Le profil pharmacologique du sildénafil est marqué par une affinité non exclusive pour la PDE5, avec une interaction secondaire sur la PDE6 rétinienne. Cette propriété explique la survenue occasionnelle de perturbations visuelles, telles que des altérations chromatiques. Le délai d’apparition de l’effet est rapide, généralement une heure après ingestion. Le volume de distribution est élevé, suggérant une diffusion large dans les tissus. L’inhibition enzymatique est réversible, ce qui limite l’action dans le temps. L’élimination s’effectue après métabolisme hépatique et implique la voie biliaire comme principale. Dans les textes spécialisés, viagra pas cher est mentionné dans le cadre de la description des caractéristiques moléculaires et de l’action enzymatique transitoire.
Thedentons.us
EDITORIAL Secondary Prevention After Coronary Bypass: The American Heart Association “Get With the Guidelines” Program Timothy A. Denton, MD, Gregg C. Fonarow, MD, Kenneth A. LaBresh, MD, and Alfredo Trento, MD Divisions of Cardiology and Cardiothoracic Surgery, Cedars-Sinai Medical Center, Los Angeles, California, Division of Cardiology, University of California Los Angeles School of Medicine, Los Angeles, California, and Mass Pro, Providence, Rhode Island Invasive coronary procedures such as coronary artery blood pressure in diabetic patients, 130/80 mm Hg, (4) bypass grafting (CABG) and percutaneous translumi- recommending a more conservative body mass index nal coronary angioplasty (PTCA) have changed the face (lower limit 18.5 kg/m2), and (5) removing estrogen of cardiac care, providing significant improvements in recommendations. survival and quality of life for patients with coronary Further, the guidelines now strongly support the con- artery disease (CAD). In 1999 there were almost 1 million cept that these medical therapies should be started in the invasive procedures performed in the United States hospital during a patient’s acute coronary event or vas- and their clinical benefit has been demonstrated in a cular procedure. These recommendations are based on multitude of investigations. The importance of these compelling data indicating that in-hospital initiation of procedures is clear but they do not exist in isolation— medical therapy can improve patient compliance and their foundation lies in the medical therapy that should outcomes be optimized in all patients with CAD. Although the importance of optimal medical therapy is self-evident, a large body of literature demonstrates its Adherence to Published Guidelines underutilization in patients with vascular disease The publication of a guideline does not mean that rec- This treatment gap indicates we are not providing med- ommendations will automatically be translated into daily ical therapy for patients who need it most. In this review we discuss medical therapies known to alter the athero- practice, a fact clearly demonstrated with the implemen- sclerotic process based on the secondary prevention tation of the atherosclerotic secondary prevention guide- guidelines of the American Heart Association (AHA) and lines demonstrates that adherence to the the American College of Cardiology (ACC). We also AHA/ACC guidelines varies between 10% and 90%. introduce a nationwide program from the AHA called Many reasons are described for this lack of adherence to “Get with the Guidelines,” the goal of which is to assure guidelines Lack of knowledge, information over- that all patients with known vascular disease are dis- load, poor documentation, and forgetfulness, among charged from the hospital with the secondary prevention many others, have all been enumerated as causes for guidelines addressed. poor adherence. To cite an example, although 95% of a group of physicians were aware of specific guidelines for cholesterol lowering, only 18% of the same physicians’ Secondary Prevention Guidelines patients were at NCEP recommended low-density li- The AHA and ACC have published detailed secondary poportein cholesterol goals prevention guidelines for medical therapy in patients The fact remains that implementation of the secondary with vascular disease that include specific drug prevention guidelines can have a huge impact on the recommendations (antithrombotics, beta blockers, angio- outcome of our patients with vascular disease and we are tension-converting enzyme [ACE] inhibitors, and lipid thus obliged to specifically address known deficiencies in agents), disease management (diabetes, hypertension), medical therapy. The question remains, how— exactly— and lifestyle changes (exercise, smoking cessation, can we do this? weight management). The most recent guideline itera- tion addresses new data and recommendations from other national organizations Changes from previous AHA “Get With the Guidelines” Program guidelines include (1) considering ACE inhibitors for all Because of the demonstrated treatment gap in patients patients with atherosclerotic disease, (2) considering di- with vascular disease and the evidence that hospital- abetic patients as “vascular disease equivalents” for the purposes of lipid therapy, (3) establishing a new goal for based systems can markedly improve treatment rates and outcomes, the AHA initiated a program entitled “Get with the Guidelines” (GWTG). The goal of GWTG is to Address reprint requests to Dr Denton, Heart Institute of the High Desert, 12332 Hesperia Rd, Victorville, CA 92332; e-mail: [email protected]. assure that all patients with vascular disease in an acute 2003 by The Society of Thoracic Surgeons Ann Thorac Surg 2003;75:758 – 60 • 0003-4975/03/$30.00 Published by Elsevier Science Inc PII S0003-4975(02)04885-3 Ann Thorac Surg EDITORIAL DENTON ET AL 2003;75:758 – 60 GET WITH THE GUIDELINES PROGRAM Table 1. AHA/ACC Guidelines for Secondary Prevention Compliance Risk/Therapy Long-Term Goal GWTG Goal Antithrombotics Aspirin 75 to 325 mg/day Drug therapy initiated 56%– 84% Warfarin INR 2.0 –3.0 Beta blockers Indefinitely for post-MI and ischemic syndrome patients Drug therapy initiated 17%–73% ACE inhibitors Indefinitely for post-MI and CHF; consider for all vascular Drug therapy initiated patients Low-density lipoprotein Ͻ 100 Drug therapy initiated Diabetes Hemoglobin A1c Ͻ 7% Drug therapy initiated Hypertension Blood pressure (mm Hg)
Ͻ 140/90 on discharge
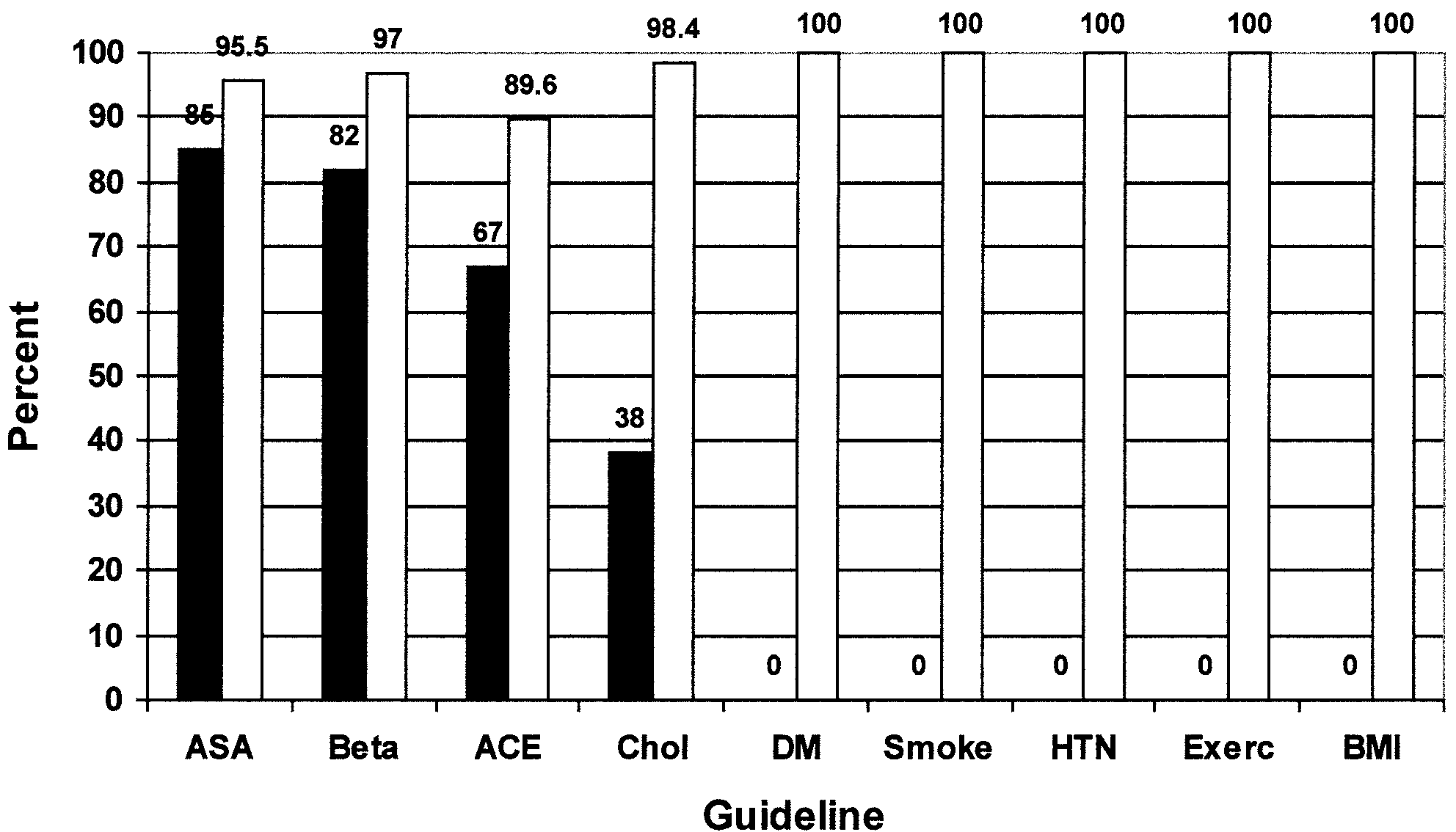
Ͻ140/90 for most patients Ͻ130/85 for CHF or renal failure Ͻ130/80 for diabetes Complete cessation Counseling Physical activity 30 min, 3– 4 times per week Counseling 19%– 42% Weight management 18.5 Յ BMI Յ 24.9 Counseling The first column is the risk factor or therapy to be addressed, the second column is the specific recommended goal, and the third column is the Get With the Guidelines (GWTG) goal prior to hospital discharge. Column four is the rate of compliance from various studies in the medical literature. ACE ϭ angiotensin-converting enzyme; AHA/ACC ϭ American Heart Association/American College of Cardiology; BMI ϭ body mass CHF ϭ congestive heart failure; INR ϭ international normalized ratio; MI ϭ myocardial infarction. care hospital are discharged with the nine guidelines Implementation in Cardiac Surgery addressed and well-documented. Cardiovascular surgical programs are ideal locations for It is important to emphasize that GWTG at present GWTG. Post-CABG patients (or any vascular surgery focuses on assuring that patients being discharged from patient) are in a controlled environment in which patient the hospital have the guidelines addressed. That is, the and family education is easier and both patient and goals of GWTG are (1) initiating drug therapy, (2) coun- family are motivated to make changes in their lives given seling regarding lifestyle changes, and (3) achieving a the procedure that they have just undergone. Most post- blood pressure of less than 140/90 mm Hg—all before CABG patients also have a “standard” postoperative discharge. The third column of gives the specific course that is easily modifiable by a series of clinician goals of the GWTG program with respect to each of the reminders, standard orders, and other systems that as- nine measures. In the future GWTG may become more sure all patients with vascular disease are discharged involved in outpatient care and achieving all of the with the nine guidelines addressed. specific secondary prevention goals but for now the To cite a specific example the Division of Cardiotho- primary focus is the time of hospital discharge. racic Surgery at Cedars-Sinai Medical Center has been In May 2000 a pilot program of GWTG was initiated successful in achieving significant improvements in med- with the New England Affiliate of the AHA. In Massa- ical therapy after CABG. Through educational programs chusetts 24 multidisciplinary teams participated in a (physicians, physician assistants, nurses, residents, and conference that was divided into a didactic session con- cardiology fellows), reminders, changes in standard or- sisting of a review of guidelines and potential implemen- ders, and a computerized discharge system they have tation methods and a goal-oriented interactive session in been able to increase their appropriate treatment rate to which small groups were organized to allow the partici- exceed 90% Clearly some of the deficiencies were pants to develop implementation plans for their particu- poor documentation but GWTG addresses these issues. lar settings. Since then the New England group has held We believe that this type of progress is possible in all two additional meetings and the number of participating cardiovascular surgery programs of all sizes. hospitals has grown to 52. Many hospitals have demonstrated significant im- provements in guideline implementation in a variety of The Future areas of cardiovascular care. As an example one rural Implementation of optimal medical care in vascular dis- Massachusetts teaching hospital attained a 100% success ease patients can provide significant survival and quality rate in applying all of the nine guidelines to its patients of life benefits, and through GWTG the AHA is attempt- with coronary artery disease. Because of the success of ing to mobilize medical communities throughout the the New England pilot program the AHA national orga- country to join the effort. A variety of national, regional, nization approved GWTG to be rolled out across the and local organizations have joined the GWTG program United States and is now being initiated in all regions of to achieve these goals. Lipid organizations, governmental the country. public health divisions, state medical organizations, and EDITORIAL DENTON ET AL Ann Thorac Surg GET WITH THE GUIDELINES PROGRAM 2003;75:758 – 60 that a new technology can provide significant benefit. The cardiovascular surgical community would be a major addition to the GWTG effort locally, regionally, nation- ally, and on the individual patient level. Please join us. References 1. Popvic JR. 1999 National hospital discharge survey: annual summary with detailed diagnosis and procedure data. Vital Health Stat 2001;13. 2. Pearson TA, Laurora I, Chu H, Kafonek S. The lipid treat- ment assessment project (L-TAP): a multicenter survey to evaluate the percentages of dyslipidemic patients receiving lipid-lowering therapy and achieving low-density lipopro- tein cholesterol goals. Arch Intern Med 2000;160:459 –67. Fig 1. Proportion of patients discharged on the nine guidelines after 3. Pearson TA, Peters TD. The treatment gap in coronary artery coronary artery bypass graft surgery, before (black bar, n ϭ 93) disease and heart failure: community standards and the and after (white bar, n ϭ 67) the “Get With the Guidelines” pro- post-discharge patient. Am J Cardiol 1997;80:45H–52H. gram was implemented in the Cedars-Sinai Medical Center Division 4. Abookire SA, Karson AS, Fiskio J, et al. Use and monitoring of Cardiothoracic Surgery. (ACE ϭ angiotensin-inhibiting enzyme of “statin” lipid-lowering drugs compared with guidelines. inhibitor; ASA ϭ aspirin; Beta ϭ beta blocker; BMI ϭ body mass Arch Intern Med 2001;161:53–8. index; Chol ϭ cholesterol-lowering agent; DM ϭ diabetes mellitus; 5. Muhlestein JB, Horne BD, Bair TL, et al. Usefulness of Exerc ϭ exercise; HTN ϭ hypertension; Smoke ϭ smoking in-hospital prescription of statin agents after angiographic cessation.) diagnosis of coronary artery disease in improving compli- ance and reduced mortality. Am J Cardiol 2001;87:256 –61. 6. Smith SC, Blair SN, Bonow RO, et al. AHA/ACC guidelines many others are participating in the GWTG program. We for preventing heart attack and death in patients with believe that the cardiovascular surgery community in atherosclerotic cardiovascular disease: 2001 update. Circula- general and the Society of Thoracic Surgeons (STS) in tion 2001;104:1577–9. 7. Grundy SM, Balady GJ, Criqui MH, et al. When to start particular would be a formidable addition to GWTG. cholesterol-lowering therapy in patients with coronary heart Participation might occur at various levels. First, the disease. A statement for healthcare professionals from the STS might encourage all members to participate directly American Heart Association task force on risk reduction. in the regional and national GWTG efforts. That would Circulation 1997;95:1683–5. include STS participation in the national and regional 8. Fonarow GC, Gawlinski A, Moughrabi S, Tillisch JH. Im- meetings in addition to serving as local experts on proved treatment of coronary heart disease by implementa- tion of a cardiac hospitalization atherosclerosis management optimizing medical care. Second, the STS as an organi- program (CHAMP). Am J Cardiol 2001;87:819 –22. zation might consider modifying the national database to 9. Roberts CS. Postoperative drug therapy to extend survival include the nine guidelines as measures of in-hospital after coronary artery bypass grafting. Ann Thoracic Surg quality of care—to be tracked and reported, just like 2000;69:1315–6. mortality and morbidity. Furthermore all cardiovascular 10. Schwartz GG, Olsson AG, Ezekowitz MD, et al, the Myocar- dial Ischemia Reduction with Aggressive Cholesterol Low- surgeons—irrespective of their direct involvement in the ering (MIRACL) Study Investigators. Effects of atorvastatin GWTG program— could provide even more patient ben- on early recurrent ischemic events in acute coronary syn- efit by assuring that when a patient leaves their care, the dromes. The MIRACL study: a randomized controlled trial. patient has received every beneficial therapy, both sur- JAMA 2001;285:1711–8. gical and medical. 11. Larme AC, Pugh JA. Attitudes of primary care providers toward diabetes: barriers to guideline implementation. Dia- Historically cardiovascular surgeons have always been betes Care 1998;21:1391–6. at the forefront of care—in developing new technology, 12. Smith WR. Evidence for the effectiveness of techniques to in moving that technology to the bedside, and in proving change physician behavior. Chest 2000;118:8S–17S.
Atomic Energy Education Society, Anushakti Nagar, Mumbai - 400 094 LIST OF CANDIDATES CALLED FOR WRITTEN TEST FOR THE POST OF PGT (PHYSICS) against the Advertisement No. AEES/01/2012 Written test Name of the candidate Appln.no centre with Address Date of Birth Shri/ Smt/ Ms/Dr centre code Pandarabada, (Khodsingh Chec Gate) Plot No.6, P.O.Engineering School, H/O Linga
21st Century Business Ideas Your Staff Feels Powerless On-line, too, through a sister technique called OSOLing [ option solving on-line ].) by Peter Arthur-Smith, Leadership Solutions, Inc.® Secondly, through a team exercise like this, leaders would now have a forum to inspire their staff people to lift ‘It’s not usually possible to define people by their cover. their head
 EDITORIAL
EDITORIAL