Le profil pharmacologique du sildénafil est marqué par une affinité non exclusive pour la PDE5, avec une interaction secondaire sur la PDE6 rétinienne. Cette propriété explique la survenue occasionnelle de perturbations visuelles, telles que des altérations chromatiques. Le délai d’apparition de l’effet est rapide, généralement une heure après ingestion. Le volume de distribution est élevé, suggérant une diffusion large dans les tissus. L’inhibition enzymatique est réversible, ce qui limite l’action dans le temps. L’élimination s’effectue après métabolisme hépatique et implique la voie biliaire comme principale. Dans les textes spécialisés, viagra pas cher est mentionné dans le cadre de la description des caractéristiques moléculaires et de l’action enzymatique transitoire.
Sitemaker.umich.edu
D o u b l e - B l i n d , R a n d o m i z e d T r i a l C o m p a r i n g t h e E f fi c a c y a n d T o l e r a b i l i t y o f F u l v e s t r a n t V e r s u s A n a s t r o z o l e i n P o s t m e n o p a u s a l W o m e n W i t h A d v a n c e d B r e a s t C a n c e r P r o g r e s s i n g o n P r i o r E n d o c r i n e T h e r a p y : R e s u l t s o f a N o r t h A m e r i c a n T r i a l
By C.K. Osborne, J. Pippen, S.E. Jones, L.M. Parker, M. Ellis, S. Come, S.Z. Gertler, J.T. May, G. Burton, I. Dimery,
A. Webster, C. Morris, R. Elledge, and A. Buzdar
Purpose: To compare the efficacy and tolerability of sponse ؉ partial response ؉ stable disease > 24 weeks) fulvestrant (formerly ICI 182,780) with anastrozole in the were 42.2% for fulvestrant and 36.1% for anastrozole treatment of advanced breast cancer in patients whose (95% CI, ؊4.00% to 16.41%; P ؍ .26). In responding disease progresses on prior endocrine treatment. patients, median DOR (from randomization to progres- Patients and Methods: In this double-blind, double- sion) was 19.0 months for fulvestrant and 10.8 months dummy, parallel-group study, postmenopausal pa- for anastrozole. Using all patients, DOR was signifi- tients were randomized to receive either an intramus- cantly greater for fulvestrant compared with anastro- cular injection of fulvestrant 250 mg once monthly or a zole; the ratio of average response durations was 1.35 daily oral dose of anastrozole 1 mg. The primary end (95% CI, 1.10 to 1.67; P < 0.01). Both treatments were point was time to progression (TTP). Secondary end well tolerated. points included objective response (OR) rate, duration Conclusion: Fulvestrant was at least as effective as of response (DOR), and tolerability. anastrozole, with efficacy end points slightly favoring Results: Patients (n ؍ 400) were followed for a me- fulvestrant. Fulvestrant represents an additional treat- dian period of 16.8 months. Fulvestrant was as effec- ment option for postmenopausal women with ad- tive as anastrozole in terms of TTP (hazard ratio, 0.92; vanced breast cancer whose disease progresses on 95.14% confidence interval [CI], 0.74 to 1.14; P ؍ .43); tamoxifen therapy. median TTP was 5.4 months with fulvestrant and 3.4 J Clin Oncol 20:3386-3395. 2002 by American months with anastrozole. OR rates were 17.5% with Society of Clinical Oncology. both treatments. Clinical benefit rates (complete re-
THE SELECTIVE estrogen receptor modulator (SERM) with ductal carcinoma-in-situ.3 Patients who have tumor
tamoxifen (Nolvadex; AstraZeneca, Wilmington, DE)
progression or develop resistance to tamoxifen are often
is well established as a highly effective treatment for pre-
treated with second-line hormonal therapy. The treatment
and postmenopausal patients with either advanced or early
options currently available comprise the third generation of
breast cancer.1 Tamoxifen has also been shown to be
oral, selective nonsteroidal aromatase inhibitors including
effective in reducing the incidence of breast cancer in
anastrozole, letrozole, and the steroidal agent exemestane.
patients at risk of developing the disease2 and in women
Fulvestrant (Faslodex; AstraZeneca, Macclesfield, UnitedKingdom) is a “pure” estrogen antagonist with a novelmode of action, distinct from that of tamoxifen or any otherantiestrogen currently available. Fulvestrant, like tamox-
From the Breast Center at Baylor College of Medicine, MethodistHospital, US Oncology, and M.D. Anderson Cancer Center, Houston, and
ifen, binds to estrogen receptors (ERs) competitively. How-
Baylor-Sammons Cancer Center, Dallas, TX; Dana-Farber Cancer Insti-
ever, in contrast to tamoxifen, fulvestrant’s binding leads to
tute and Beth Israel Deaconess Medical Center, Boston, MA; Lombardi
rapid degradation and loss of ER protein.4 Furthermore,
Cancer Center, Washington, DC; Ottawa Regional Cancer Center, Ot-
fulvestrant antagonizes all of the transactivating functions
tawa, Ontario, Canada; Hematology Oncology Association VA Ltd,Richmond, VA; Louisiana State University Health Science Center, Shreve-
of the receptor, whereas tamoxifen blocks only one, a
port, LA; and AstraZeneca, Macclesfield, United Kingdom.
feature that contributes to its estrogen agonist activity in
Submitted October 10, 2001; accepted March 22, 2002.
some tissues.4 Accordingly, fulvestrant is the first in a new
Supported by a grant from AstraZeneca Pharmaceuticals, Wilming-
class of antiestrogens—an ER downregulator—and is de-
This article was published ahead of print at www.jco.org.
void of agonist activity.5 Fulvestrant has greater potency
Address reprint requests to C.K. Osborne, MD, Breast Center,
than tamoxifen at inhibiting the growth of breast tumors and
Baylor College of Medicine, 1 Baylor Plaza, MS 600, Houston, TX
doubles the time to the development of resistance in a
77030; email: [email protected].
xenograft murine model of human breast cancer.6 It also
2002 by American Society of Clinical Oncology. 0732-183X/02/2016-3386/$20.00
inhibits growth of tamoxifen-resistant tumors in this mod-
Journal of Clinical Oncology, Vol 20, No 16 (August 15), 2002: pp 3386-3395
FULVESTRANT v ANASTROZOLE IN ADVANCED BREAST CANCER
el.6 In primary breast cancer patients who received a single
The primary end point of the comparison between the two drugs was
injection of fulvestrant (at doses of 50, 125, or 250 mg)
TTP. Secondary end points included OR, duration of response (DOR),time to treatment failure (TTF), time to death (TTD), and tolerability.
14 to 21 days before the initial tumor resection, fulves-
Other secondary end points were quality of life, symptomatic response,
trant produced a dose-dependent reduction in both ER
and pharmacokinetics. Other end points included clinical benefit (CR ϩ
and progesterone receptor (PgR) expression.7 In contrast,
PR ϩ stable disease [SD] Ն 24 weeks) and duration of clinical benefit.
a separate group of patients in the same study who
All data are reported here except pharmacokinetics, which will be
received tamoxifen 20 mg orally before tumor resection
showed an increase in PgR expression, thereby confirm-
ing the partial estrogen agonist activity of tamoxifen. Aphase II study in postmenopausal women with advanced
All patients were postmenopausal women with locally advanced or
metastatic breast cancer whose disease had progressed on adjuvant
breast cancer whose disease progresses after tamoxifen
endocrine therapy with an antiestrogen or whose disease had pro-
therapy given as adjuvant or for advance disease showed
gressed after first-line endocrine therapy for advanced disease. All
that subsequent treatment with fulvestrant was associated
women had a life expectancy of longer than 3 months and tumors with
evidence of hormone sensitivity (ie, prior sensitivity to hormonal
This study provides the first opportunity to compare the
therapy or known ER or PgR positivity).
For inclusion in the trial, patients had to have a World Health
relative efficacy of ER suppression with the ER downregu-
Organization performance status of Յ 2, histologic or cytologic
lator fulvestrant with that of anastrozole, as second-line
confirmation of breast cancer, objective evidence of recurrence or
therapy in patients with potentially hormone-dependent
progression of disease that was not amenable to curative treatment, and
the presence of at least one measurable or assessable (nonmeasurable)lesion. All patients had to be postmenopausal (ie, Ն 60 years old or
aged Ն 45 years with amenorrhea for Ͼ 12 months or follicle-stimulating hormone levels within postmenopausal range, or havingundergone a bilateral oophorectomy).
Exclusion criteria included the following: the presence of life-
threatening metastatic visceral disease (defined as extensive hepatic
The study (trial 0021) was a randomized, double-blind, double-
involvement) or any degree of brain or leptomeningeal involvement;
dummy, phase III trial conducted in North America. The trial was
symptomatic pulmonary lymphangitic spread; prior treatment for breast
originally designed to compare two doses of fulvestrant (125 mg and
cancer with fulvestrant or any aromatase inhibitor; more than one prior
250 mg per month) as an intramuscular injection with anastrozole as a
endocrine medical treatment for advanced breast cancer; extensive
1 mg/d oral dose. A nonblinded, open-label trial using the same drug
radiation therapy or cytotoxic treatment within the past 4 weeks;
doses and a similar protocol (trial 0020) was conducted concurrently in
estrogen replacement therapy within 4 weeks of randomization; treat-
Europe, South Africa, and Australia (see accompanying article in this
ment with luteinizing hormone–releasing hormone analogs within 3
issue of the Journal of Clinical Oncology).11
months before randomization; and any concurrent medical illness or
A preliminary data summary and an interim analysis were planned
laboratory abnormalities that would compromise safety or prevent
and conducted to determine the clinical activity of fulvestrant 125 mg,
which had not been previously tested. Therefore both trials included a
Subjects taking bisphosphonates for bone disease were permitted
preliminary data summary stage after the first 30 subjects in the
to enter the trial, but their bone lesions were not considered to be
fulvestrant 125-mg group (combined from both trials) had been treated
assessable for response, although they were assessable for progres-
and followed up for 3 months. This interim assessment showed
sion. Initiation of bisphosphonate treatment during the trial was
insufficient evidence of clinical activity for fulvestrant 125 mg with no
discouraged but allowed in the absence of objective evidence of
objective tumor responses at 3 months. The independent data monitor-
progression. If bisphosphonates were commenced, bone lesions
ing committee therefore recommended that recruitment to the fulves-
trant 125-mg treatment arm be stopped. Patients already recruited into
All patients provided written informed consent, and the relevant
the 125-mg arm in trial 0021 were permitted to remain on fulvestrant
ethical committees approved the studies.
125 mg or withdraw from the trial and be placed on other treatments atthe discretion of their clinician. These patients were not monitored
further for efficacy. The lack of an objective response in the low-dosefulvestrant arm also suggests that response due to tamoxifen with-
Fulvestrant was supplied in vials as a single-dose, castor oil– based,
drawal in this study must be uncommon. As a consequence of dropping
5% solution. Each vial contained 250 mg of fulvestrant at a concen-
this treatment arm, the protocol for the study was amended to compare
tration of 50 mg/mL in a volume of 5 mL. The matched placebo was
fulvestrant 250 mg with anastrozole 1 mg.
5 mL of the oily excipient. Fulvestrant 250 mg or matching placebo
An interim analysis was conducted when 170 progressions or deaths
was administered slowly as a 2.5-mL injection into each buttock.
had occurred across the remaining arms and time to progression (TTP)
Injections were given once a month, which was defined as every 28
was formally analyzed. The rate of objective response (OR; defined as
complete response [CR] ϩ partial response [PR] using Union Interna-
Anastrozole (Arimidex) 1 mg and matching placebo were supplied
tionale Contre le Cancer criteria) and adverse event (AE) data were
as round, white, film-coated tablets and administered orally once daily.
summarized. As a result of the interim analysis, the independent data
Medical personnel saw all patients on a monthly basis because all
monitoring committee recommended that the trial should continue.
patients required fulvestrant or placebo injections.
Patients continued treatment until objective disease progression or
TTF was defined as the number of days from randomization
other events required withdrawal; at such time, trial treatment was
until the earliest occurrence of disease progression, death from any
stopped and standard therapy was initiated at the discretion of the
cause, or withdrawal from trial treatment for any reason. Patients
treating physician. Thereafter, patients were followed up until death.
whose treatment had not failed at the time of analysis were right-
Patients who withdrew from trial treatment before progression were
censored in the analysis at the time of their last assessment. Any patient
followed up until objective disease progression and death.
who did not receive any trial therapy was assigned an uncensored TTF
All patients were seen by a physician to make objective tumor
of zero days. Statistically, TTF was analyzed in the same way as TTP.
assessments every 3 months until evidence of either objective disease
Responders were defined as those patients with a CR or
progression or death. Patients with skin and soft tissue lesions were also
PR. To qualify as a responder, the patient had to satisfy the criteria for
assessed every month during the first 3 months of treatment.
CR or PR on one visit with no evidence of disease recurrence or deathwithin 4 weeks after assessment. Treatment differences in OR were
assessed by comparing the proportion of responders using a logistic
The trial was designed to detect the superiority of fulvestrant 250 mg
regression model (with the same covariates as for TTP). The estimate
in terms of efficacy and tolerability compared with anastrozole 1 mg in
of the treatment effect is expressed as an odds ratio (fulvestrant/
postmenopausal women with advanced breast cancer.
anastrozole), together with the corresponding CI and P value. In
The final analysis was scheduled to occur when 340 events (ie,
addition, an estimate of the difference in response rates (fulvestrant/
objective disease progression or death) had occurred across the two
anastrozole) and corresponding CI was also produced.
groups. This provided 90% power to detect a hazard ratio (HR) Ն 1.43
The DOR was defined for responding patients only as the
or Յ 0.70 for fulvestrant treatment compared with anastrozole treat-
period of time from randomization to the first observation of disease
ment, at a significance level of 5%. It was therefore planned to recruit
progression. Patients who died before reaching progression were
392 patients (196 in each treatment group) to achieve the required
classified as completing their response at time of death. The DOR was
summarized using Kaplan-Meier curves for each treatment group, and
The efficacy analyses were performed according to randomized
the median DOR was also calculated for each group.
treatment (ie, “intention to treat”) using a nominal significance level of
No statistical comparison was performed for DOR in only those
5%. However, for the TTP and OR analyses, the significance level was
patients responding to treatment, because this is not a randomized
adjusted to 4.86% because of the preliminary data summary of OR and
comparison. Rather, all patients were included in a statistical analysis
the interim analysis of TTP. As a result, the 95% confidence intervals
of DOR, defined for responders as the time from onset of response to
(CIs) were adjusted accordingly to 95.14%. All significance levels are
disease progression and for nonresponders as zero. These data were
also summarized using Kaplan-Meier curves.
Although not described in the protocol, fulvestrant was retrospec-
Clinical benefit was defined as the sum of CR ϩ
tively compared with anastrozole for noninferiority for OR, TTP, and
PR ϩ SD Ն 24 weeks. Although a formal analysis of clinical benefit
TTF. Because of the interim analysis, a one-sided CI of 97.57% was
was not protocoled, treatment differences in the rate of clinical benefit
used for the evaluation of TTP and OR. For the analysis of TTF, a
were retrospectively assessed in the same way as that of OR rate. The
one-sided CI of 97.5% was used. These limits are identical to using the
duration of clinical benefit was presented as for DOR.
upper limit of the 95.14% two-sided CI from the analysis of TTP, the
As specified in the protocol, TTD (overall survival) will be
lower limit of the 95.14% two-sided CI for the difference in response
analyzed when more than 50% of the patients have died. At the time of
rates for OR, and the upper limit of the 95% two-sided CI for TTF.
this data analysis, only 34.5% of patients had died; therefore, no formal
For previous United States regulatory submissions of hormonal
statistical analyses were conducted.
treatments for advanced breast cancer, the requirements for showingnoninferiority for TTP were based on the upper one-sided confidence
limit for the TTP HR not being greater than 1.25 (ie, a potential
Any detrimental change in a patient’s condition subsequent to them
deficiency of Ͼ 25% for the experimental treatment had to be ruled
entering the trial and during the follow-up period after the final
out). In the same submissions, the requirement for demonstrating
treatment (8 weeks after last injection or 30 days after the last tablet,
noninferiority in terms of response rate was based on ruling out a
whichever was the greater), which was not unequivocally due to
deficiency in the difference in response rates of more than 10%.
progression of disease, was considered to be an AE. No formal
Consequently, these criteria have been used to assess noninferiority of
statistical analyses were performed on the safety data from this
fulvestrant relative to anastrozole in this trial.
individual trial. However, a planned statistical analysis of predefined
TTP was defined as the time from randomization until
AEs was performed on the combined data from this trial and the
objective disease progression or death from any cause before progres-
multinational trial; this will be reported elsewhere. The most common
sion. Subjects who had not progressed at the time of analysis were
AEs (occurring at an incidence of Ն 10%) and most common
right-censored using the last assessment date. Treatments were com-
drug-related AEs are reported here by treatment received.
pared using Cox’s proportional hazards regression model (including thecovariates age, performance status, measurable compared with non-
measurable disease, receptor status, previous response to hormonetherapy, previous use of cytotoxic chemotherapy, and use of bisphos-
Quality of life (QOL) was assessed using the Functional Assessment
phonate therapy for bone disease). A global test was performed to
of Cancer Therapy (FACT)–Breast questionnaire, which is composed
determine whether there were significant treatment-by-baseline covari-
of the FACT-General QOL tool for cancer patients plus the breast
ate interactions. The estimate of the treatment effect was expressed as
cancer subscale. This questionnaire has been extensively validated in
an HR (fulvestrant/anastrozole), together with the corresponding CI
respect to psychometric properties and sensitivity to clinical chang-
and P value. TTP was also summarized using Kaplan-Meier curves for
es12,13 and is in use in a number of large breast cancer treatment trials
each treatment group, and the median TTP was calculated.
FULVESTRANT v ANASTROZOLE IN ADVANCED BREAST CANCER
The analysis was undertaken on data collected up to the date of
Table 1. Demographic and Pretreatment Characteristics
progression using the trial outcome index (TOI) within the FACT-
Breast. This measure is the sum of the functional well-being, physical
well-being and breast cancer subscale dimensions of the questionnaire.
The difference in TOI over time between the fulvestrant 250-mg
group and the anastrozole 1-mg group was compared using a general-
ized linear mixed model (ie, a random coefficients model) with the
same covariates as for TTP. A graph of the mean TOI (Ϯ standard
deviation) over time was also produced.
A total of 400 patients randomized to either fulvestrant
250 mg (n ϭ 206) or to anastrozole (n ϭ 194) were
followed for a median period of 16.8 months. The majority
(95% of the fulvestrant group and 96% of the anastrozole
group) had been treated previously with tamoxifen either as
adjuvant therapy or as initial therapy for advanced disease.
Metastatic or recurrent disease at baseline
Ninety-four patients in each group had received endocrine
therapy as adjuvant treatment. Of these, 67 patients in the
fulvestrant group and 75 patients in the anastrozole group
stopped treatment less than 365 days before randomization.
The characteristics of the patients are presented in Table
1. Patients in the fulvestrant and the anastrozole groups
were similar for age, weight, breast cancer history, and ER
Extent of metastatic or recurrent disease at
At the time of analysis, 83.5% of the fulvestrant
group and 86.1% of the anastrozole group had experienced
disease progression. There was no significant difference for
TTP between the two treatment groups (HR, 0.92; 95.14%
CI, 0.74 to 1.14; P ϭ .43). The HR (0.92) indicates that the
NOTE. Patients may be in more than one category.
risk of progression (over a given period of time) for patients
Abbreviations: ER, estrogen receptor; PgR, progesterone receptor.
randomized to fulvestrant was 8% lower than it was for
*Mixed is defined as breast and/or a combination of skin, bone, liver, lung,
patients randomized to anastrozole. The 95.14% CI indi-
cates that the risk of progression for patients randomized to
†Measurable lesions were lesions that were clinically measurable in two
perpendicular axes with at least one dimension being Ն 2.5 cm or measurable
fulvestrant 250 mg could be between 26% lower and 14%
using imaging in two perpendicular axes with at least one dimension being Ն
higher than it is for patients randomized to anastrozole.
These data demonstrate noninferiority of fulvestrant relativeto anastrozole. Median TTP was 5.4 months for fulvestrantand 3.4 months for anastrozole (Fig 1).
(HR, 0.96; 95% CI, 0.77 to 1.19; P ϭ .69) (Fig 2). The
The majority of treatment failures were due to
data also satisfy the criteria for noninferiority. Median
objective disease progression (94%), and accordingly, the
TTF was 4.6 months for fulvestrant (n ϭ 206) and 3.3
Kaplan-Meier curves for TTP and TTF are very similar. For
fulvestrant, there were 164 treatment failures (79.6%) be-
cause of disease progression; for anastrozole, there were
OR in 36 patients (17.5%), while anastrozole produced an
163 (84.0%). Other reasons for treatment failures in-
OR in 34 patients (17.5%) (Table 2). There was no
cluded AEs, protocol noncompliance, and withdrawal of
statistically significant difference in OR between fulvestrant
informed consent. TTF was similar for the two groups,
and anastrozole (difference in response rates, 0.17%;
with there being no significant difference between them
95.14% CI, Ϫ6.31% to 9.30%). The lower CI shows
Fig 1. Kaplan-Meier estimates for time to progression.
noninferiority of fulvestrant relative to anastrozole. The
patients—where DOR was defined as from the onset of
odds ratio for achieving an OR in the fulvestrant group
response to disease progression for responders and zero for
versus the anastrozole group was 1.01 (95.14% CI, 0.59 to
nonresponders—was significantly greater for fulvestrant
compared with anastrozole (ratio of average response dura-
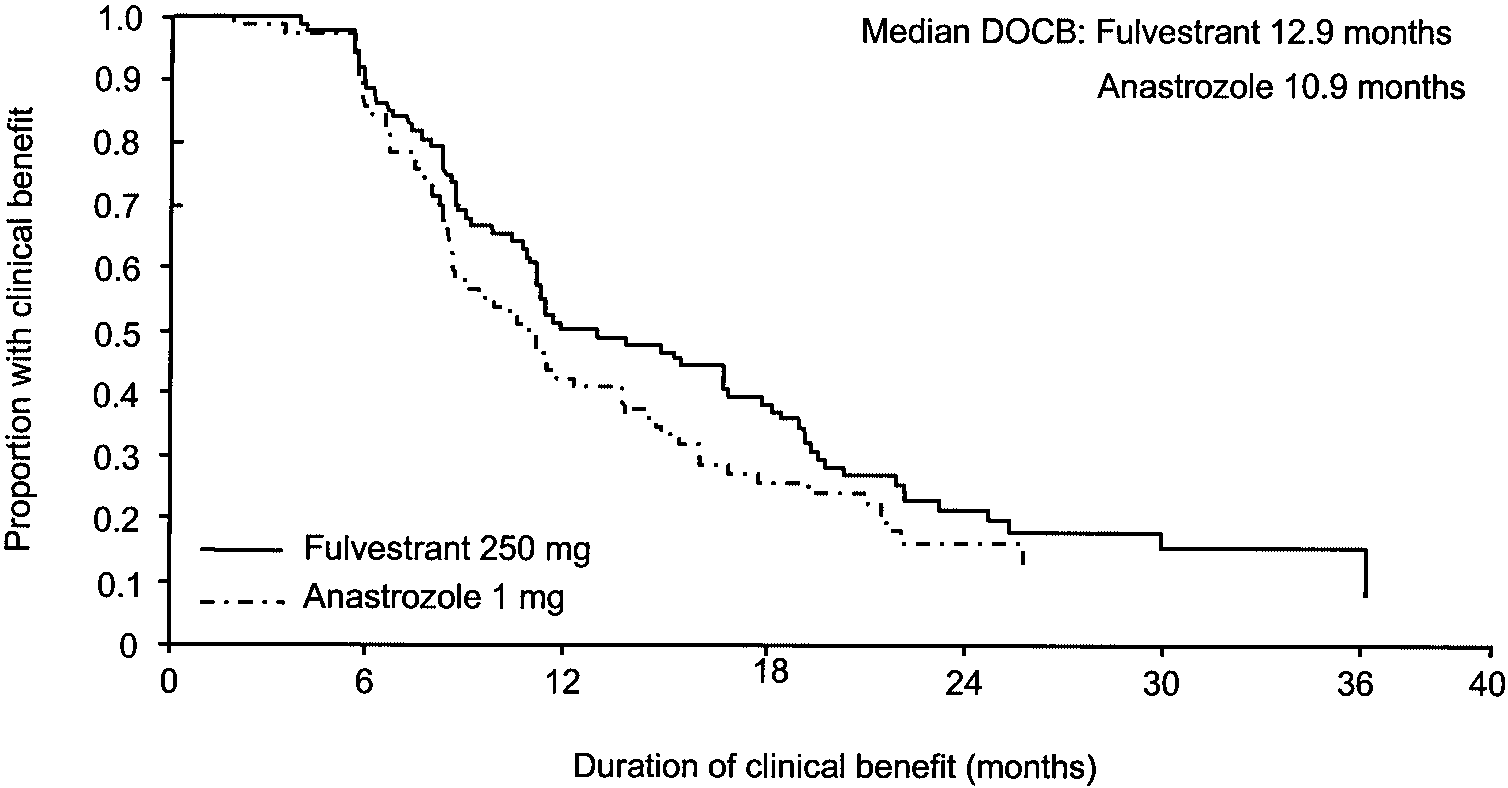
Clinical benefit rates of 42.2% and 36.1% were observed
tions, 1.35; 95% CI, 1.10 to 1.67; P Ͻ .01). The Kaplan-
for fulvestrant and anastrozole, respectively (Table 2), with
Meier curves for DOR in all patients are shown in Fig 4.
the analysis showing no statistically significant difference
The median duration of clinical benefit was 12.9 months for
(difference in clinical benefit rates, 5.83%; 95% CI,
fulvestrant (n ϭ 87) and 10.9 months for anastrozole (n ϭ
Extended follow-up was performed in order to obtain
At the time of this data analysis, a similar
more complete information for DOR (median follow-up,
number of deaths had occurred in each treatment group
21.3 months). The median DOR, as measured from random-
(fulvestrant, n ϭ 73 [35.4%]; anastrozole, n ϭ 65
ization to progression, in those patients who responded to
[33.5%]). However, as specified in the protocol, TTD
treatment was 19.0 months for fulvestrant (n ϭ 36) and 10.8
(overall survival) will be analyzed when more than 50%
months for anastrozole (n ϭ 34). The Kaplan-Meier curves
of the patients have died. Consequently, no formal
for the DOR are shown in Fig 3. In addition, DOR using all
statistical analyses have been conducted on these data. In
Fig 2. Kaplan-Meier estimates for time to treatment failure.
FULVESTRANT v ANASTROZOLE IN ADVANCED BREAST CANCER
Table 2. Best Objective Responses for Fulvestrant 250 mg IM or
were generally similar between treatment groups. The
Anastrozole 1 mg Orally od
most common drug-related AEs are shown in Table 4.
The incidence of hot flashes was similar for both drugs
(23.5% for fulvestrant and 24.9% for anastrozole).
The incidence of weight gain (fulvestrant v anastrozole:
1.5% v 1.6%), vaginitis (3.4% v2.6%), and thromboem-
bolic disease (3.4% v 6.7%) was low for both fulvestrant
and anastrozole. Joint disorders (including arthritis,
arthralgia, and arthrosis) were reported by 9.3% and
13.5% of patients in the fulvestrant and anastrozole
total 6,908 monthly injections: 3,752 injections in the
fulvestrant group and 3,156 placebo injections in the anas-
Abbreviations: CR, complete response; PR, partial response; SD, stable
trozole group. Fifty-five patients (27.0%) receiving fulves-
trant and 45 patients (23.3%) receiving anastrozole (plusplacebo injection) reported injection site reactions. Overall,
line with the study protocol, TTD analyses will be
86 fulvestrant courses (4.6%) of the total of 1,879 and 71
placebo courses (4.4%) of the total of 1,624 resulted in aninjection site event. Most of these events were charac-
terized as injection site pain, reaction, and/or inflamma-
Both fulvestrant and anastrozole were well tolerated,
tion. None of these events was serious, and only one
with only five fulvestrant patients (2.5%) and five anas-
patient complained of severe injection site pain and
trozole patients (2.6%) withdrawing because of AEs. The
requested to be withdrawn from fulvestrant treatment (the
profile of AEs (thought to be drug-related or not) was
investigator did not consider the event to be drug
similar for the two drugs, and patients in both treatment
related). Two anastrozole-treated patients given placebo
groups reported a wide range of AEs. The most fre-
injections were also withdrawn because of AEs related to
quently reported AEs, graded according to Coding Sym-
(COSTART) classification, are shown in Table 3 andincluded asthenia, nausea, pain, headache, vasodilatation,
A graph of the mean TOI (Ϯ standard deviation) over
pharyngitis, dyspnea, back pain, bone pain, and vomiting.
time is shown in Fig 6. The analysis of QOL data up to the
The incidence and severity (most were mild) of events
date of progression showed that QOL was maintained over
3. Kaplan-Meier mates for duration of response. 4. Kaplan-Meier mates for duration of response (all patients).
time and that the two treatments were not statistically
significantly greater in the fulvestrant group than in the
anastrozole group. The clinically durable response observedwith fulvestrant is in accordance with preclinical observa-
tions in tumor models, where fulvestrant was shown to
This North American, randomized, double-blind, double-
double the DOR compared with tamoxifen or withdrawal of
dummy, phase III study in postmenopausal women with
estrogen,6 as well as with phase II clinical data,10 where
advanced breast cancer was designed to compare the effi-
long responses were observed in tamoxifen-resistant, ad-
cacy and tolerability of fulvestrant with that of the well-
vanced breast cancer patients. Furthermore, in the clinical
established third-generation aromatase inhibitor anastro-
benefit group, where patient numbers were higher, the
zole. Although the results did not show superiority of
duration of clinical benefit also favored fulvestrant. With
fulvestrant over anastrozole, the primary analysis of TTP
respect to other end points of the study, fulvestrant showed
showed fulvestrant to be at least as effective as anastrozole.
a numerical improvement in TTP (median, 5.4 months) and
The CIs observed for TTP, TTF, and OR for the two
TTF (median, 4.6 months) compared with anastrozole
hormone agents allow us to rule out inferiority of fulvestrant
(median, 3.4 and 3.3 months, respectively), although the
to anastrozole. Furthermore, DOR using all patients was
analyses of TTP and TTF showed no statistically significant
5. Kaplan-Meier mates for duration of clinical benefit (DOCB).
FULVESTRANT v ANASTROZOLE IN ADVANCED BREAST CANCER
differences. OR was identical in the fulvestrant and anastrozole
tively protocoled for the combined data from this North
groups (17.5%). A greater number of patients in the fulvestrant
American trial 0021 and the multinational trial 0020.
group achieved long-term SD, giving a slightly higher clinical
These results will be presented separately; therefore, the
benefit rate (42.2% for fulvestrant v 36.1% for anastrozole),
comparative tolerability of fulvestrant and anastrozole in
although the analysis of clinical benefit rate showed no
the present study is not discussed further.
statistically significant difference. Thus, trends for all major
With regard to the route of administration, fulvestrant
end points favored fulvestrant. Reassuringly, the summary data
was well tolerated, with only one patient withdrawing from
of QOL showed that the use of fulvestrant in this patient
treatment because of an injection site reaction. The data
population maintained QOL as well as anastrozole did. It is
from the placebo treatment in the anastrozole arm provided
premature to perform survival analyses, which by protocol
confirmation that injection site reactions to fulvestrant are
design require that more than 50% of patients have died. Given
related to the injection itself (or the excipients used to carry
the results to date and the multiple additional therapies given
fulvestrant) and not to the local effects of fulvestrant itself.
after progression in such patients, it seems highly unlikely that
Injection site reactions were also few in the companion
patients randomized to fulvestrant would have worse overall
multinational study, in which patients received a larger
survival. The double-dummy design provided the opportunity
single 5-mL injection. A potential advantage of the paren-
to determine more thoroughly the toxicity profile of fulves-
teral injection is that compliance, which can be a problem
trant. In this trial, fulvestrant and anastrozole were both very
(particularly in elderly patients), can be assured.
well tolerated, with the AE profile for fulvestrant being similar
This study confirms that an antiestrogen with a dominant
to that of anastrozole. Similar numbers of AEs were observed
estrogen antagonist profile and unique mechanism of action
in both treatment arms, with the majority being mild. Most
can induce long remissions in tumors with acquired resistance
importantly, a low percentage of patients in each group
to tamoxifen, a SERM with mixed agonist/antagonist proper-
withdrew because of AEs (2.5% with fulvestrant v 2.6%
ties. This lack of cross-resistance between tamoxifen and
with anastrozole). Many of the AEs in both groups could
fulvestrant has not been observed clinically with other anties-
have been related more to the serious underlying and
trogens. Raloxifene was found to be ineffective in metastatic
progressive disease or to concomitant therapy (eg, opi-
breast cancer patients who were refractory to tamoxifen.14,15
ates for pain). Statistical analysis of AEs was prospec-
Multiple phase II metastatic breast cancer trials investigatingtoremifene in tamoxifen-refractory patients also demonstratedcross-resistance to tamoxifen.16,17 Clearly, the fact that fulves-
Table 3. Most Common Adverse Effects Occurring in > 10% of Patients
trant is effective in women progressing after prior tamoxifen
therapy emphasizes that it has a mode of action distinct from
that of tamoxifen and the other SERMs.
The results of trial 0021 are similar to those found in the
another multinational trial (0020), also published in this of
the Journal.11 The difference in DOR between fulvestrant
and anastrozole, as measured from randomization to pro-
gression, in those patients who responded to treatment was
greater in trial 0021 compared with trial 0020. However, the
Table 4. Drug-Related Adverse Events Occurring in > 3% of Patients in Either Group (excluding injection site reactions) Fig 6. Quality of life: observed mean (؎ standard deviation) treatment outcome index over time.
DOR using all patients, where DOR was defined as from the
ER-positive, which could also have influenced benefit
onset of response to disease progression for responders and as
from treatments designed to target the receptor. Finally,
zero for nonresponders, was significantly greater for fulves-
patients in trial 0021 had greater body weight and had
trant compared with anastrozole in both trials. An advantage
more frequently received prior chemotherapy, although it
for fulvestrant compared with estrogen deprivation or tamox-
is not clear how these differences could affect the results.
ifen treatment was also shown in a preclinical model, leading
In conclusion, this study shows that fulvestrant is the first
to the hypothesis that it might take breast cancer cells longer to
antiestrogen to show clinically relevant activity in tamox-
develop resistance to fulvestrant.6 Although the difference in
ifen-resistant advanced breast cancer, confirming that ful-
these clinical trials could be a chance finding, there were some
vestrant represents the first of a new class of antiestrogen.
differences in the trials that could contribute to this discrep-
Although fulvestrant was not statistically significantly su-
ancy. In trial 0021, all patients were seen monthly by
perior to anastrozole, it is the first antiestrogen to be at least
medical personnel to receive injections; therefore, dis-
as effective as anastrozole in the treatment of patients with
ease symptoms could be followed more closely. In trial
advanced breast cancer whose disease has progressed after
0020, only fulvestrant patients were seen monthly,
prior endocrine treatment. Given its efficacy and tolerability
whereas patients receiving anastrozole were followed up
profile, fulvestrant will provide a new endocrine treatment
every 3 months, potentially biasing efficacy in favor of
option for the management of women with advanced breast
anastrozole. More patients in trial 0021 were known to be
The appendix listing fulvestrant study group investigators is available online at www.jco.org.
1. Jaiyesimi IA, Buzdar AU, Decker DA, et al: Use of tamoxifen
3. Fisher B, Dignam J, Wolmark N, et al: Tamoxifen in treatment
for breast cancer: Twenty-eight years later. J Clin Oncol 13:513-
of intraductal breast cancer: National Surgical Adjuvant Breast and
Bowel Project B-24 randomised controlled trial. Lancet 353:1993-
2. Fisher B, Costantino JP, Wickerham DL, et al: Tamoxifen for
prevention of breast cancer: Report of the National Surgical Adjuvant
4. Howell A, Osborne CK, Morris C, et al: ICI 182,780 (Faslo-
Breast and Bowel Project P-1 study. J Natl Cancer Inst 90:1371-1388,
dex™): Development of a novel, ‘pure’ antiestrogen. Cancer 89:817-
FULVESTRANT v ANASTROZOLE IN ADVANCED BREAST CANCER
5. Wakeling AE, Dukes M, Bowler J: A potent specific pure
11. Howell A, Robertson JFR, Quaresma Albano J, et al: Fulves-
antioestrogen with clinical potential. Cancer Res 51:3867-3873,
trant, formerly ICI 182,780, is as effective as anastrozole in postmeno-
pausal women with advanced breast cancer progressing after prior
6. Osborne CK, Coronado Heinsohn EB, Hilsenbeck SG, et al:
endocrine treatment. J Clin Oncol 20:3396-3403, 2002
Comparison of the effects of a pure steroidal antiestrogen with those of
12. Cella DF, Tulsky DS, Gray G, et al: The Functional Assessment
tamoxifen in a model of human breast cancer. J Natl Cancer Inst
of Cancer Therapy Scale: Development and validation of the general
7. Robertson JFR, Nicholson RI, Bundred NJ, et al: Comparison of
13. Brady MJ, Cella DF, Mo F, et al: Reliability and validity of the
Functional Assessment of Cancer Therapy-Breast quality-of-life instru-
the short-term biological effects of fulvestrant (ICI 182,780) with
tamoxifen in postmenopausal women with primary breast cancer.
14. Buzdar AU, Marcus C, Holmes F: Phase II evaluations
Breast Cancer Res Treat 59:99, 2000 (abstr)
of LY156758 in metastatic breast cancer. Oncology 45:344-345,
8. Howell A, DeFriend D, Robertson J, et al: Response to a specific
antiestrogen (ICI 182,780) in tamoxifen-resistant breast cancer. Lancet
15. Gradishar W, Glusman J, Lu Y, et al: Effects of high dose
raloxifene in selected patients with advanced breast carcinoma. Cancer
9. Howell A, DeFriend DJ, Robertson JFR, et al: Pharmacokinetics,
pharmacological, and anti-tumour effects of the specific anti-oestrogen
16. Vogel CL, Shermano I, Schoenfelder J, et al: Multicenter phase
ICI 182,780 in women with advanced breast cancer. Br J Cancer
II efficacy trial of toremifene in tamoxifen refractory patients with
advanced breast cancer. J Clin Oncol 11:345-350, 1993
10. Robertson JFR, Howell A, De Friend DJ, et al: Duration of
17. Pyrhonen S, Valavaara R, Vuorinen J, et al: High dose
remission to ICI 182,780 compared to megestrol acetate in tamoxifen
toremifene in advanced breast cancer resistant to or relapsed during
resistant breast cancer. Breast 6:186-189, 1997
tamoxifen treatment. Breast Cancer Res Treat 29:223-228, 1994
Feeste in die Ou Testament, en hul invloed in die Nuwe-Testamentiese tyd§ God vorm die sentrum (allerheiligste in § Feeste verbind die groot dade van God in die verlede met die ervaring van die hede, en die hoop vir die toekoms§ Feeste weerspieël iets van die tydloosheid Feesgeleentheid Die uittog as simbool van die verhouding tussen God en Israel uitgedruk in beelde van liefde en die
1. James A. Lin, C.-L., Shyu, and Tzong-Shyuan Lee . 1994. Establishment of Mycoplasma spp. cleaning program in a breeder farm combined with Ofloxacin. Taiwan J. Vet. Med. Ani. Husb . 2. James A. Lin, Tzong-Shyuan Lee , J.-S. Wang and K.-T. Tong. 1995. The artifical Taiwan J. Vet. Med. Anim. Husb . 65: 147-152. 3. James A. Lin and Tzong-Shyuan Lee. 1995. The application of E
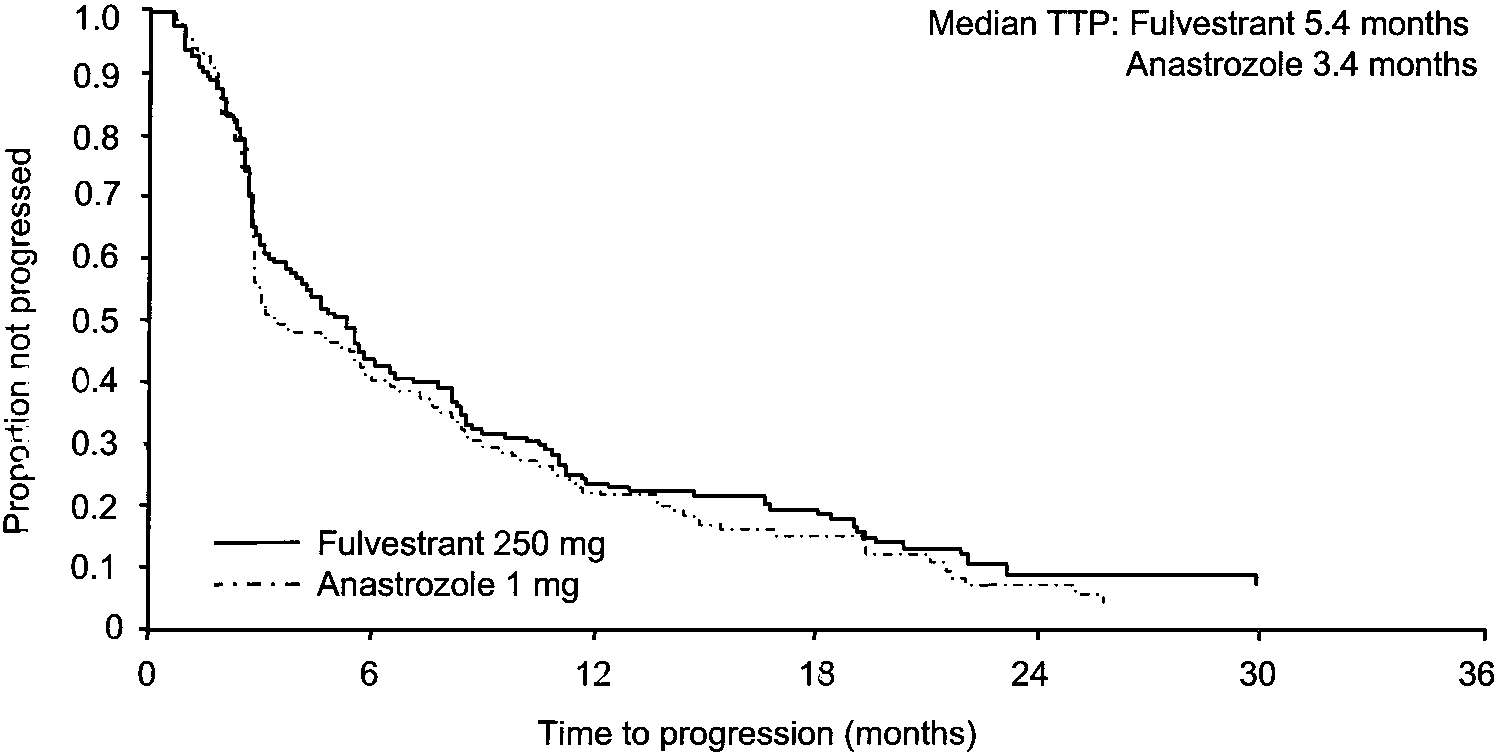
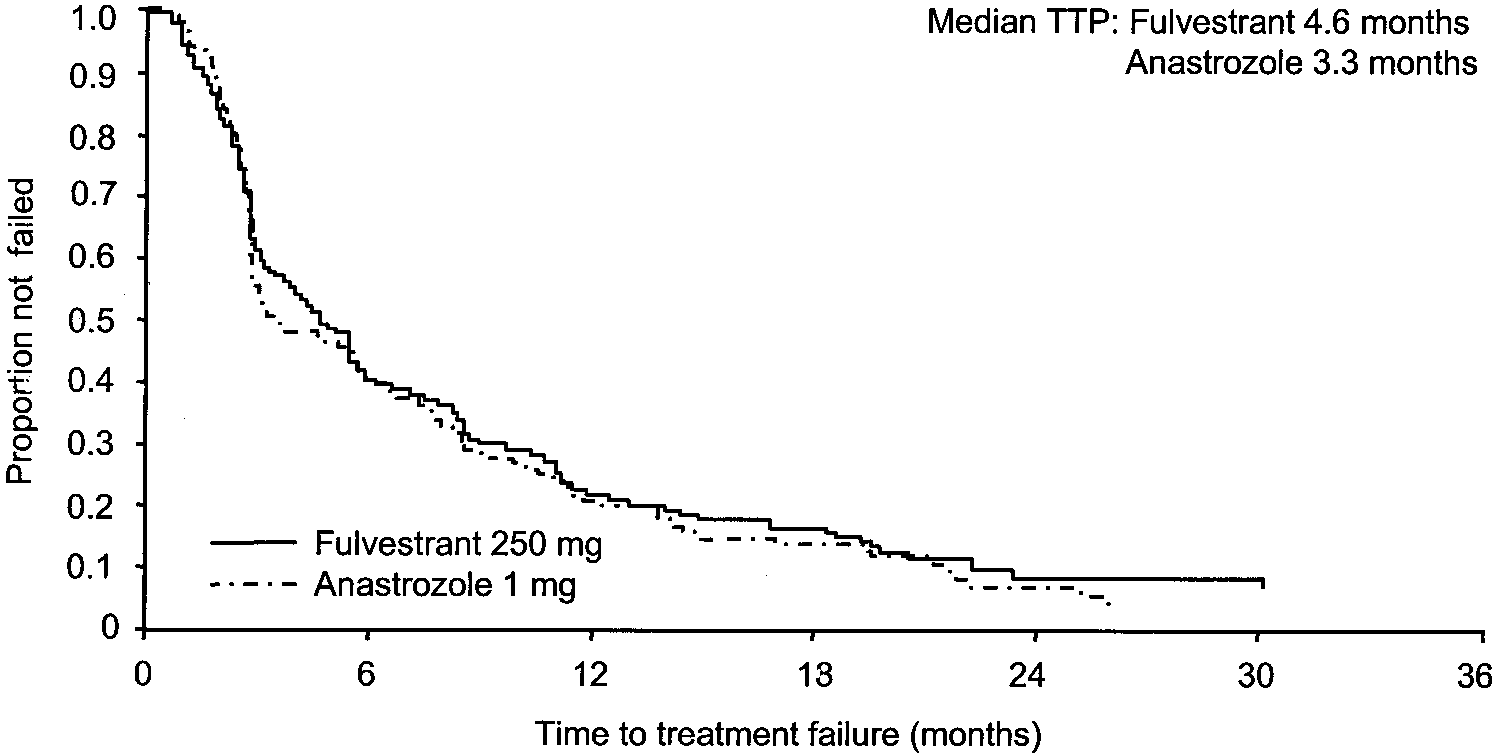 Fig 1. Kaplan-Meier estimates
Fig 1. Kaplan-Meier estimates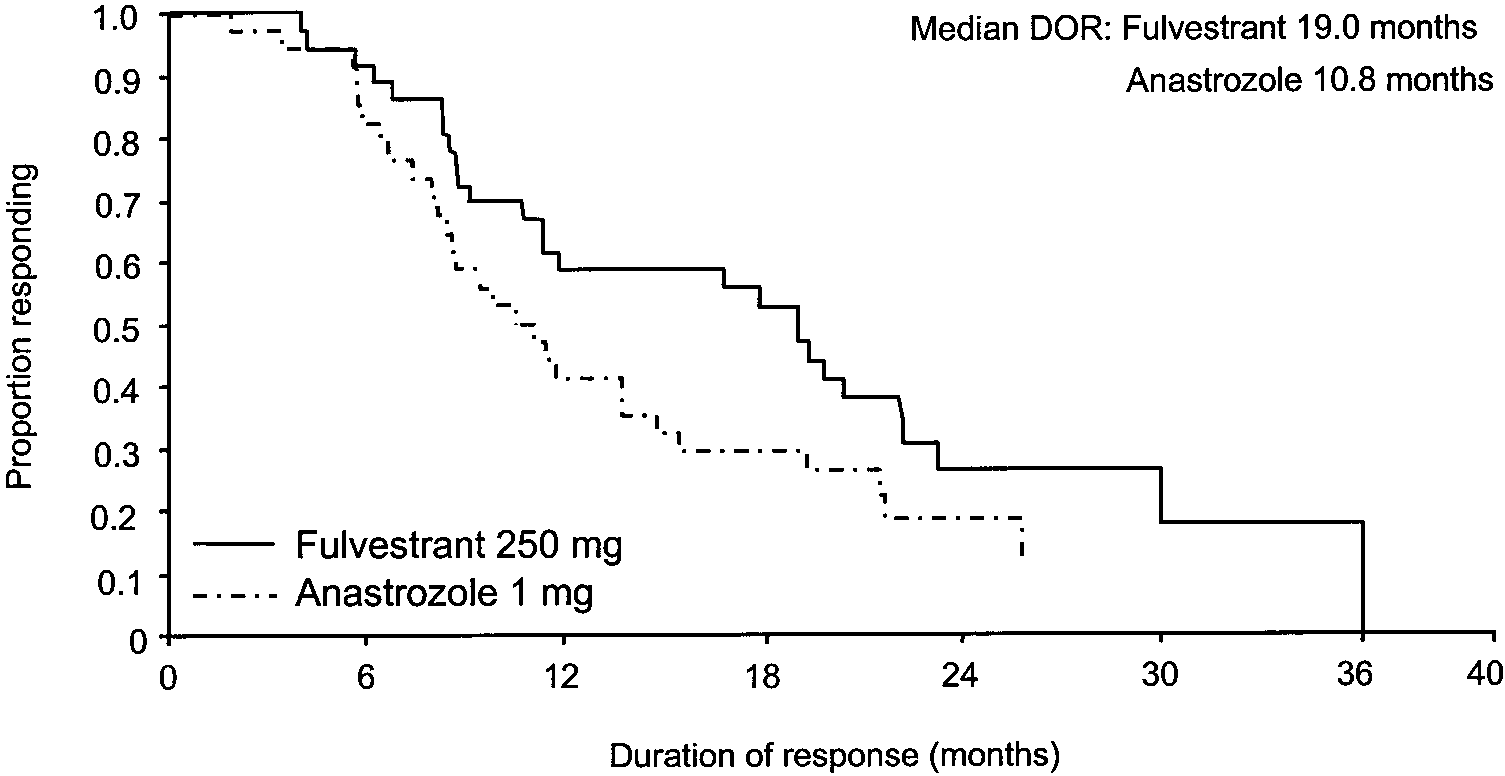 FULVESTRANT v ANASTROZOLE IN ADVANCED BREAST CANCER
Table 2. Best Objective Responses for Fulvestrant 250 mg IM or
FULVESTRANT v ANASTROZOLE IN ADVANCED BREAST CANCER
Table 2. Best Objective Responses for Fulvestrant 250 mg IM or
 4. Kaplan-Meier
4. Kaplan-Meier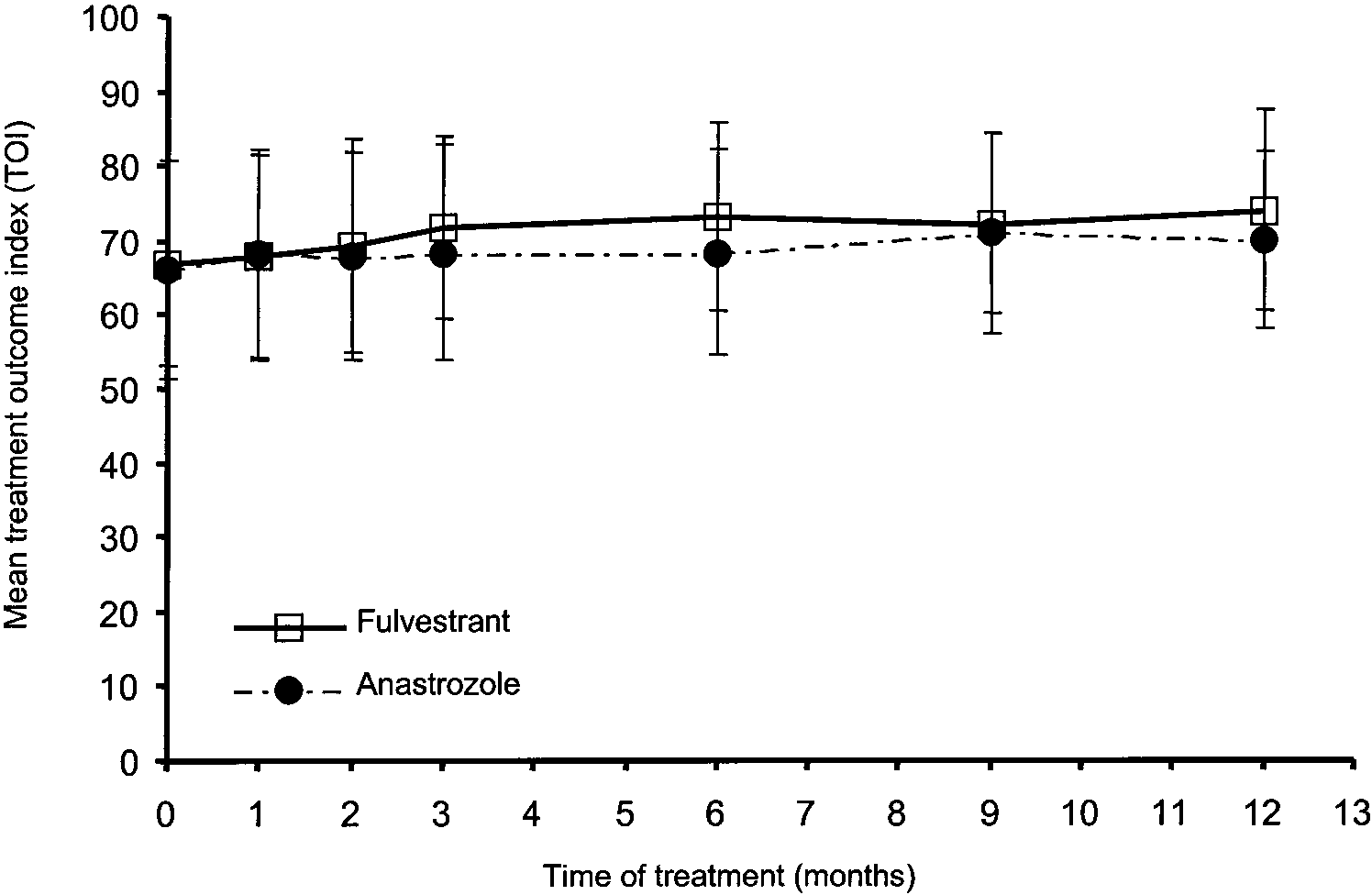 Fig 6. Quality of life: observed
Fig 6. Quality of life: observed