Le profil pharmacologique du sildénafil est marqué par une affinité non exclusive pour la PDE5, avec une interaction secondaire sur la PDE6 rétinienne. Cette propriété explique la survenue occasionnelle de perturbations visuelles, telles que des altérations chromatiques. Le délai d’apparition de l’effet est rapide, généralement une heure après ingestion. Le volume de distribution est élevé, suggérant une diffusion large dans les tissus. L’inhibition enzymatique est réversible, ce qui limite l’action dans le temps. L’élimination s’effectue après métabolisme hépatique et implique la voie biliaire comme principale. Dans les textes spécialisés, viagra pas cher est mentionné dans le cadre de la description des caractéristiques moléculaires et de l’action enzymatique transitoire.
Microsoft word - patient intake form2.doc
6410 Rockledge Drive, Suite 110, Bethesda, MD, 20817 (O) 301.530.7303 (F) 301.530.7312 2112 F Street, NW, Suite 802A, Washington, DC, 20037 (O) 202.775.7246 (F) 202.775.2345 NAME: ____________________________________________ DATE: ____________
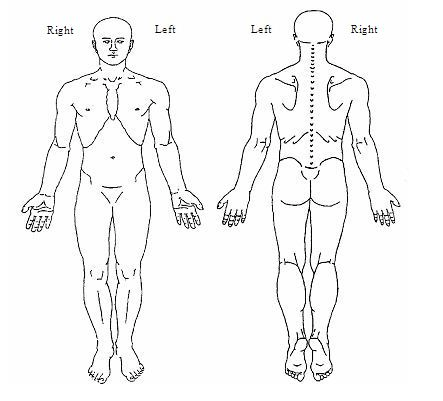
Home Phone: ____________________ Work Phone: _______________________ Cell Phone: ______________________ Who to call in case of emergency: ___________ Name of the doctor who has referred you: _____________________________________ Names of doctors who should get this report: ___________________________________ REASON FOR VISIT: ___________________________________________________ The worst area(s) of pain: __________________________________________________ Please mark the areas of pain Please rate your average daily pain: from 0 (no pain) to 10 (worst possible pain): /10 Length of time that you have had this pain in this area: ________________________ Has something or an event started your pain? YES NO If so what event? ________________________________________________________________________ Circle factors that aggravate your pain? None Standing Exercising Walking Bending Straining Lifting Stress Weather changes Medications Repetitive motions Sitting Head movement Mood swings Light touch Deep breathing Coughing Bearing down Lying down Rolling in bed Other ______________________________________ Circle factors that help your pain: Nothing Resting Walking Standing Sitting Moving Physical therapy Massage Heat/Ice packs Medication Lying down Changing Positions Other__________________________________________________ Circle all characteristics of your pain: Constant Intermittent Burning Sharp Shooting Aching Throbbing Tingling Numbness Other _________________________ Circle prior treatments: Anti-inflammatory medications: (example Ibuprofen), Celebrex, Medrol dose pack Narcotics: Ultram (tramadol), Percocet, Oxycodone, Oxycontin, Vicoden, Hydrocodone, Morphine, Methadone, Dilaudid, Hydromorphone, Duragesic, Actiq Antidepressants: Elavil (Amitriptylline), Pamelor (nortriptylline), Trazodone, Desipramine, Cymbalta Antiseizure medication: Neurontin, Trileptal, Topamax, Gabitril, Lyrica Acupuncture, Magnets, Massage, Chiropractic manipulation, Herbs, Physical therapy Nerve Blocks , Epidural injections, Facet blocks , other ___________________________ ALLERGIES: __________________________________________________________ ALL CURRENT MEDICATIONS YOU ARE TAKING: ______________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ PAST AND PRESENT MEDICAL ISSUES/DISEASES: ______________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ PAST SURGERIES: _____________________________________________________ ________________________________________________________________________ ________________________________________________________________________
FAMILY HISTORY:
SOCIAL HISTORY: Circle all that applies to you. Single Married Divorced Separated Widowed Partnered Do you have children? Yes No How many? ___________________________________ Do you work? Yes No If so, describe please_________________________________ Do you Smoke? Yes No How much? _______________________________________ Do you drink? Yes No How much? _______________________________________ Do you use illicit drugs? Yes No How much? _______________________________ Have you ever been addicted to nicotine, alcohol, or illicit drugs? If so, Please explain ________________________________________________________________________ Are you involved in any unsettled legal issues involving your symptoms? Yes No If so, please explain: ________________________________________________________________________ ________________________________________________________________________ GENERAL HEATH QUESTIONS: Have you had any of the following in the past 2 weeks? (Circle all that applies to you) Fevers Chills Night sweat Unexplained weight loss Eye problems Ear problems Heart problems Lung problems Stomach problems Bladder /kidney problems Skin problems Neurological problems Psychological issues Thyroid problems Diabetes Bleeding problems Please explain any of the above: ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________
CURRICULUM VITAE CARLOS A. DUJOVNE, M.D. Internist,Basic & Clinical Pharmacologist,Clinical Lipidologist, Clinical trials’Investigator Phases I-IV, R&D of drugs-nutraceuticals for prevention and treatment of Cardio-metabolic risks. 1920 SW River Drive, Portland, Oregon 97201 APPOINTMENTS, ACADEMIC TRAINING AND EDUCATION 1998- PresentChairman and Medical Director, Kansas Fou
ED I T O R I A LS “Those who cannot remember the past are condemnedhence Viagra and Zyprexa), was launched in 2001 to the samehype and with even more sophisticated marketing tech“Scepticism is the chastity of the intellect, and it isBy late 2005, it had recorded sales of $214.6 mspitethe release of a negative second studynd about $100 million despite growing concerns about its efficacy

 6410 Rockledge Drive, Suite 110, Bethesda, MD, 20817 (O) 301.530.7303 (F) 301.530.7312
6410 Rockledge Drive, Suite 110, Bethesda, MD, 20817 (O) 301.530.7303 (F) 301.530.7312