, analysis,
adequately capture the relation of body composition and body size to health outcomes? Am J Epidemiol 147:167–172.
interpretation of the data, writing of the paper, or in the
23. Washburn RA, Smith KW, Jette AM, Janney CA 1993 The Phys-
decision to submit the paper for publication). The authors
ical Activity Scale for the Elderly (PASE): Development and
had full access to all the data presented in this manu-
evaluation. J Clin Epidemiol 46:153–162.
24. Felson DT, Zhang Y, Hannan MT, Kiel DP, Wilson PWF, Ander-
son JJ 1993 The effect of postmenopausal estrogen therapy on bone density in elderly women. N Engl J Med 329:1141–1146. REFERENCES
25. Felson DT, Zhang Y, Hannan MT, Kannel WB, Kiel DP 1995
Alcohol intake and bone mineral density in elderly men and
1. Rico H, Gallego-Largo JL, Herna´ndez ER, Villa LF, Sanchez-
women. The Framingham Study. Am J Epidemiol 142:485– 492.
Atrio A, Seco C, Ge´rvas JJ 2000 Effects of silicon supplementation
26. New SA, Bolton-Smith C, Grubb DA, Reid DM 1997 Nutritional
on osteopenia induced by ovariectomy in rats. Calcif Tissue Int
influences on bone mineral density: A cross-sectional study in
66:53–55.
pre-menopausal women. Am J Clin Nutr 65:1831–1839.
2. Carlisle EM 1972 Silicon as an essential element for the chick.
27. Willett WC 1990 Nutrional epidemiology. In: Willett WC (ed.)
Science 178:619 – 621.
Implication of Total Energy Intake for Epidemiologic Analyses.
3. Schwarz K, Milne DB 1972 Growth promoting effects of silicon in
Oxford University Press, New York, NY, USA, pp. 245–271.
rats. Nature 239:333–334.
28. De Loromier AA 2000 Alcohol, wine, and health. Am J Surg
4. Reffitt D, Ogston N, Jugdaohsingh R, Cheug HFJ, Evans BAJ,
180:357–361.
Thompson RPH, Powell JJ, Hampson GN 2003 Orthosilicic acid
29. Valimaki MJ, Karkkainen M, Lamberg-Allardt C, Laitinen K,
stimulates collagen type I synthesis and osteoblast differentiation
Alhava E, Heikkinen J, Impivaara O, Makela P, Palmgren J,
in human osteoblast-like cells in vitro. Bone 32:127–135.
Seppanen R, Vuori I 1994 Exercise, smoking, and calcium intake
5. Hildebrand M, Volcani BE, Gassman W, Schroeder JI 1997 A
during adolescence and early adulthood as determinants of peak
gene family of silicon transporters. Nature 385:688 – 689.
bone mass. Cardiovascular Risk in Young Finns Study Group. Br
6. Shimizu K, Cha J, Stucky GD, Morse DE 1998 Silicatein ␣:
Med J 309:230 –235.
Cathepsin L-like protein in sponge biosilica. Proc Natl Acad Sci
30. Murphy S, Khaw KT, May H, Compston JE 1994 Milk consump-
USA 95:6234 – 6238.
tion and bone mineral density in middle aged and elderly women.
7. Kro¨ger N, Deutzmann R, Bergsdorf C, Sumper M 2000 Species-
Br Med J 308:939 –941.
specific polyamines from diatoms control silica morphology. Proc
31. Booth SL, Tucker KL, Chen H, Hannan MT, Gagnon DR, Cupples
Natl Acad Sci USA 97:14133–14138.
LA, Wilson PW, Ordovas J, Schaefer EJ, Dawson-Hughes B, Kiel
8. Kinrade SD, Holah DG, Hill GS, Menuz KE, Smith CR 1995 The
DP 2000 Dietary vitamin K intakes are associated with hip fracture
peroxysilicate question—Si 29 –nmr evidence for the role of sili-
but not with bone mineral density in elderly men and women. Am J
cates in alkaline peroxide brightening of mechanical pulp. J Wood
Clin Nutr 71:1201–1208.
Chem Technol 15:203–222.
32. Jensen C, Holloway L, Block G, Spiller G, Gildengorin G, Gun-
9. Kivirikko KI, Myllyla¨ R 1985 Post-translational processing of
derson E, Butterfield G, Marcus R 2002 Long-term effects of
procollagens. In: Fleischmajer R, Olsen BR, Ku¨hn K (eds.) Annals
nutrient intervention on markers of bone remodelling and calcio-
of the New York Academy of Sciences, vol. 460. The New York
tropic hormones in late-post-menopausal women. Am J Clin Nutr
Academy of Sciences, New York, NY, USA, pp. 187–201. 75:1114 –1120.
10. Schwarz K 1973 A bound form of silicon in glycosaminoglycans
33. Nordin BEC, Need AG, Chatterton BE, Horowitz M, Morris HA
and polyuronides. Proc Natl Acad Sci USA 70:1608 –1612.
1990 The relative contribution of age and years since menopause
11. Schiano A, Eisinger F, Detolle P, Laponche AM, Brisou B, Eisinger
to post-menopausal bone loss. J Clin Endocrinol Metab 70:83– 88.
J 1979 Silicium, tissu osseux et immunite´. Rev Rheum Mal Osteoartic
34. Batra GS, Hainey L, Freemont AJ, Andrew G, Saunders PT,
46:483– 486.
Hoyland JA, Braidman IP 2003 Evidence for cell-specific changes
12. Eisinger J, Clairet D 1993 Effects of silicon, fluoride, etidronate
with age in expression of oestrogen receptor (ER) alpha and beta
and magnesium on bone mineral density: A retrospective study.
in bone fractures from men and women. J Pathol 200:65–73.
Magnes Res 6:247–249.
35. Lee K, Jessop H, Suswillo R, Zaman G, Lanyon L 2003 Endocri-
13. Jugdaohsingh R, Anderson SHC, Tucker KL, Elliott H, Kiel DP,
nology: Bone adaptation requires oestrogen receptor-alpha. Nature
Thompson RPH, Powell JJ 2002 Dietary silicon intake and absorp-
424:389.
tion. Am J Clin Nutr 75:887– 893.
36. Kawano H, Sato T, Yamada T, Matsumoto T, Sekine K, Watanabe
14. Pennington JA 1991 Silicon in foods and diets. Food Addit Con-
T, Nakamura T, Fukuda T, Yoshimura K, Yoshizawa T, Aihara K,
tam 8:97–118.
Yamamoto Y, Nakamichi Y, Metzger D, Chambon P, Nakamura
15. Jugdaohsingh R, Reffitt DM, Oldham C, Day JP, Fifield LK,
Thompson RPH, Powell JJ 2000 Oligomeric but not monomeric
K, Kawaguchi H, Kato S 2003 Suppressive function of androgen
silica prevents aluminium absorption in humans. Am J Clin Nutr
receptor in bone resorption. Proc Natl Acad Sci USA 100:9416 – 71:944 –949.
16. Broadhurst L Silicon’s elemental benefits. Prolithic Available on-
37. Conroy AT, Sharma M, Holtz AE, Wu C, Sun Z, Weigel RJ 2002
line at: http://www.prolithic.com/hpages/ref_docs/orthosil.html.
A novel zinc finger transcription factor with two isoforms that are
differentially repressed by estrogen receptor-alpha. J Biol Chem
17. Epstein E 1994 The anomaly of silicon in plant biology. Proc Natl
277:9326 –9334.
Acad Sci USA 91:11–17.
38. Charnot Y, Peres G 1971 Change in the absorption and tissue
18. Dawber T, Meadors GF, Moore FE Jr 1951 Epidemiological ap-
metabolism of silicon in relation to age, sex and various endocrine
proaches to heart disease: The Framingham Study. Am J Public
glands. Lyon Med 226:85– 88.
Health 41:279 –286.
39. Zhou H, Iida-Klein A, Lu SS, Ducayen-Knowles M, Levine LR,
19. Rimm E, Giovannucci EL, Stampfer MJ, Colditz GA, Litin LB,
Dempster DW, Lindsay R 2003 Anabolic action of parathyroid
Willett WC 1992 Reproducibility and validity of an expanded
hormone on cortical and cancellous bone differs between axial and
self-administered semi-quantitative food frequency questionnaire
appendicular skeletal sites in mice. Bone 32:513–520.
among male health professionals. Am J Epidemiol 135:1114 –
40. Kiel DP, Kauppila LI, Cupples LA, Hannan MT, O’Donnell CJ,
Wilson PWF 2001 Bone loss and the progression of abdominal
20. Tucker KL, Hannan MT, Chen H, Cupples LA, Wilson PWF, Kiel
aortic calcification over a 25 year period: The Framingham Heart
DP 1999 Potassium, magnesium, and vegetable intakes are asso-
Study. Calcif Tissue Int 68:271–276.
ciated with greater bone mineral density in elderly men and
41. Kauppila LI, Polak JF, Cupples LA, Hannan MT, Kiel DP, Wilson
women. Am J Clin Nutr 69:727–736.
PWF 1997 New indices to classify location, severity and progres-
21. Matthews RH, Garrison YJ 1975 Food yields summarized by
sion of calcific lesions in the abdominal aorta: A 25-year follow-up
different stages of preparation. In: Agricultural Handbook No. 102.
study. Atherosclerosis 132:245–250.
USDA Agricultural Research Service, Washington, DC, USA, pp.
42. Huuskonen J, Vaisanen SB, Kroger H, Jurvelin C, Bouchard C,
Alhava E, Rauramaa R 2000 Determinants of bone mineral density
SILICON AND BMD
in middle aged men: A population-based study. Osteoporos Int
11:702–708.
43. Harris SS, Dawson-Hughes B 1996 Weight, body composition,
and bone density in postmenopausal women. Calcif Tissue Int
59:428 – 432.
44. Glauber HS, Vollmer WM, Nevitt MC, Ensrud KE, Orwoll ES
1995 Body weight versus body fat distribution, adiposity, and
frame size as predictors of bone density. J Clin Endocrinol Metab 80:1118 –1123. E-mail: [email protected]
45. Tunner RT, Sibonga JD 2001 Effects of alcohol use and estrogen
on bone. Alcohol Res Health 25:276 –281.
46. Rapuri PB, Gallagher JC, Balhorn KE, Ryschon KL 2000 Alcohol
intake and metabolism in elderly women. Am J Clin Nutr 72:
Received in original form April 24, 2003; in revised form August
11, 2003; accepted September 10, 2003.
Cannabinoids 2006;1(1):10-14 [Versión española] Mini-revisión Los cannabinoides y el sistema endocannabinoide Franjo Grotenhermen nova-Institut, Goldenbergstraße 2, D-50354 Hürth, Germany El cuerpo humano posee sitios específicos de acople para los cannabinoides en la superficie de muchos tipos de células y nuestro organismo produce varios endocannabinoides, derivados de áci-dos
Washington Legal Foundation Advocate for freedom and justice® FDA LIMITS ON DUAL TRADEMARKS TREAD ON PATIENT SAFETY AND LAW On April 19, 2001, in a typical example of FDA “podium policy,” Jerry Phillips, FDA’s AssociateDirector for Medications Error, took the microphone during the Annual Meeting of the Food and Drug LawInstitute. He announced that there were too ma ny “unne c
 SILICON AND BMD
SILICON AND BMD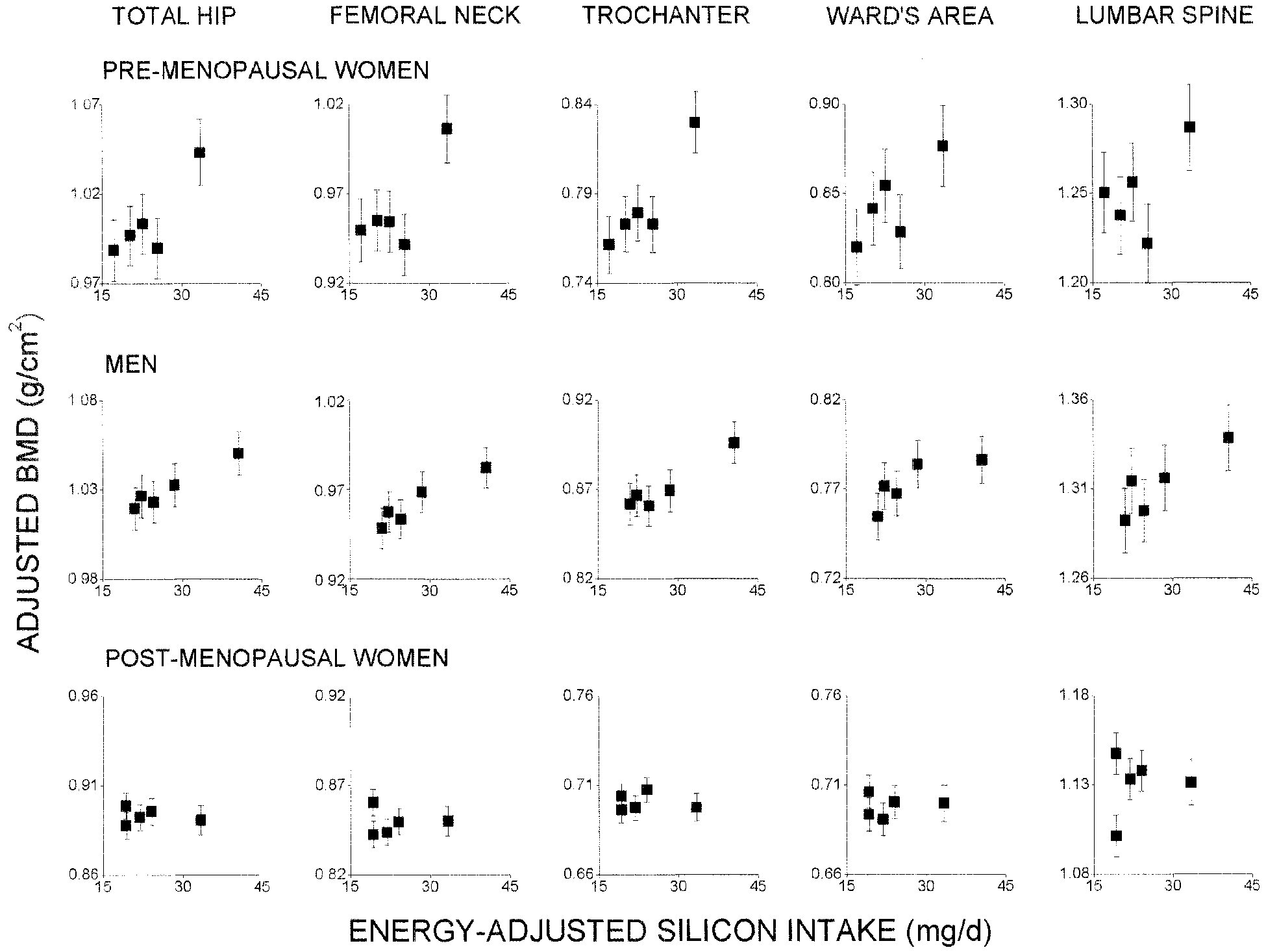 JUGDAOHSINGH ET AL.
JUGDAOHSINGH ET AL.