AHA Scientific Statement Supplement to the Guidelines for the Management of Transient Ischemic Attacks A Statement From the Ad Hoc Committee on Guidelines for the Management of Transient Ischemic Attacks, Stroke Council, American Heart Association
Gregory W. Albers, MD, Chair; Robert G. Hart, MD; Helmi L. Lutsep, MD;
In 1994, a panel of the American Heart Association Stroke of these conditions, although few of these studies were
Council published guidelines for the management of tran-
sient ischemic attacks (TIAs).1 Over the last 5 years, many
Reduction of both systolic and diastolic pressure in hyper-
significant advances in medical and surgical therapy for
tensive subjects substantially reduces stroke risk.4,5 Reduc-
patients with TIAs have occurred. In addition, new data
tion of isolated systolic hypertension to Ͻ140 mm Hg in the
regarding risk factors for cerebral ischemic events have
elderly, for example, in the recently completed Syst-Eur trial6
become available. These scientific advances have prompted
demonstrated that treatment of older patients with isolated
this supplement to the 1994 guidelines, which provides
systolic hypertension led to a 42% reduction in stroke risk
updated recommendations for management of patients with
with no significant decline in overall mortality. Current
guidelines for the treatment of hypertension have been
Specific stroke-prevention strategies after a TIA are tai-
published by the Joint National Committee on Prevention,
lored to the most likely cause of the event and the patient’s
Detection, Evaluation, and Treatment of High Blood
underlying risk factors as determined by a focused, expedient
diagnostic evaluation. For more information about epidemi-
Diabetes mellitus is a well-established stroke risk factor.8,9
ology, etiology, and diagnostic evaluation of TIAs, see the
Death due to cerebrovascular disease is substantially in-
original guidelines.1 For the current report, panel members
creased in patients with 2-hour blood glucose values above
followed the rules of evidence used by the 1998 American
the 97.5 percentile compared with those with values below
College of Chest Physicians Conference on Antithrombotic
the 80th percentile.10 Intensive treatment of both type 1 and
type 2 diabetes, aimed at obtaining near-normal levels ofblood glucose, can substantially reduce the risk of microvas-
Risk Factor Modification
cular complications such as retinopathy, nephropathy, and
The approach to stroke prevention among patients who have
neuropathy but has not been conclusively shown to reduce
already had their first TIA includes identification and modi-
macrovascular complications, including stroke.11–14 One re-
fication of stroke risk factors. Nonmodifiable risk markers for
cent study13 demonstrated that aggressive treatment of blood
stroke include age, sex, race-ethnicity, and heredity.3 Al-
pressure in persons with type 2 diabetes reduced the risk of
though these risk markers cannot be changed, they nonethe-
stroke by 44% (Pϭ0.01). Recent guidelines for management
less serve as important identifiers of patients at risk of stroke,
of diabetes have been published by the American Diabetes
for whom an aggressive search for other modifiable risk
factors might be particularly important. Modifiable strokerisk factors include hypertension, cardiac disease (particularly
Lifestyle factors, including cigarette smoking, heavy use of
atrial fibrillation), diabetes, hypercholesterolemia, cigarette
alcohol, and physical inactivity, have all been associated with
smoking, excessive use of alcohol, and physical inactivity.
an increased risk of stroke.16–19 Modification of these behav-
Numerous prospective studies and clinical trials have consis-
iors can lead to a decrease in risk of stroke, which may be
tently shown a decreased risk of stroke with control of most
mediated by reductions in other stroke risk factors, such ashypertension, diabetes, hypercholesterolemia, and coronaryartery disease.
This statement was approved by the American Heart Association
Science Advisory and Coordinating Committee in July 1999. A single
Clinical trials analyzing the relationship of lipid-lowering
reprint is available by calling 800-242-8721 (US only) or writing the
strategies and stroke have yet to confirm a reduction in risk
American Heart Association, Public Information, 7272 Greenville Ave,
for patients who have already had a TIA or stroke. Data
Dallas, TX 75231-4596. Ask for reprint No. 71-0179. To purchaseadditional reprints: up to 999 copies, call 800-611-6083 (US only) or fax
addressing the impact of treatment with statins on the
413-665-2671; 1000 or more copies, call 214-706-1466, fax 214-691-
incidence of stroke are derived exclusively from trials of
6342, or e-mail [email protected]. To make photocopies for personal or
primary and secondary prevention of coronary disease. In
educational use, call the Copyright Clearance Center, 978-750-8400. (Stroke. 1999;30:2502-2511.)
these studies, stroke was either a secondary end point or a
1999 American Heart Association, Inc.
nonspecified end point determined on the basis of post hoc
Stroke is available at http://www.strokeaha.org
analyses. Meta-analyses of the lipid-lowering trials with the
2502 Albers et al Supplement to Guidelines for TIA Management 2503
new statin agents have found significant reductions in stroke
dose selection. Recent clinical trials have addressed this
risk.20 A 29% reduced risk of stroke and a 22% reduction in
overall mortality were found. Secondary prevention trialsshowed a 32% reduction in stroke risk, and primary trials
Optimal Dose of Aspirin to Prevent Stroke
demonstrated a 20% reduction. Two large trials21,22 in which
After TIA
stroke was prespecified as a secondary end point have also
Aspirin doses ranging from 25 mg 2 times per day29 to 325
shown significant reductions with pravastatin among subjects
mg 4 times per day30 have been shown to be efficacious for
with coronary artery disease and normal to only modest
prevention of stroke after TIA. Controversy continues to
elevations of cholesterol. Some clinical trials23,24 have also
surround the question of whether aspirin doses in the higher
demonstrated carotid plaque regression with statins. Although
end of this range (ie, Ն650 mg/d) offer more protection
statins have not been tested in patients with stroke or TIA,
against stroke than lower doses.31–34 Two well-executed
clinical trials in patients with cerebrovascular disease are
randomized trials directly compared different aspirin doses in
under way. TIA patients with cardiovascular risk factors and
patients with TIAs and minor ischemic stroke (1200 versus
cholesterol levels Ͼ200 mg/dL should have a complete lipid
300 mg/d35 and 283 versus 30 mg/d36) and found no statisti-
analysis (total cholesterol, LDL, HDL, and triglycerides) and
cally significant differences. Some have criticized these
most likely will benefit from cholesterol-lowering regimens
results because patients recruited into these trials were
younger and had a relatively lower risk of stroke than most
There are no data available from randomized clinical trials
TIA patients, and because modest differences favoring high-
to address the risks or benefits of postmenopausal hormone
dose aspirin were not excluded with statistical confi-
replacement therapy after a TIA. Ongoing trials, such as the
dence.31,34 Nevertheless, available data from these direct
Women’s Estrogen Stroke Trial and the Postmenopausal
comparisons in TIA patients suggest that the efficacy of
Estrogen and Progestin Intervention trial, may help provide
aspirin for prevention of stroke is similar for all doses in the
more evidence-based recommendations regarding the use of
ranges tested. Indirect comparisons and results of in vitrostudies have been marshaled to support the possible addi-
postmenopausal hormone replacement therapy. Data from
tional efficacy of high-dose aspirin,31,34 but their clinical
observational studies suggest that hormone replacement ther-
apy may be associated with a reduction in myocardial
A recently completed randomized trial, the Aspirin Carotid
infarction and death. Data suggesting an increased risk of
Endarterectomy (ACE) study, also directly compared differ-
stroke from oral contraceptive use cannot be extrapolated to
ent doses of aspirin in 2849 patients after carotid endarterec-
postmenopausal hormone replacement therapy (for which the
tomy. The rate of the event constellation of stroke, myocar-
goal is to obtain physiological levels of estrogen).
dial infarction, or death within 3 months of surgery was
Studies25,26 are continuing regarding the importance of
modestly (6.2% versus 8.4%) but significantly lower in those
other risk factors, including elevation of homocysteine, li-
assigned lower doses of aspirin (81 or 325 mg/d) versus
poprotein fractions [including lipoprotein (a)], and hyperco-
higher doses (650 or 1300 mg/d) (PϽ0.03).37 The effect on
agulable states from antiphospholipid antibodies, factor V,
stroke as a separate end point was similar: 64 versus 85
protein C, and protein S deficiencies.
(PϭNS) among those receiving lower versus higher doses,
Despite the wealth of data on the importance of stroke risk
respectively. These findings contrast with the nonrandomized
factors, control of these conditions is still inadequate because
post hoc analysis of long-term follow-up data from the North
of poor patient compliance and adherence to behavior mod-
ifications as well as decreased detection and treatment by
(NASCET),38 which suggested that high doses of aspirin
healthcare providers.27,28 Further reductions in the risk of
might be more effective than low doses. Although the
stroke among patients with TIA will require enhancements in
relevance of these findings to patients with TIA who have not
our ability to detect, modify, and treat cerebrovascular risk
had surgery is open to question, the results of the ACE study
lend support to the use of lower doses of aspirin in patientswith cerebrovascular atherosclerosis. Medical Therapy for TIAs
The gastrointestinal toxicity of aspirin is dose related, but
Antiplatelet Agents
even low-dose aspirin (ie, 50 to 75 mg/d) slightly increases
Antiplatelet agents are typically the treatment of choice for
the risk of major bleeding, particularly gastrointestinal hem-
prevention of future stroke in patients who have experienced
orrhage.39 Enteric coating reduces gastrointestinal toxicity
a TIA of presumed atherothrombotic origin. Four different
and appears to inhibit thromboxane synthetase similarly to
antiplatelet agents have shown efficacy for preventing stroke
equal doses of uncoated preparations despite altered pharma-
and/or other vascular events in patients with cerebrovascular
cokinetics and dynamics, although this has not been thor-
disease. The selection of a specific agent is typically based on
oughly studied in elderly stroke-prone patients.
interpretation of the results of randomized clinical trials that
Recently, the US Food and Drug Administration advocated
have tested these agents in populations of patients who have
the use of aspirin in doses of 50 to 325 mg/d for prevention
had a recent TIA or stroke. Aspirin continues to be the most
of stroke. There appears to be an emerging consensus in
economical and frequently chosen antiplatelet agent for
North America, irrespective of specialty, favoring the use of
treatment of patients after a TIA. The greatest controversy
aspirin 325 mg/d for prevention of stroke.40 For those unable
regarding the use of aspirin for stroke prevention involves
to tolerate aspirin 325 mg/d because of minor dyspepsia, the
2504 Stroke November 1999
options include taking aspirin with meals, using an enteric-
ticlopidine patients; it was severe in 0.8% of patients (none of
coated formulation, or taking a lower dose. It is the view of
the patients in the aspirin group of TASS had severe neutro-
this writing group that reasonable management of patients
penia) but was reversible in all. Because severe neutropenia
with TIA includes aspirin in doses of 50 to 1300 mg/d. With
occurred within 90 days of initiation of therapy, a recommen-
respect to the lack of established benefit of higher doses
dation was made to screen for this potential side effect by
coupled with modest dose-related toxicity, the writing group
obtaining a complete blood count with differential every 2
recommends a dosage range of 50 to 325 mg of aspirin per
weeks. Since the release of this drug, reports have described
another hematologic problem, thrombotic thrombocytopenic
For patients who experience an initial or recurrent TIA
while taking aspirin (“aspirin failures”), there is no good
Although ticlopidine is efficacious in stroke prevention, its
evidence that altering the dose of aspirin instead of continu-
usefulness is limited by its side effects. Ticlopidine is
ing the original dose will reduce the risk of subsequent
typically used in patients who are intolerant to aspirin or who
stroke.41 Those who experience TIA or minor ischemic stroke
have had an ischemic event despite taking aspirin. Because
while taking aspirin appear to have a particularly high risk for
the majority of side effects occur within the first 3 months,
subsequent stroke. Most clinicians empirically replace aspirin
patients who have tolerated these early months of therapy can
with another antiplatelet agent in this circumstance. Although
such an approach seems sensible, it is not evidencebased.41–43
Clopidogrel Clopidogrel is chemically related to ticlopidine and also Alternative Antiplatelet Agents
works by inhibiting platelet aggregation induced by ADP. Apotentially better side-effect profile than that of ticlopidine
Ticlopidine
generated interest in this antiplatelet agent.
Ticlopidine hydrochloride prevents platelet aggregation in-
The Clopidogrel versus Aspirin in Patients at Risk of
duced by adenosine diphosphate (ADP). It is approved in theUnited States for prevention of stroke in patients with TIA or
Ischemic Events (CAPRIE) trial47 assessed the relative effi-
minor stroke. Two large, multicenter, randomized trials have
cacy of clopidogrel and aspirin in reducing the risk of a
evaluated the efficacy of ticlopidine in patients with cerebro-
composite outcome cluster of ischemic stroke, myocardial
infarction, or vascular death. Stroke by itself was not a
The Canadian American Ticlopidine Study (CATS)44 as-
prespecified end point in this trial. A 75 mg/d dose of
sessed the efficacy of ticlopidine in patients who had a recent
clopidogrel was compared with a 325 mg/d dose of aspirin in
moderate to severe atherothrombotic (74%) or lacunar (26%)
patients with recent ischemic stroke or myocardial infarction
stroke for reducing the incidence of important vascular
or patients who had symptomatic atherosclerotic peripheral
events: stroke, myocardial infarction, or vascular death.
arterial disease. Patients in the stroke subgroup had had a
Patients with strokes occurring from 1 week to 4 months
stroke within 6 months of randomization and exhibited
earlier were randomized to 250 mg of ticlopidine 2 times per
persistent neurological signs for Ն1 week. TIA patients were
day or placebo. A total of 1053 patients at 25 centers in
not eligible for this study. In the entire group of 19 185
Canada and the United States were enrolled in the study.
patients enrolled in the study, intention-to-treat analysis
According to an intention-to-treat analysis, the relative risk
showed a statistically significant but quite small relative risk
reduction for the cluster of important vascular events was
reduction of 8.7% for the event cluster in favor of clopidogrel.
For the 6431 patients in the stroke subgroup, the relative risk
In the Ticlopidine Aspirin Stroke Study (TASS),45 the
reduction was a nonsignificant 7.3% in favor of clopidogrel
efficacy of ticlopidine was compared with aspirin in reducing
(Pϭ0.26). The majority of these stroke subgroup patients
the incidence of stroke and death from all causes in 3069
developed a stroke as their first outcome event.
patients with a recent TIA (50%), reversible ischemic neuro-
The safety profile of the drug appeared to be at least as
logical deficit (12%), minor stroke (23%), or Ͼ1 of these
good as that of aspirin. Although diarrhea and rash occurred
events (15%). Patients with ischemic symptoms that occurred
more commonly in the clopidogrel group than in the aspirin
within 3 months of randomization were assigned to receive
group, gastrointestinal distress and hemorrhage were reported
either 250 mg of ticlopidine twice a day or 650 mg of aspirin
more often in the aspirin cohort. Because the clopidogrel-
twice a day. According to an intention-to-treat analysis, the
treated patients showed no excess myelotoxicity, routine
overall risk reduction of fatal and nonfatal stroke by ticlopi-
blood count monitoring is not recommended as it is for
dine at 3 years was 21%. Ticlopidine also reduced the risk of
stroke and all causes of death by 12% compared with aspirin.
Although clopidogrel had a slightly greater efficacy than
In a subgroup analysis of the TASS study, ticlopidine was
aspirin in reducing the combined end point of myocardial
noted to be particularly effective in patients who had been
infarction, stroke, and vascular death in patients with athero-
taking aspirin or anticoagulant therapy at the time of their
sclerotic vascular diseases, the absolute benefit was small
(0.5% absolute annual risk reduction), and there was no
Diarrhea was the most frequent side effect of ticlopidine,
significant benefit in patients with a recent stroke. Compared
occurring in 12.5% of patients. Neutropenia was more com-
with aspirin, clopidogrel had a smaller relative risk reduction
mon in the ticlopidine groups in the TASS and CATS studies
for stroke than ticlopidine. No direct comparisons between
than in the comparison groups and occurred in 2.4% of all
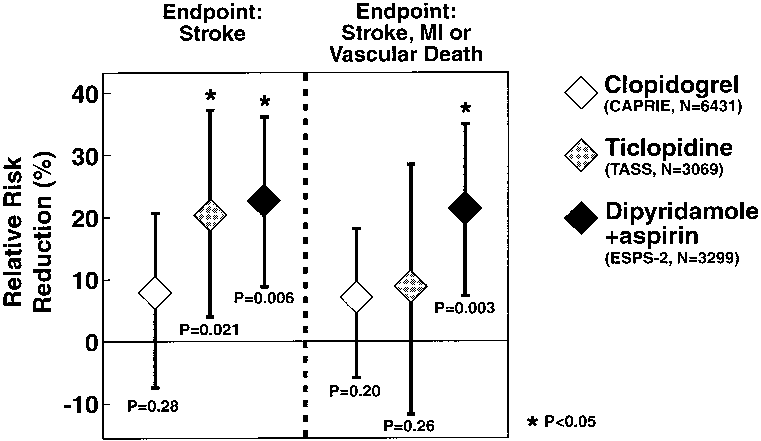
clopidogrel and ticlopidine are available (see Figure 1). Albers et al Supplement to Guidelines for TIA Management 2505
A second European Stroke Prevention Study (ESPS-2)29
was designed to ascertain the efficacy of aspirin and anextended-release formulation of dipyridamole for preventionof stroke or death and to determine whether the combinationof the 2 agents was superior to each agent given alone. ESPS-2 was larger than previous trials investigating thedipyridamole and aspirin combination; it included 6602patients with stroke (76.3%) or TIA (23.7%) within 3 monthsof enrollment. The study had a 2ϫ2 factorial design, whichallowed comparisons between 4 treatment groups: aspirin 25
Figure 1. Comparison of the efficacy of alternative antiplatelet
mg BID; extended-release dipyridamole 200 mg BID; the
agents with aspirin in patients with cerebrovascular disease:
combination of aspirin 25 mg BID and extended-release
major outcome events (relative risk reductions and 95% confi-dence intervals) in 3 large trials that compared an alternative
dipyridamole 200 mg BID; and matched placebo. Com-
antiplatelet agent with aspirin therapy alone. These data suggest
pared with placebo, stroke risk was significantly reduced by
that each of the 3 alternative agents is more effective than aspi-
18% with aspirin alone, 16% with dipyridamole alone, and
rin alone for prevention of major vascular events. Data fromESPS-2 for the combined vascular end point reflect stroke
37% with combination therapy. The risk of the combination
and/or MI and/or sudden death. Data taken from: Albers GW,
of stroke or death was also reduced by each active treatment,
Easton JD, Sacco RL, Teal P. Antithrombotic and thrombolytic
although no effect was seen on death alone. When combina-
therapy for ischemic stroke. Chest. 1998;114:683S– 698S.
tion therapy with aspirin and dipyridamole was comparedwith aspirin alone, there was a statistically significant 23.1%
However, clopidogrel clearly has an advantage over ticlopi-
reduction in stroke risk, whereas combination therapy com-
dine in its side-effect profile. Clopidogrel offers another
pared with dipyridamole alone reduced stroke risk by 24.7%.
alternative to aspirin that is particularly useful for patients
Nearly twice as many events were avoided with combination
with intolerance to aspirin. It is also likely to be useful for
therapy as with aspirin or dipyridamole alone. The narrow
patients who have an ischemic event despite aspirin therapy.
confidence interval of the ESPS-2 trial overlapped the wide
Dipyridamole and Aspirin
confidence intervals of the earlier, smaller trials, which was
The combination of aspirin, a cyclo-oxygenase inhibitor, and
compatible with a consistent beneficial treatment effect of the
dipyridamole, a cyclic nucleotide phosphodiesterase inhibi-
dipyridamole and aspirin combination.
tor, theoretically offers a pharmacological advantage over
The most common side effects of extended-release dipyr-
each of these agents alone. This combination was evaluated in
idamole-containing preparations were headache and gastro-
5 trials of cerebral ischemia, 4 of which included a compar-
intestinal events. The aspirin-containing regimens produced
ison with aspirin. The first 3 trials were relatively small. The
more frequent and severe bleeding episodes.
French Toulouse Study enrolled 440 patients with TIAs.48
In comparison with aspirin, reductions in stroke risk with
There was no statistically significant difference in outcome
the combination therapy of extended-release dipyridamole
measures among groups receiving aspirin 900 mg/d, aspirin
and aspirin were greater than those reported for clopidogrel
plus dihydroergotamine, aspirin plus dipyridamole and dihy-
(see Figure 1); however, these agents have not been compared
droergotamine, or dihydroergotamine alone. A study by
directly. The aspirin and extended-release dipyridamole com-
Bousser et al,49 the Accidents Ischemiques Cerebraux Lies a
bination was well tolerated and provides another useful
l’Atherosclerose (AICLA) study, included 604 patients with
alternative to aspirin for prevention of stroke. Combinations
TIAs (16%) or small strokes (84%). Patients were randomly
of aspirin and ticlopidine or clopidogrel have not been tested
assigned to receive aspirin 1000 mg/d, aspirin combined with
in TIA or stroke patients. Therefore, the efficacy and safety of
dipyridamole 225 mg/d, or placebo. There was a 42%
these combinations in patients at risk of stroke are unknown.
reduction in risk of stroke with aspirin compared withplacebo. No added benefit was derived with dipyridamole. In
Anticoagulants
the American-Canadian Cooperative Study,50 890 patients
Cardioembolic Stroke
with carotid-distribution TIAs were evaluated. Brain or reti-
Adjusted-dose oral anticoagulation with warfarin continues to
nal infarction occurred in 60 (14%) of 442 patients taking
be the therapy of choice for stroke prevention in patients with
aspirin and in 53 (12%) of 448 patients taking aspirin plus
atrial fibrillation who have had a TIA. The superior efficacy
dipyridamole, which was not a significant difference.
of anticoagulation over aspirin for prevention of stroke in
The European Stroke Prevention Study (ESPS)51 compared
patients with atrial fibrillation and a recent TIA or minor
placebo with aspirin 975 mg/d plus dipyridamole 225 mg/d in
stroke was shown in the European Atrial Fibrillation Trial.52
2500 patients with TIAs (33%), reversible ischemic neuro-
In addition, considerable data from multiple randomized trials
logical deficits (7%), or stroke (60%). Because no patients
have shown that oral anticoagulation is the treatment of
were given aspirin alone, this study did not permit compari-
choice for primary stroke prevention in high-risk atrial
son of the combination with aspirin therapy. However, there
fibrillation patients. Patients with atrial fibrillation who are at
was an overall reduction of 33% in the risk of stroke and
high risk of stroke include persons with a history of hyper-
death and a reduction of 38% in the risk of stroke alone for
tension, poor left ventricular function, rheumatic mitral valve
those assigned to the combination treatment compared with
disease, prosthetic heart valves, a prior stroke, TIA, systemic
2506 Stroke November 1999
The efficacy of aspirin for prevention of cardioembolic
study). Some experts also recommend anticoagulation ther-
stroke is considerably less than warfarin. Aspirin is recom-
apy for patients who experienced a TIA while taking an
mended for patients at high risk of cardioembolism who have
antiplatelet agent or for persons with crescendo TIAs. Some
contraindications to oral anticoagulation. Anticoagulant ther-
clinicians use short-term anticoagulation after a TIA while an
apy is appropriate for patients with several other high-risk
urgent evaluation is being performed. No adequate data are
sources of cardiogenic emboli who have a TIA; however,
available to support or refute this practice. TIA patients with
randomized clinical trials have not been performed in these
extracranial cervical artery dissections, severe carotid steno-
specific patient populations. These high-risk sources for
sis before endarterectomy, antiphospholipid antibody syn-
recurrent cardiac embolization include mechanical prosthetic
drome, or cerebral venous sinus thrombosis may respond
heart valves, recent myocardial infarction, left ventricular
favorably to anticoagulation therapy; however, randomized
thrombus, dilated cardiomyopathies, and marantic endocardi-
clinical trial data are not available for these specific disorders.
tis. The role of anticoagulation for patients with TIA whohave a patent foramen ovale or an atrial septal aneurysm is
Surgical Management
not clear. An ongoing study is comparing the efficacy of
Carotid Artery Disease
aspirin with oral anticoagulation in patients with patent
Atherosclerotic narrowing of the internal carotid artery at the
foramen ovale who suffered a recent cryptogenic stroke.
carotid bifurcation in the neck is a common cause of TIA and
Mitral valve prolapse, a common valvular abnormality, was
stroke. During the late 1980s and 1990s, the value of carotid
formerly thought to cause stroke, but more recent population-
endarterectomy for stroke prevention was assessed by pro-
based and case-control studies have not demonstrated an
spective randomized trials. Three major prospective random-
ized trials—NASCET, the European Carotid Surgery Trial(ECST), and the Veterans Affairs Cooperative Study Program
Optimal Intensity of Anticoagulation Recent studies have addressed the optimal intensity of oral
309 (VACSP 309)— evaluated the efficacy of carotid endar-
anticoagulation for prevention of stroke in patients with atrial
terectomy in symptomatic patients (patients with TIAs or
fibrillation. Results from a large case-control study56 and 2
small strokes) with high-grade carotid stenosis. The results of
randomized clinical trials52,57 suggest that the efficacy of oral
these trials were reported in 1991 and showed a clear benefit
anticoagulation declines significantly below an International
of carotid endarterectomy.62–64 Endarterectomy was not ben-
Normalized Ratio (INR) of 2.0. Recent surveys indicate that
eficial for patients with mild stenosis (Ͻ30%) in the ECST.63
a high percentage of atrial fibrillation patients who are taking
Recent Results for Moderate Carotid Stenosis
warfarin have subtherapeutic levels of anticoagulation.58
The results of NASCET and ECST, which compared surgical
Current recommendations suggest a target INR of 2.5 (range
and medical therapy in patients with recently symptomatic
2.0 to 3.0) for most indications for oral anticoagulation.59
moderate carotid stenosis, were reported in 1998.39,65 The
Anticoagulation for Atherothrombotic Stroke
long-term (up to 8 years) outcome in patients with high-grade
The relative efficacy of oral anticoagulation compared with
stenosis who were entered in the trials was also reported.
antiplatelet therapy has not been adequately studied in pa-
NASCET reported the results for symptomatic patients
tients with atherothrombotic stroke or TIA. At present, the
with moderate carotid stenosis who were randomly assigned
only large randomized trial available compared very-high-
to receive medical care (1108 patients) or surgery (1118
intensity oral anticoagulation (INR 3.0 to 4.5) with aspirin
patients). Entry criteria included moderate carotid stenosis
(30 mg/d) in patients with a recent TIA or minor stroke.60
and a nondisabling stroke or TIA referable to the stenosis
This study was terminated prematurely because of a high rate
within 180 days. Patients were stratified into 2 groups (either
of major hemorrhage in the anticoagulation group. These
a 50% to 69% or 30% to 49% stenosis of the internal carotid
results demonstrate that an INR range of 3.0 to 4.5 is not safe
artery measured angiographically). Average follow-up was 5
for patients with a recent TIA or atherothrombotic stroke. The
years, and primary outcome measures were fatal or nonfatal
Warfarin Aspirin Recurrent Stroke Study is a large ongoing
stroke ipsilateral to carotid stenosis. For patients with 50% to
trial comparing a lower target INR (1.4 to 2.8) with aspirin
69% stenosis, the rate of ipsilateral stroke over the 5-year
(325 mg/d) in patients with a recent atherothrombotic stroke.
period was 22.2% in the medically treated group and 15.7%
A European study (European and Australian Stroke Preven-
in the surgically treated group (6.5% absolute risk reduction
tion in Reversible Ischemia Trial) is also comparing the
over 5 years, Pϭ0.045).39 In patients with Ͻ50% stenosis, the
efficacy of oral anticoagulation with antiplatelet therapy for
ipsilateral stroke rate was slightly lower (14.9%) in those
secondary stroke prevention. The results of these trials are
treated with endarterectomy than in those who were medi-
expected to significantly clarify the role of oral anticoagula-
cally treated (18.7%), but this was not significantly different
tion after a noncardioembolic cerebral ischemic event.
(Pϭ0.16). The benefit achieved by surgery was greatest
It is possible that specific atherothrombotic stroke subtypes
among men, in patients with recent stroke (rather than TIA)
may respond favorably to oral anticoagulation. For example,
as the qualifying event, and in patients with hemispheric
a nonrandomized retrospective study61 found that patients
with symptomatic intracranial stenosis had a lower stroke rate
The final results of ECST were also reported in 1998.65
when they took warfarin rather than aspirin. A randomized
This report contained long-term follow-up data on patients
trial based on these preliminary results is currently under way
with a moderate degree of stenosis randomly assigned to
(the Warfarin-Aspirin Symptomatic Intracranial Disease
surgery or medical treatment as well as additional follow-up
Albers et al Supplement to Guidelines for TIA Management 2507
symptomatic patients with Ͼ70% stenosis as measured by theNASCET method can expect a far greater benefit fromcarotid endarterectomy. Surgical benefits appear to be partic-ularly robust for men, patients with hemispheric symptomsand without diabetes, and for persons with significant ulcersas demonstrated by angiography. The benefit of carotidendarterectomy is highly dependent on surgical risk. NASCET had strict criteria for qualifying surgeons and usedongoing quality assessments to ensure acceptable levels ofperioperative complications. Angioplasty and Stent Placement Transluminal angioplasty with intravascular placement of Figure 2. Differences in measurement techniques used by NASCET and ECST. Comparisons of differences in stenosis
stents for treatment of carotid stenosis is currently being
severity by the 2 methods are also illustrated. Reprinted with
evaluated as an alternative to carotid endarterectomy. Some
permission from: Donnan GA, Davis SM, Chambers BR, Gates
initial case series have reported relatively low complication
PC. Commentary: surgery for prevention of stroke. Lancet. 1998;351:1372–1373.
rates, and some investigators advocate this method of treat-ment for patients who are at high risk for surgery because of
in patients with severe carotid stenosis and mild carotid
heart disease or other comorbid factors. However, other
stenosis. This multicenter, prospective, randomized, con-
recent reports have suggested that the complication rate from
trolled trial enrolled a total of 3024 patients. Entry criteria
this procedure may be higher than initially reported.68 Early
included Ն1 transient or mild symptomatic ischemic vascular
results have demonstrated high rates of restoration of the
event in the distribution of a carotid artery with some degree
luminal diameter in the internal carotid artery.69 Case series
have included patients with asymptomatic as well as symp-
Like the results of NASCET, the results of ECST revealed
tomatic carotid stenosis and mixtures of patients with various
that surgery was most effective in patients with more severe
degrees of comorbidity. The long-term effects of stenting and
degrees of carotid stenosis. In the entire group (all degrees of
rate of restenosis are unknown. Prospective randomized trials
stenosis), 669 (37%) of the patients in the surgery group and
comparing angioplasty and stenting with carotid endarterec-
440 (36.5%) of the patients in the control group sustained a
tomy are ongoing.70,71 Until the results of these studies are
major stroke or death (not significantly different). There was
available, this procedure should be considered investiga-
a 7% chance of major stroke or death complicating surgery.
tional. Recent case series have also provided preliminary data
The risk of major ischemic strokes was much higher ipsilat-
regarding the safety and efficacy of angioplasty for treatment
eral to an unoperated symptomatic carotid artery with a
of symptomatic intracranial stenosis.72,73 A high degree of
stenosis Ͼ80% for 2 to 3 years after randomization. The
technical success and low complication rates have been
long-term risk of major stroke or death in medically treated
patients with carotid stenosis Ͼ80% of the original lumendiameter at 3 years was 26.5% versus 14.9% in the surgically
Extracranial-Intracranial Bypass
treated group for an absolute benefit of 11.6% over 3 years
Extracranial-intracranial bypass is a procedure designed to
(Pϭ0.001). As in the NASCET findings, women benefited
improve blood flow to the brain by direct vascular conduits
from the external carotid circulation to the intracranial circu-
It is important to consider that the degree of carotid
lation.74 The effects of superficial temporal to middle cerebral
stenosis in ECST was measured differently than that in
artery bypass were evaluated for patients with TIAs or mild
NASCET.66,67 The degree of carotid stenosis is significantly
strokes in a large, prospective, randomized trial funded by the
higher if calculated by the NASCET rather than the ECST
National Institutes of Health and conducted in 71 North
method66 (see Figure 2). Stroke rates in medically treated
American, European, and Asian centers.75 Entry criteria
patients with carotid stenosis increase dramatically with
included recent cerebral ischemic symptoms combined with
stenosis Ͼ80% as measured by the ECST method. This
carotid occlusion, carotid artery narrowing distal to the
corresponds roughly to a 60% stenosis measured by the
carotid bifurcation, or intracranial stenosis. Although a high
patency rate of the bypass was demonstrated, the study found
In summary, it appears that patients with a recent TIA or
that superficial temporal artery–middle cerebral artery bypass
nondisabling stroke with ipsilateral carotid stenosis benefit
had no advantage over medical therapy.
from surgery if the stenosis is Ͼ50% as measured by the
Because this trial included patients without hemodynamic
NASCET method; however, this benefit appears to be less
insufficiency, it is possible that patients selected on a hemo-
pronounced in women. Sex and age differences, as well as
dynamic basis may benefit from the procedure.76–79 New
comorbidity, must be considered when treatment options are
imaging techniques such as positron emission tomography,
evaluated in patients with stenosis of 50% to 69%, because
xenon computed tomography, and transcranial Doppler with
the absolute benefit of surgery is relatively small for these
vasoreactivity testing have been shown to identify patients
patients. Women or patients with retinal TIAs with carotid
with extracranial occlusive disease who are at high risk for
stenosis Ͻ70% may not benefit from surgery. Recently
subsequent stroke.80–82 Randomized clinical trials will be
2508 Stroke November 1999 Use of Antithrombotic Agents in Patients With TIAs
TIA (atherothrombotic) and aspirin-intolerant* or if
ASA 50–325 mg/d (if contraindications to warfarin)
ASA indicates acetylsalicylic acid (aspirin); ER-DP, extended-release dipyridamole. *Neither ER-DPϩASA or ASA alone is recommended for patients who are allergic to aspirin or unable to take low-dose aspirin. †The recommended antithrombotic agents have not been specifically tested in patients who have experienced a TIA during ASA therapy.
required to establish whether extracranial-intracranial bypass
2. Cigarette smoking should be discontinued. Counseling,
surgery can benefit a specific subgroup of patients. Patients
nicotine replacement therapies, bupropion, and formal
with moyamoya disease who have had TIAs or recent strokes
smoking cessation programs may all be helpful.
may benefit from extracranial-intracranial bypass or encepha-
3. Coronary artery disease, cardiac arrhythmias, conges-
tive heart failure, and valvular heart disease should be
lodural synangiosis procedures; however, results of well-
controlled trials are not available.83–86
4. Excessive use of alcohol should be eliminated. Formal
alcohol cessation programs are recommended. Mild to
Surgery for Vertebrobasilar Disease
moderate use of alcohol (1 to 2 drinks per day) has been
TIAs referable to the posterior circulation can result from
associated with a reduction in stroke rates.
occlusive disease of the vertebrobasilar system. The 2 most
5. Treatment of hyperlipidemia is recommended. The
common sites for vertebral artery atheroma are the origin of the
AHA Step II diet (Յ30% of calories derived from fat,
vertebral artery and slightly distal to the transition from the
Ͻ7% from saturated fat, and Ͻ200 mg/d cholesterol
extracranial to the intracranial portion.87–89 Surgical and endo-
consumed) is recommended along with maintenance ofideal body weight and engagement in regular physical
vascular treatments have been performed for patients with TIAs
activity. If lipid levels remain elevated (LDL Ͼ130
or small strokes referable to atheromatous disease of the verte-
mg/dL), use of a lipid-lowering agent, preferably a
brobasilar system.90–92 Small case series have reported favorable
statin, is recommended. The goal of therapy should be
results. Vertebral artery transposition to the common carotid
artery is increasingly used for vertebral origin stenosis.87,92–95
6. Fasting blood glucose levels Ͻ126 mg/dL are recom-
Angioplasty can also be performed at this site. Either direct
mended. Diet and oral hypoglycemics or insulin should
endarterectomy or angioplasty with or without stenting has also
be prescribed as needed to control diabetes.
been performed for patients with symptomatic intracranial ver-
7. Physical activity (30 to 60 minutes of exercise Ն3 to 4
tebral artery stenosis.88,90,96 For mid-vertebral lesions with fixed
8. Discontinuation of postmenopausal estrogen replace-
stenosis or positional obstruction with ischemic symptoms,
surgical reconstruction or decompression can be effective inrelieving symptoms.92,97 Bypass procedures have also been used
Medical Therapy (Table)
in patients with vertebrobasilar ischemia.91 Comparisons ofsurgery and endovascular therapy are lacking, and there are no
Atherothrombotic TIAs Patients who have had an atherothrombotic TIA should
randomized controlled trials comparing these procedures with
receive daily therapy with an antiplatelet agent to reduce the
risk of recurrent stroke (grade A-1). Aspirin, clopidogrel,ticlopidine, and the combination of aspirin and extended-
Recommendations
release dipyridamole are all acceptable options for initial
Risk Factor Management
Risk factor guidelines are grade C because randomized trials
In general, aspirin at a dosage range of 50 to 325 mg/d is
have not been completed in TIA patients.
recommended as initial therapy for patients who are not allergicor intolerant to aspirin. For patients who have an atherothrom-
1. After thorough evaluation to determine the cause of the
botic TIA while taking aspirin, there is no compelling evidence
TIA, hypertension should be treated to maintain systolic
that increasing the dose of aspirin provides additional benefit.
blood pressure below 140 mm Hg and diastolic blood
Alternative antiplatelet agents are typically considered for these
pressure below 90 mm Hg. For persons with diabetes,
patients, although they have not been specifically evaluated in
blood pressure levels Ͻ130/85 mm Hg are recommended.
patients who have “failed aspirin.” Although ticlopidine may be
Albers et al Supplement to Guidelines for TIA Management 2509
more effective for preventing stroke (on the basis of indirect
Bypass Surgery
comparisons), clopidogrel (75 mg/d) is generally recommended
Extracranial-intracranial bypass is not recommended for patients
in favor of ticlopidine (250 mg BID) (grade C-2) because of its
with TIAs (grade A-1). A subgroup of patients with anterior
superior safety profile. The combination of extended-release
circulation ischemia unresponsive to medical therapy with he-
dipyridamole and aspirin may also be more effective than
modynamic disturbances may benefit from bypass surgery.
clopidogrel (on the basis of indirect comparisons; grade C-2),
Additional studies are required to determine the role of surgery
and both have a favorable safety profile.
in these patients. Patients with moyamoya disease may benefit
Anticoagulant therapy is not routinely recommended for
from extracranial-intracranial bypass (grade C-2).
patients with atherothrombotic TIAs, as either short- or
Therapy for Vertebrobasilar Ischemia
long-term therapy (grade B-2). Anticoagulant therapy is an
Surgical or endovascular therapy may be appropriate for
option for patients with a TIA who continue to have symp-
patients with significant vertebrobasilar stenosis who have
toms despite antiplatelet therapy (grade C-2). At anticoagu-
continued symptoms referable to the posterior circulation
lation intensities of INR 3.0 to 4.5, the risk of brain hemor-
despite medical therapy. For significant stenosis at the origin
rhage outweighs the potential benefits (grade A-1).
of the vertebral artery, vertebral artery transposition to the
Therefore, if oral anticoagulants are used for atherothrom-
common carotid artery or angioplasty and stenting are treat-
botic TIA patients, a target INR Ͻ3.0 should be chosen.
ment options (grade C-2). For significant stenosis at the distal
Cardioembolic TIAs
vertebral artery, endarterectomy, bypass, or endovascular
Long-term oral anticoagulation is recommended for patients
procedures are treatment options. For midvertebral lesions
with atrial fibrillation who have a TIA (grade A-1). For these
with fixed stenosis or positional obstruction with ischemic
patients, a target INR of 2.5 (range 2.0 to 3.0) is recom-
symptoms, surgical reconstruction or decompression can be
mended. Oral anticoagulation is also beneficial for prevention
effective in relieving symptoms (grade C-2).
of stroke in patients with other high-risk cardiac sources ofembolism (see section on Anticoagulants, Cardioembolic
References
Stroke). Aspirin is recommended for patients with contrain-
1. Feinberg WM, Albers GW, Barnett HJM, Biller J, Caplan LR, Carter LP,
Hart RG, Hobson RW II, Kronmal RA, Moore WS, Robertson JT, Adams
HP Jr, Mayberg M, et al. Guidelines for the management of transientischemic attacks: from the Ad Hoc Committee on Guidelines for the
Surgical Management
Management of Transient Ischemic Attacks of the Stroke Council of theAmerican Heart Association. AHA medical/scientific statement: special
Extracranial Carotid Artery Disease
report. Circulation. 1994;89:2950 –2965.
2. Guyatt GH, Cook DJ, Sackett DL, Eckman M, Pauker S. Grades of
recommendation for antithrombotic agents. Chest. 1998;114:441S– 444S.
Carotid endarterectomy is indicated for patients who are good
3. Sacco RL, Benjamin EJ, Broderick JP, Dyken M, Easton JD, Feinberg
surgical candidates and who have experienced Ն1 TIA or
WM, Goldstein LB, Gorelick PB, Howard G, Kittner SJ, Manolio TA,
minor stroke within the last 2 years, regardless of the
Whisnant JP, Wolf PA. Risk Factors Panel: American Heart AssociationPrevention Conference IV: prevention and rehabilitation of stroke: risk
response to antiplatelet drugs (grade A-1).
factors. Stroke. 1997;28:1507–1517.
4. Collins R, Peto R, MacMahon S, Hebert P, Fiebach NH, Eberlein KA,
Godwin J, Qizilbash N, Taylor JO, Hennekens CH. Blood pressure,
Patients with a recent TIA or minor stroke have a reduced
stroke, and coronary heart disease, part 2: short-term reductions in blood
stroke rate with endarterectomy versus medical treatment and
pressure: overview of randomised drug trials in their epidemiological
should be considered for endarterectomy (grade A-1). The
context. Lancet. 1990;335:827– 838.
5. SHEP Cooperative Research Group. Prevention of stroke by antihyper-
absolute benefit of surgery is less than that for patients with
tensive drug treatment in older persons with isolated systolic hyper-
higher degrees of stenosis and among women and patients
tension: final results of the Systolic Hypertension in the Elderly Program
with retinal TIAs. Consideration should be given to clinical
(SHEP). JAMA. 1991;265:3255–3264.
features that influence stroke risk and surgical morbidity.
6. Staessen JA, Fagard R, Thijs L, Celis H, Arabidze GG, Birkenhager WH,
Bulpitt CJ, de Leeuw PW, Dollery CT, Fletcher AE, Forette F, Leonetti
G, Nachev C, O’Brien ET, Rosenfeld J, Rodicio JL, Tuomilehto J,Zanchetti A. Randomised double-blind comparison of placebo and active
Patients with Ͻ50% stenosis with recent symptoms of cere-
treatment for older patients with isolated systolic hypertension: the Sys-
bral ischemia do not benefit from carotid endarterectomy
tolic Hypertension in Europe (Syst-Eur) Trial Investigators. Lancet. 1997;
(grade A-1). Antiplatelet therapy is recommended for these
patients (see section on Medical Therapy).
7. The sixth report of the Joint National Committee on prevention, detection,
evaluation, and treatment of high blood pressure. Arch Intern Med.
8. Wolf PA, D’Agostino RB, Belanger AJ, Kannel WB. Probability of
Prospective trials evaluating the results of angioplasty and
stroke: a risk profile from the Framingham Study. Stroke. 1991;22:
stent placement in comparison with carotid endarterectomy
are now in progress. The use of endovascular treatment is not
9. Kuller LH, Dorman JS, Wolf PA. Cerebrovascular diseases and diabetes.
routinely recommended for treatment of carotid bifurcation
In: National Diabetes Data Group, Department of Health and HumanServices, National Institutes of Health. Diabetes in America: DiabetesData Compiled for 1984. Bethesda, MD: National Institutes of Health;1985:1–18.
10. Balkau B, Shipley M, Jarrett RJ, Pyorala K, Pyorala M, Forhan A,
*Recommendations for degree of stenosis based on NASCET mea-
Eschwege E. High blood glucose concentration is a risk factor for mor-
surements (see text and Figure 2 for details).
tality in middle-aged nondiabetic men: 20-year follow-up in the Whitehall
2510 Stroke November 1999
Study, the Paris Prospective Study, and the Helsinki Policemen Study.
33. Patrono C, Roth GJ. Aspirin in ischemic cerebrovascular disease: how
Diabetes Care. 1998;21:360 –367.
strong is the case for a different dosing regime? Stroke. 1996;27:
11. Effect of intensive diabetes management on macrovascular events and
risk factors in the Diabetes Control and Complications Trial. Am J
34. Barnett HJM, Kaste M, Meldrum H, Eliasziw M. Aspirin dose and stroke
prevention: beautiful hypotheses slain by ugly facts. Stroke. 1996;27:
12. UK Prospective Diabetes Study Group. Intensive blood-glucose control
with sulphonylureas or insulin compared with conventional treatment and
35. Farrell B, Godwin J, Richards S, Warlow C. The United Kingdom
risk of complications in patients with type 2 diabetes: UKPDS 33. Lancet.
Transient Ischemic Attack (UK-TIA) aspirin trial: final results. J NeurolNeurosurg Psychiatry. 1991;54:1044 –1054.
13. UK Prospective Diabetes Study Group. Tight blood pressure control and
36. The Dutch TIA Trial Study Group. A comparison of two doses of aspirin
risk of macrovascular and microvascular complications in type 2 diabetes:
(30 mg vs 283 mg a day) in patients after a transient ischemic attack or
UKPDS 38. BMJ. 1998;317:703–713.
minor ischemic stroke. N Engl J Med. 1991;325:1261–1266.
14. The Diabetes Control and Complications Trial Research Group. The
37. Taylor DW, Barnett HJM, Haynes RB, Ferguson GG, Sackett DL, Thorpe
effect of intensive treatment of diabetes on the development and pro-
KE, Simard D, Silver FL, Hachinski V, Clagett GP, Barnes R, Spence JD,for the ASA and Carotid Endarterectomy (ACE) Trial Collaborators.
gression of long-term complications in insulin-dependent diabetes
Low-dose and high-dose acetylsalicylic acid for patients undergoing
mellitus. N Engl J Med. 1993;329:977–986.
carotid endarterectomy: a randomised controlled trial. Lancet. 1999;353:
15. American Diabetes Association. Clinical practice recommendations 1998. Diabetes Care. 1998;21(suppl 1):S1–S89.
38. Barnett HJ, Taylor DW, Eliasziw M, Fox AJ, Ferguson GG, Haynes RB,
16. Sacco RL, Gan R, Boden-Albala B, Lin IF, Kargman DE, Hauser WA,
Rankin RN, Clagett GP, Hachinski VC, Sackett DL, Thorpe KE,
Shea S, Paik M. Leisure-time physical activity and ischemic stroke risk:
Meldrum HE. Benefit of carotid endarterectomy in patients with symp-
the Northern Manhattan Stroke Study. Stroke. 1998;29:380 –387.
tomatic moderate or severe stenosis: North American Symptomatic
17. Lee IM, Hennekens CH, Berger K, Buring JE, Manson JE. Exercise and
Carotid Endarterectomy Trial Collaborators. N Engl J Med. 1998;339:
risk of stroke in male physicians. Stroke. 1999;30:1– 6.
18. Truelsen T, Gronbaek M, Schnohr P, Boysen G. Intake of beer, wine, and
39. Hansson L, Zanchetti A, Carruthers SG, Dahlof B, Elmfeldt D, Julius S,
spirits and risk of stroke: the Copenhagen City Heart Study. Stroke.
Menard J, Rahn KH, Wedel H, Westerling S. Effects of intensive blood-
pressure lowering and low-dose aspirin in patients with hypertension:
19. Sacco RL, Elkind M, Boden-Albala B, Lin I-F, Kargman DE, Hauser
principal results of the Hypertension Optimal Treatment (HOT) ran-
WA, Shea S, Paik MC. The protective effect of moderate alcohol con-
domised trial: HOT Study Group. Lancet. 1998;351:1755–1762.
sumption on ischemic stroke. JAMA. 1999;281:53– 60.
40. Goldstein LB, Bonito AJ, Matchar DB, Duncan PW, DeFriese GH,
20. Hebert PR, Gaziano JM, Chan KS, Hennekens CH. Cholesterol lowering
Oddone EZ, Paul JE, Akin DR, Samsa GP. US national survey of
with statin drugs, risk of stroke, and total mortality: an overview of
physician practices for the secondary and tertiary prevention of ischemic
randomized trials. JAMA. 1997;278:313–321.
stroke: design, service availability, and common practices. Stroke. 1995;
21. Sacks FM, Pfeffer MA, Moye LA, Rouleau JL, Rutherford JD, Cole TG,
Brown L, Warnica JW, Arnold JM, Wun CC, Davis BR, Braunwald E.
41. Dyken ML. Aspirin dose in secondary prevention of stroke. Cerebrovasc
The effect of pravastatin on coronary events after myocardial infarction in
Dis. 1998;8:361–362. Letter.
patients with average cholesterol levels: Cholesterol and Recurrent
42. Grotta JC, Norris JW, Kamm B. Prevention of stroke with ticlopidine:
Events Trial investigators. N Engl J Med. 1996;335:1001–1009.
who benefits most? TASS Baseline and Angiographic Data Subgroup.
22. The Long-Term Intervention with Pravastatin in Ischaemic Disease
Neurology. 1992;42:111–115.
(LIPID) Study Group. Prevention of cardiovascular events and death with
43. Rothrock JF, Hart RG. Ticlopidine hydrochloride use and threatened
pravastatin in patients with coronary heart disease and a broad range of
stroke. West J Med. 1994;160:43– 47.
initial cholesterol levels. N Engl J Med. 1998;339:1349 –1357.
44. Gent M, Blakely JA, Easton JD, Ellis DJ, Hachinski VC, Harbison JW,
23. Furberg CD, Adams HP, Applegate WB, Byington RP, Espeland MA,
Panak E, Roberts RS, Sicurella J, Turpie AG. The Canadian American
Hartwell T, Hunninghake DB, Lefkowitz DS, Probstfield J, Riley WA,
Ticlopidine Study (CATS) in thromboembolic stroke. Lancet. 1989;1:
Young B, for the Asymptomatic Carotid Artery Progression Study
(ACAPS) Research Group. Effect of lovastatin on early carotid athero-
45. Hass WK, Easton JD, Adams HP Jr, Pryse-Phillips W, Molony BA,
sclerosis and cardiovascular events. Circulation. 1994;90:1679 –1687.
Anderson S, Kamm B. A randomized trial comparing ticlopidine hydro-
24. Crouse JR III, Byington RP, Bond MG, Espeland MA, Craven TE,
chloride with aspirin for the prevention of stroke in high-risk patients:
Sprinkle JW, McGovern ME, Furberg CD. Pravastatin, lipids, and ath-
Ticlopidine Aspirin Stroke Study Group. N Engl J Med. 1989;321:
erosclerosis in the carotid arteries (PLAC-II). Am J Cardiol. 1995;75:
46. Bennett CL, Weinberg PD, Rozenberg-Ben-Dror K, Yarnold PR, Kwaan
HC, Green D. Thrombotic thrombocytopenic purpura associated with
25. Giles WH, Croft JB, Greenlund KJ, Ford ES, Kittner SJ. Total homocys-
ticlopidine: a review of 60 cases. Ann Intern Med. 1998;128:541–544.
t(e)ine concentration and the likelihood of nonfatal stroke: results from
47. CAPRIE Steering Committee. A randomised, blinded, trial of clopidogrel
the third National Health and Nutrition Examination Survey, 1988 –1994.
versus aspirin in patients at risk of ischaemic events (CAPRIE). Lancet.
26. Sacco RL, Roberts JK, Jacobs BS. Homocysteine as a risk factor for
48. Giraud-Chaumeil B, Rascol A, David J, Boneu B, Clanet M, Bierme R.
ischemic stroke: an epidemiological story in evolution. Neuroepidemiol-
Pre´vention des re´cidives des accidents vasculaires ce´re´braux ische´miques
par les anti-aggregants plaquettaires: re´sults d’un essai the´rapeutique
27. Joseph LN, Babikian VL, Allen NC, Winter MR. Risk factor modification
controle de 3 ans. Rev Neurol (Paris). 1982;138:367–385.
in stroke prevention: the experience of a stroke clinic. Stroke. 1999;30:
49. Bousser MG, Eschwege E, Haguenau M, Lefaucconnier JM, Thibult N,
Touboul D, Touboul PJ. AICLA controlled trial of aspirin and dipyri-
28. Gorelick PB. Stroke prevention: windows of opportunity and failed
damole in the secondary prevention of atherothrombotic cerebral ische-
expectations: a discussion of modifiable cardiovascular risk factors and a
prevention proposal. Neuroepidemiology. 1997;16:163–173.
50. The American-Canadian Co-Operative Study Group. Persantine Aspirin
29. Diener HC, Cunha L, Forbes C, Sivenius J, Smets P, Lowenthal A.
Trial in cerebral ischemia, II: end point results. Stroke. 1985;16:406 – 415.
European Stroke Prevention Study 2: dipyridamole and acetylsalicylic
51. The ESPS Group. The European Stroke Prevention Study (ESPS):
acid in the secondary prevention of stroke. J Neurol Sci. 1996;143:1–13.
principal end-points. Lancet. 1987;2:1351–1354.
30. Canadian Cooperative Study Group. A randomized trial of aspirin and
52. EAFT (European Atrial Fibrillation Trial) Study Group. Secondary pre-
sulfinpyrazone in the threatened stroke. N Engl J Med. 1978;299:53–59.
vention of vascular events in patients with nonrheumatic atrial fibrillation
31. Dyken ML, Barnett HJM, Easton JD, Fields WS, Fuster V, Hachinski V,
and a recent transient ischaemic attack or minor ischaemic stroke. Lancet.
Norris JW, Sherman DG. Low-dose aspirin and stroke: “it ain’t neces-
sarily so.” Stroke. 1992;23:1395–1399.
53. Laupaucis A, Albers GW, Dalen J, Dunn MI, Jacobson AK, Singer DE.
32. Hart RG, Harrison MJG. Aspirin wars: the optimal dose of aspirin to
Antithrombotic therapy in atrial fibrillation. Chest. 1998;114(suppl
prevent stroke. Stroke. 1996;27:585–587. Albers et al Supplement to Guidelines for TIA Management 2511
54. Petty GW, Orencia AJ, Khandheria BK, Whisnant JP. A population-based
76. Awad IA, Spetzler RF. Extracranial-intracranial bypass surgery: a critical
study of stroke in the setting of mitral valve prolapse: risk factors and
analysis in light of the International Cooperative Study. Neurosurgery.
infarct subtype classification. Mayo Clin Proc. 1994;69:632– 634.
55. Gilon D, Buonanno FS, Joffe MM, Leavitt M, Marshall JE, Kistler JP,
77. Caplan LR, Piepgras DG, Quest DO, Toole JF, Samson D, Futrell N,
Levine RA. Lack of evidence of an association between mitral-valve
Millikan C, Flamm ES, Heros RC, Yonekawa Y, Eguchi T, Yonas H,
prolapse and stroke in young patients. N Engl J Med. 1999:341:8 –13.
Rothbart D, Spetzler RF. EC-IC bypass 10 years later: is it valuable? Surg
56. Hylek EM, Skates SJ, Sheehan MA, Singer DE. An analysis of the lowest
effective intensity of prophylactic anticoagulation for patients with non-
78. McCormick PW, Tomecek FJ, McKinney J, Ausman JI. Disabling
rheumatic atrial fibrillation. N Engl J Med. 1996;335:540 –546.
cerebral transient ischemic attacks. J Neurosurg. 1991;75:891–901.
57. Stroke Prevention in Atrial Fibrillation Investigators. Adjusted-dose
79. Schmiedek P, Piepgras A, Leinsinger G, Kirsch C, Einhupl K.
warfarin versus low-intensity, fixed-dose warfarin plus aspirin for
Improvement of cerebrovascular reserve capacity by EC-IC arterial
high-risk patients with atrial fibrillation: Stroke Prevention in Atrial
bypass surgery in patients with ICA occlusion and hemodynamic cerebral
Fibrillation III randomised clinical trial. Lancet. 1996;348:633– 638.
ischemia. J Neurosurg. 1994;81:236 –244.
58. Albers GW, Yim JM, Belew KM, Bittar N, Hattemer CR, Phillips BG,
80. Grubb RL Jr, Derdeyn CP, Fritsch SM, Carpenter DA, Yundt KD, Videen
Kemp S, Hall EA, Morton DJ, Vlasses PH. Status of antithrombotic
TO, Spitznagel EL, Powers WJ. Importance of hemodynamic factors in
therapy for patients with atrial fibrillation in university hospitals. Arch
the prognosis of symptomatic carotid occlusion. JAMA. 1998;280:
Intern Med. 1996;156:2311–2316.
59. Hirsh J, Dalen JE, Anderson DR, Poller L, Bussey H, Ansell J, Deykin D,
81. Kleiser B, Widder B. Course of carotid artery occlusions with impaired
Brandt JT. Oral anticoagulants: mechanism of action, clinical effec-
cerebrovascular reactivity. Stroke. 1992;23:171–174.
tiveness, and optimal therapeutic range. Chest. 1998;114(5 suppl):
82. Yonas H, Smith HA, Durham SR, Pentheny SL, Johnson DW. Increased
stroke risk predicted by compromised cerebral blood flow reactivity.
60. The Stroke Prevention in Reversible Ischemia Trial (SPIRIT) Study
J Neurosurg. 1993;79:483– 489.
Group. A randomized trial of anticoagulants versus aspirin after cerebral
83. Chiu D, Shedden P, Bratina P, Grotta JC. Clinical features of moyamoya
ischemia of presumed arterial origin. Ann Neurol. 1997;42:857– 865.
disease in the United States. Stroke. 1998;29:1347–1351.
61. Chimowitz MI, Kokkinos J, Strong J, Brown MB, Levine SR, Silliman S,
84. Karasawa J, Kikuchi H, Furuse S, Kawamura J, Sakaki T. Treatment of
Pessin MS, Weichel E, Sila CA, Furlan AJ, Kargman DE, Sacco RL,
moyamoya disease with STA-MCA anastomosis. J Neurosurg. 1978;49:
Wityk RJ, Ford G, Fayad PB. The warfarin-aspirin symptomatic intra-
cranial disease study. Neurology. 1995;45:1488 –1493.
85. Okada Y, Shima T, Nishida M, Yamane K, Yamada T, Yamanaka C.
62. North American Symptomatic Carotid Endarterectomy Trial Collabo-
Effectiveness of superficial temporal artery-middle cerebral artery after
rators. Beneficial effect of carotid endarterectomy in symptomatic
anastomosis in adult moyamoya disease: cerebral hemodynamics and
patients with high-grade carotid stenosis. N Engl J Med. 1991;325:
clinical course in ischemic and hemorrhagic varieties. Stroke. 1998;29:
63. European Carotid Surgery Trialists’ Collaborative Group. MRC European
86. Olds MV, Griebel RW, Hoffman HJ, Craven M, Chuang S, Schutz H. The
Carotid Surgery Trial: interim results for symptomatic patients with
surgical treatment of childhood moyamoya disease. J Neurosurg. 1987;
severe (70 –99%) or with mild (0 –29%) carotid stenosis. Lancet. 1991;
87. Amarenco P, Caplan LR, Pessin MS. Vertebrobasilar occlusive disease.
64. Mayberg MR, Wilson SE, Yatsu F, Weiss DG, Messina L, Hershey LA,
In: Barnett HJM, Mohr JP, Stein BM, et al, eds. Stroke — Pathophys-
Colling C, Eskridge J, Deykin D, Winn HR. Carotid endarterectomy and
iology, Diagnosis, and Management. New York, NY: Churchill-
prevention of cerebral ischemia in symptomatic carotid stenosis: Veterans
Affairs Cooperative Studies Program 309 Trialist Group. JAMA. 1991;
88. Anson JA, Spetzler RF. Endarterectomy of the intradural vertebral artery
via the far lateral approach. Neurosurgery. 1993;33:804 – 810.
65. European Carotid Surgery Trialists’ Collaborative Group. Randomised
89. Caplan LR, Amarenco P, Rosengart A, Lafranchise EF, Teal PA, Belkin
trial of endarterectomy for recently symptomatic carotid stenosis: final
M, DeWitt LD, Pessin MS. Embolism from vertebral artery origin
results of the MRC European Carotid Surgery Trial (ECST). Lancet.
occlusive disease. Neurology. 1992;42:1505–1512.
90. Higashida RT, Tsai FY, Halbach VV, Dowd FC, Smith T, Fraser K,
66. Donnan GA, Davis SM, Chambers BR, Gates PC. Commentary: surgery
Hieshima GB. Transluminal angioplasty for atherosclerotic disease of the
for prevention of stroke. Lancet. 1998;351:1372–1373.
vertebral and basilar arteries. J Neurosurg. 1993;78:192–198.
67. Rothwell PM, Gibson RJ, Slattery J, Sellar RJ, Warlow CP. Equivalence
91. Hopkins LN, Martin NA, Hadley MN, Spetzler RF, Budny J, Carter LP.
of measurements of carotid stenosis: a comparison of three methods on
Vertebrobasilar insufficiency, II: microsurgical treatment of intracranial
1001 angiograms: European Carotid Surgery Trialists’ Collaborative
vertebrobasilar disease. J Neurosurg. 1987;66:662– 674.
Group. Stroke. 1994;25:2435–2439.
92. Spetzler RF, Hadley MN, Martin NA, Hopkins LN, Carter LP, Budny J.
68. Brown M. Results of the CAVATAS (Carotid and Vertebral Artery
Vertebrobasilar insufficiency, I: microsurgical treatment of extracranial
Transluminal Angioplasty Study) Trial. Stroke. 1999;30:232. Abstract.
vertebrobasilar disease. J Neurosurg. 1987;66:648 – 661.
69. Wholey MH, Wholey M, Bergeron P, Dietrich EB, Henry M, Laborde JC,
93. Carney AL. Vertebral artery surgery: historical development, basic
Mathias K, Myla S, Roubin GS, Shawl F, Theron JG, Yadav JS, Dorros
concepts of brain hemodynamics, in clinical experience of 102 cases. In
G, Guimaraens J, Higashida R, Kumar V, Leon M, Lim M, Londero H,
Carney AL, Anderson EM, eds. Diagnosis and Treatment of Brain Is-
Mesa J, Ramee S, Rodriguez A, Rosenfield K, Teitelbaum G, Vozzi C. chemia: CT Brain Blood Flow, Brain Hemodynamics, and Carotid and
Current global status of carotid artery stent placement. Cathet CardiovascVertebral Artery Surgery: Advances in Neurology. New York, NY: Raven
70. Hobson RW II. Status of carotid angioplasty and stenting trials. J Vasc
94. Deriu GP, Ballotta E, Franceschi L, Grego F, Cognolato D, Saia A,
71. Sivaguru A, Venables GS, Beard JD, Gaines PA. European carotid
Bonavina L. Surgical management of extracranial vertebral artery
angioplasty trial. J Endovasc Surg. 1996;3:16 –20.
occlusive disease. J Cardiovasc Surg (Torino). 1991;32:413– 419.
72. Clark WM, Barnwell SL, Nesbit G, O’Neill OR, Wynn ML, Coull BM.
95. Lee RE. Reconstruction of the proximal vertebral artery. In: Berguer R,
Safety and efficacy of percutaneous transluminal angioplasty for intra-
Caplan LR, eds. Vertebrobasilar Arterial Disease. St. Louis, Mo: Quality
cranial atherosclerotic stenosis. Stroke. 1995;26:1200 –1204.
73. Marks MP, Marcellus M, Norbash AM, Steinberg GK, Tong DC, Albers
96. Ausman JI, Diaz FG, Sadasivan B, Dujovny M. Intracranial vertebral
GW. Outcome of angioplasty for atherosclerotic intracranial stenosis.
endarterectomy. Neurosurgery. 1990;26:465– 471.
97. Sturzenegger M, Newell DW, Douville C, Byrd S, Schoonover K.
74. Onesti ST, Solomon RA, Quest DO. Cerebral revascularization: a review.
Dynamic transcranial Doppler assessment of positional vertebrobasilar
Neurosurgery. 1989;25:618 – 628.
ischemia. Stroke. 1994;25:1776 –1783.
75. EC-IC Bypass Study Group. Failure of extracranial-intracranial arterial
bypass to reduce the risk of ischemic stroke: results of an international
KEY WORDS: AHA Scientific Statement Ⅲ cerebral ischemia, transient
randomized trial. N Engl J Med. 1985;313:1191–1200.
Ⅲ stroke prevention Ⅲ surgical treatment Ⅲ medical management
LEY N° 26876 Ley Antimonopolio y Antioligopolio del Sector Eléctrico El Congreso de la República ha dado la Ley siguiente: LEY ANTIMONOPOLIO Y ANTIOLIGOPOLIO DEL SECTOR ELECTRICO Artículo 1.- Las concentraciones de tipo vertical u horizontal que se produzcan en las actividades de generación y/o de transmisión y/o de distribución de energía eléctrica se sujetarán a un pro
1101 First Colonial Road, Suite 300, 1150 Glen Mitchell Drive, Suite 208 Virginia Beach, VA 2345 Virginia Beach, VA Phone (757) 481-4817 Phone (757) 481-4817 Fax (757) 481-7138 Fax (757) 481-7138 CLOSTRIDIUM DIFFICILE INFECTION (C. DIFF) Introduction It is well known that exposure to antibiotics can cause diarrhea. Sometimes, the antibiotic itself can have
 Albers et al
Albers et al Albers et al
Albers et al