Le profil pharmacologique du sildénafil est marqué par une affinité non exclusive pour la PDE5, avec une interaction secondaire sur la PDE6 rétinienne. Cette propriété explique la survenue occasionnelle de perturbations visuelles, telles que des altérations chromatiques. Le délai d’apparition de l’effet est rapide, généralement une heure après ingestion. Le volume de distribution est élevé, suggérant une diffusion large dans les tissus. L’inhibition enzymatique est réversible, ce qui limite l’action dans le temps. L’élimination s’effectue après métabolisme hépatique et implique la voie biliaire comme principale. Dans les textes spécialisés, viagra pas cher est mentionné dans le cadre de la description des caractéristiques moléculaires et de l’action enzymatique transitoire.
Gallstones.pm7
National Digestive Diseases Information Clearinghouse
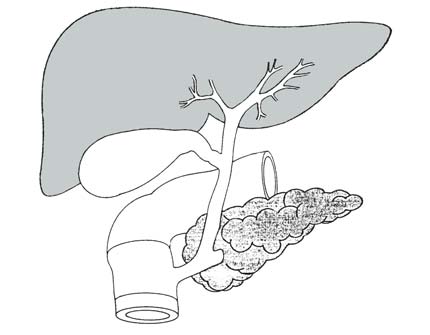
Gallstones form when liquid stored in thegallbladder hardens into pieces of stone-
like material. The liquid, called bile, is
National
used to help the body digest fats. Bile is
Institute of
made in the liver, then stored in the gall-
Diabetes and Digestive
bladder until the body needs to digest fat. and Kidney
At that time, the gallbladder contracts and
Diseases
pushes the bile into a tube—called a duct—
NATIONAL
that carries it to the small intestine, where
INSTITUTES OF HEALTH
Bile contains water, cholesterol, fats, bilesalts, and bilirubin. Bile salts break up fat,
and bilirubin gives bile and stool a brown-
ish color. If the liquid bile contains toomuch cholesterol, bile salts, or bilirubin, itcan harden into stones.
the cystic and hepatic ducts to the small
The two types of gallstones are cholesterol
intestine. Bile trapped in these ducts can
cause inflammation in the gallbladder, the
ducts, or, rarely, the liver. Other ducts open
made primarily of hardened cholesterol.
gallstones. Pigment stones are small, dark
enzymes out of the pancreas. If a gallstone
stones made of bilirubin. Gallstones can be
blocks the opening to that duct, digestive
as small as a grain of sand or as large as a
golf ball. The gallbladder can develop just
creas and cause an extremely painful inflam-
one large stone, hundreds of tiny stones,
Gallstones can block the normal flow of bileif they lodge in any of the ducts that carry
bile from the liver to the small intestine.
That includes the hepatic ducts, which carry
bile out of the liver; the cystic duct, which
takes bile to and from the gallbladder; and
the common bile duct, which takes bile from
If any of these ducts remain blocked for a
or birth control pills appears to increase
significant period of time, severe—possibly
signs of a serious problem are fever, jaun-
• Ethnicity. Native Americans have a
genetic predisposition to secrete highlevels of cholesterol in bile. In fact, they
What Causes Gallstones?
have the highest rates of gallstones inthe United States. A majority of Native
Cholesterol Stones
Scientists believe cholesterol stones form
too much bilirubin, or not enough bile salts,
or when the gallbladder does not empty as
Pigment Stones
• Gender. Women between 20 and
The cause of pigment stones is uncertain.
They tend to develop in people who havecirrhosis, biliary tract infections, and heredi-
• Age. People over age 60 are more likely
tary blood disorders such as sickle cell anemia.
to develop gallstones than youngerpeople. Other Factors
• Cholesterol-lowering drugs. Drugs that
lower cholesterol levels in blood actually
contribute to gallstones have been identi-
fied, especially for cholesterol stones.
• Diabetes. People with diabetes gener-
ally have high levels of fatty acids called
• Obesity. Obesity is a major risk factor
triglycerides. These fatty acids increase
large clinical study showed that beingeven moderately overweight increases
• Rapid weight loss. As the body metabo-
one’s risk for developing gallstones. The
lizes fat during rapid weight loss, it causes
the liver to secrete extra cholesterol into
to reduce the amount of bile salts in bile,
• Fasting. Fasting decreases gallbladder
also decreases gallbladder emptying.
• Estrogen. Excess estrogen from preg- What Are the Symptoms? Symptoms of gallstones are often called a Who Is at Risk for
gallstone “attack” because they occur sud-
Gallstones?
• Steady, severe pain in the upper abdo-
men that increases rapidly and lastsfrom 30 minutes to several hours.
• Pain in the back between the shoulder
Gallstone attacks often follow fatty meals,
and they may occur during the night. Other
• Recurring intolerance of fatty foods. How Are Gallstones Diagnosed?
Many gallstones, especially silent stones, are
discovered by accident during tests for otherproblems. But when gallstones are sus-
doctor is likely to do an ultrasound exam.
Ultrasound uses sound waves to createimages of organs. Sound waves are sent
toward the gallbladder through a handheld
abdomen. The sound waves bounce off thegallbladder, liver, and other organs, and
• Yellowish color of the skin or whites
their echoes make electrical impulses that
monitor. If stones are present, the soundwaves will bounce off them, too, showing
Many people with gallstones have no symp-
toms. These patients are said to be asymp-tomatic, and these stones are called “silentstones.” They do not interfere in gallblad-der, liver, or pancreas function and do notneed treatment.
The standard surgery is called laparoscopiccholecystectomy. For this operation, the sur-
• Cholecystogram or cholescintigraphy.
geon makes several tiny incisions in the abdo-
men and inserts surgical instruments and a
miniature video camera into the abdomen. The
camera sends a magnified image from inside the
body to a video monitor, giving the surgeon a
closeup view of the organs and tissues. While
watching the monitor, the surgeon uses the
instruments to carefully separate the gallbladder
• Endoscopic retrograde
from the liver, ducts, and other structures. Then
cholangiopancreatography (ERCP).
the cystic duct is cut and the gallbladder re-
moved through one of the small incisions.
scope—a long, flexible, lighted tubeconnected to a computer and TV
Because the abdominal muscles are not cut
during laparoscopic surgery, patients have less
pain and fewer complications than they would
have had after surgery using a large incision
volves only one night in the hospital, followed
by several days of restricted activity at home.
If the surgeon discovers any obstacles to the
• Blood tests. Blood tests may be used
laparoscopic procedure, such as infection or
scarring from other operations, the operating
team may have to switch to open surgery. In
some cases the obstacles are known before
surgery, and an open surgery is planned. It is
called “open” surgery because the surgeon has
to make a 5- to 8-inch incision in the abdomen
to remove the gallbladder. This is a majorsurgery and may require about a 2- to 7-daystay in the hospital and several more weeks at
What Is the Treatment?
home to recover. Open surgery is required inabout 5 percent of gallbladder operations. Surgery Surgery to remove the gallbladder is the
The most common complication in gallbladder
surgery is injury to the bile ducts. An injured
common bile duct can leak bile and cause a
painful and potentially dangerous infection.
gallbladder surgery. The surgery is called
nonsurgically. Major injury, however, is more
serious and requires additional surgery. Nonsurgical Treatment Nonsurgical approaches are used only in Don’t People Need Their
special situations—such as when a patient’s
Gallbladders?
condition prevents using an anesthetic—and
only for cholesterol stones. Stones recur
after nonsurgical treatment about half the
won’t even require a change in diet.
Once the gallbladder is removed, bileflows out of the liver through the hepatic
• Oral dissolution therapy. Drugs made
stored in the gallbladder, it flows into the
• Contact dissolution therapy. This
experimental procedure involvesinjecting a drug directly into the gall-
If gallstones are in the bile ducts, the sur-
before or during the gallbladder surgery.
stones in 1 to 3 days, but it must be used
Once the endoscope is in the small intestine,
the surgeon locates the affected bile duct.
An instrument on the endoscope is used to
cut the duct, and the stone is captured in a
tiny basket and removed with the endoscope.
This two-step procedure is called ERCP with
• Extracorporeal shockwave lithotripsy (ESWL). This treatment uses shock waves to break up stones into tiny
Occasionally, a person who has had a chole-
cystectomy is diagnosed with a gallstone in
the bile ducts weeks, months, or even years
tacks of biliary colic (intense pain) are
procedure is usually successful in removing
ing stones can sometimes be dissolvedwith medication. National Digestive Diseases Points To Remember Information Clearinghouse
The National Digestive Diseases Information
Clearinghouse (NDDIC) is a service of the
National Institute of Diabetes and Digestive
part of the National Institutes of Health
Human Services. Established in 1980, theclearinghouse provides information about
digestive diseases to people with digestive
disorders and to their families, health care
swers inquiries; develops, reviews, and distrib-
utes publications; and works closely with
professional and patient organizations andGovernment agencies to coordinate resourcesabout digestive diseases.
Publications produced by the clearinghouseare carefully reviewed for scientific accuracy,content, and readability.
This publication is not copyrighted. The clearinghouse encourages users ofthis fact sheet to duplicate anddistribute as many copies as desired.
This publication is also available at<http://www.niddk.nih.gov/health/digest/digest.htm>.
U.S. DEPARTMENT OF HEALTHAND HUMAN SERVICESNational Institutes of Health
NIH Publication No. 99–2897January 1999
PREFEITURA MUNICIPAL DE SILVEIRÂNIA/MG CONSELHO MUNICIPAL DOS DIREITOS DA CRIANÇA E DO ADOLESCENTE LEI MUNICIPAL Nº675 de 17 de junho de 2013 E SUAS ALTERAÇÕES Edital 01/2013 - CONVOCAÇÃO PARA AS ELEIÇÕES PARA CONSELHEIROS TUTELARES - MANDATO 2014/2017 O Conselho Municipal dos Direitos da Criança e do Adolescente de SILVEIRÂNIA - Minas Gerais, no uso de sua comp
Supported by the European Union FP7 Health - Research Grant number HEALTH-F4-2008-202047 Work Package 2 - Clinical Studies in Humans Work package 2.5 - Fibroproliferative wound healing in the lung Pilot trial: Evaluation of molecular pathology of UIP and idiopathic fibrosing NSIP by combination of clinical and molecular assessment Protocol number: 1. Background The term idiopathic inte
 National Digestive Diseases Information Clearinghouse
National Digestive Diseases Information Clearinghouse National Digestive Diseases
National Digestive Diseases