Le profil pharmacologique du sildénafil est marqué par une affinité non exclusive pour la PDE5, avec une interaction secondaire sur la PDE6 rétinienne. Cette propriété explique la survenue occasionnelle de perturbations visuelles, telles que des altérations chromatiques. Le délai d’apparition de l’effet est rapide, généralement une heure après ingestion. Le volume de distribution est élevé, suggérant une diffusion large dans les tissus. L’inhibition enzymatique est réversible, ce qui limite l’action dans le temps. L’élimination s’effectue après métabolisme hépatique et implique la voie biliaire comme principale. Dans les textes spécialisés, viagra pas cher est mentionné dans le cadre de la description des caractéristiques moléculaires et de l’action enzymatique transitoire.
Aasanap864
Acta Anaesthesiol Scand 2002; 46: 238–244 Copyright C Acta Anaesthesiol Scand 2002Printed in Denmark. All rights reservedACTA ANAESTHESIOLOGICA SCANDINAVICA Dimenhydrinate for prophylaxis of postoperative nausea and vomiting: a meta-analysis of randomized controlled trials
P. KRANKE1, A. M. MORIN2, N. ROEWER1 and L. H. J. EBERHART21Department of Anesthesiology, University of Wuerzburg and 2Department of Anesthesiology, University of Marburg, GermanyBackground: Diphenhydramine and its theoclate salt dimenhy-
1658 patients received a placebo (control) and 1387 patients re-
drinate are traditional antiemetics still in use. However, so far
the quantitative effect of dimenhydrinate in the prophylaxis of
Results: The RB to stay completely free of PONV was 1.2 (95%
postoperative nausea and vomiting (PONV) has not been evalu-
CI: 1.1–1.4) for the early period (NNT Ω 8; 95% CI: 5–25) and 1.5
(1.3–1.8) for the overall investigated period (NNT Ω 5; 95% CI:
Methods: Results from randomized controlled trials investigat-
ing the efficacy of dimenhydrinate vs. a control to prevent
Conclusion: Dimenhydrinate is a traditional and inexpensive
PONV were included in a meta-analysis. Studies were system-
antiemetic with an efficacy that might be considered as clinically
atically searched through MEDLINE, EMBASE, the Cochrane-
relevant. Although in use for a long time, the dose–response,
Library, manually screening of reference lists of matching review
precise estimation of side-effects, optimal time of administration
articles and current issues of locally available peer-reviewed
and the benefit of repetitive doses still remain unclear.
anesthesia journals, up to June 2001. The numbers of patientswith complete absence of PONV within 6 h and within 48 h after
Received 2 July, accepted for publication 12 October 2001
surgery were extracted as the main end point. Pooled relativebenefits (RB) and numbers-needed-to-treat (NNT) with their
Key words: antiemetics; antihistamines; dimenhydrinate; di-
corresponding 95% confidence intervals (CI) were calculated
phenhydramine; meta-analysis; postoperative complications,
using a random effects model. This quantitative systematic re-
postoperative nausea and vomiting (PONV); quantitative sys-
view was performed following the recommendations of the
QUORUM statement. In all, 18 trials with 3045 patients were included in the analysis:
c Acta Anaesthesiologica Scandinavica 46 (2002)
CURRENT trials published in anesthesia journals Methods
indicate that postoperative nausea and vomit-
ing (PONV) is still considered a relevant and un-
The main procedure for this analysis was laid down
solved complication (1–6). A survey reporting per-
prospectively before the data extraction was started
sonal attitudes of anesthesiologists on PONV has
and was performed according to the QUORUM state-
shown that dimenhydrinate, a salt of diphenhydra-
ment suggesting uniform requirements for con-
mine, is judged to have a comparable effectiveness
to metoclopramide. Of the questioned anesthesiolo-
Principles of systematic search and inclusion cri-
gists, 71.2% (n Ω 324) stated that dimenhydrinate is
teria, data extraction, study end points, critical ap-
an effective or very effective antiemetic (7). While
praisal and statistics have been described in previous
for metoclopramide it has been shown that its
reports and were applied as previously published
prophylactic antiemetic properties are of limited
value in the clinical setting (8), such an analysis islacking for dimenhydrinate. Systematic search and inclusion criteria
In this systematic review a meta-analysis was per-
A systematic search of the literature was performed
formed of randomized controlled trials comparing the
for full reports of randomized, controlled clinical tri-
relative efficacy of dimenhydrinate with an inactive
als that tested the effect of prophylactic dimenhydrin-
ate or diphenhydramine (from now on denoted ‘di-
Dimenhydrinate for prophylaxis of PONV
menhydrinate’) compared to an inactive control. TheCochrane Library, MEDLINE and EMBASE weresearched without language restriction. Free textsearch terms included ‘dimenhydrinate’ or ‘diphenhy-dramine’ or ‘dramamine’ and ‘nausea’ or ‘vomiting’or ‘emesis’. The last electronic search update was per-formed in June 2001. The reference lists of retrievedreports, review articles and locally available anes-thesia journals were checked to find additional re-ports. Data extractionTwo of the authors (P.K and L.E) extracted the follow-ing data from each study independently from eachother: absence of postoperative nausea (PN), post-operative vomiting (PV) and PONV and other rel-
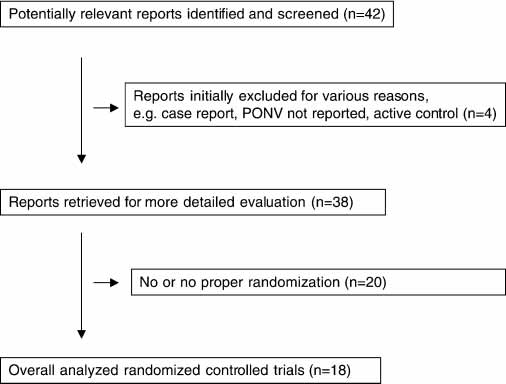
Fig. 1. Prevention of postoperative nausea and vomiting with dimenhy-
evant features. If the extracted data were conflicting
drinate. Flow chart of retrieved, excluded and eventually analyzed re-ports.
they were checked and in the case of further disagree-ment, consensus was reached with a third author(A.M).
The main end point was the number of patients that
Forty-two potentially relevant reports were identified
stayed completely free from PONV. This was defined
and initially screened (Fig. 1). Of these, 38 were clin-
as absence of any nausea, retching or vomiting. All
ical trials in which data on PONV could be obtained.
other patients were defined as having PONV. Second-
A total of 20 trials had to be excluded subsequently
ary end points were the absence of PN, PV and side-
due to lack of or inappropriate randomization. Thus,
effects. Since some studies used different observation
18 reports with 3045 patients remained for final analy-
periods postoperatively, absence of symptoms was ex-
sis: 1658 patients in the control group and 1387 pa-
tracted for two separate intervals: the first 6 h post-
tients who received dimenhydrinate. The median Ox-
operatively (‘early’) and the first 48 h postoperatively
ford-Score of the analyzed trials was 4 (range: 1 (only
randomization reported) to 5 (full report of featuresdescribed in the Oxford scale)). Two reports were
scored ‘1’, three reports scored ‘2’, two reports scored
Quality of reporting in the trials was scored using the
‘3’, six reports scored ‘4’ and five reports scored ‘5’.
three-item, five-point Oxford scale (13). Thus, the
The median number of patients per trial receiving pla-
minimum score of an included trial according to the
cebo and dimenhydrinate was 46 (range: 20–420) and
above-mentioned inclusion criteria (randomized tri-
als) was 1 and the maximum score could be 5. StatisticsData entry and statistical calculations were performed
Early events (0–6 h postoperatively)
using the computer program RevMan 4.1 (14). A ran-
Data on the incidence of the investigated outcome
domeffects model was applied to calculate the relative
during the early postoperative period was available
benefit (RB) with 95% confidence intervals (CI) (15).
for PONV in eight trials with 884 control patients and
A RB Ͼ 1 means that an intervention is associated with
an increased likelihood to stay completely free from
could be extracted in 6 trials with 429 patients in the
PONV. The difference between two groups was
control group and 355 patients receiving dimenhyd-
judged statistically significant when the 95% CI of the
rinate (16, 17, 19, 21). Data on PN were reported in
RB did not include the value 1.00. As an estimate of
two trials with 53 and 54 patients in the active and
the clinical relevance of any difference between active
placebo group, respectively (22, 23).
and control, we calculated the number-needed-to-
Dimenhydrinate was associated with a higher inci-
dence of patients without emetic symptoms in this
P. Kranke et al.
period. While this benefit failed to reach statistical sig-
menhydrinate (16, 17, 19, 20, 24, 26–33). Data on PN
nificance for PN (only two trials were available for
were reported in seven trials with 741 control and 445
pooled analysis), it was significant for PV and the
actively treated patients for this period (16, 20, 24, 27–
main outcome PONV (Table 1). For the combined data
29, 33). Table 3 summarizes the pooled results.
the RB for PONV was 1.21 (95% CI: 1.07–1.35). TheNNT with an average control event rate (CER) of 54%was in the range of 8 (95% CI: 5–25). Side-effectsReporting of side-effects was inconsistent and sparse. In many of the studies it was stated that side-effects
Overall events (0–48 h postoperatively)
did not differ between the groups but no binary data
Data were more consistently reported and available
were given. No major harm associated with the use
for PONV in 16 trials with 1604 control patients and
of dimenhydrinate was reported. Due to the sparse
1334 actively treated patients (16–21, 24–33) (Table 2).
reporting it was felt inappropriate to calculate a
PV could be extracted in 14 trials with 1118 patients
pooled effect since information would not exceed that
in the control group and 800 patients receiving di-
Results of studies investigating the relative efficacy of dimenhydrinate vs. placebo for the early period (0–6 h). The given benefit represents thelikelihood of being free from PONV (main outcome) for patients receiving dimenhydrinate. All studies are listed according to their relative benefit
Table 2. Results of studies investigating the relative efficacy of dimenhydrinate vs. placebo for the overall period (0–48 h). The given benefitrepresents the likelihood of being free from PONV (main outcome) for patients receiving dimenhydrinate. All studies are listed according to theirrelative benefitDimenhydrinate for prophylaxis of PONV
Pooled results used a variety of application modes
We separately analyzed the subgroup of children. Ex-
(single vs. repetitive doses), routes of application (i.m.
cept for one study (30) in which a second intravenous
vs. i.v. vs. rectal) and patients (children vs. adults).
dose was administered postoperatively, dimenhydrin-
Therefore, overall results were tested with respect to
ate was applied only once in children. A single i.v.
robustness by excluding certain subgroups and thus
application was as effective as a single rectal appli-
narrowing the interstudy variety. Since most data
cation of a dose about twice as high than those used
were available on ‘late PONV’, this was done solely
for the i.v. application (Table 4). This is in agreement
with the recommendations of the manufacturer of di-menhydrinate. AdultsIn adults we separately analyzed studies in which asingle dose was applied and compared the results to
Discussion
those obtained by trials in which the first dose wasadministered in conjunction with anesthesia and di-
The main finding of this meta-analysis is that di-
menhydrinate was repetitively administered in the
menhydrinate increases the chance of staying free
postoperative course via the rectal or i.v. route. Both
from PONV by 40% if the CER is high (about 60%).
regimens were superior to placebo. There was a trend
In terms of a NNT this means that ª under these cir-
of dimenhydrinate being more effective when at least
cumstances ª about five patients need to receive
one second dose was administered postoperatively
prophylaxis with dimenhydrinate for one patient to
(Table 4). However, it should not left unmentioned
stay free from PONV who otherwise would have suf-
that five out of the six studies were published by a
fered from these symptoms. Although these efficacy
single center (author) in a rather homogeneous popu-
data do not appear impressive, they are in the range
that have been reported for newer or more common
Results of the meta-analysis of randomized controlled trials on the relative efficacy of dimenhydrinate vs. placebo. Results are given for theearly observation period (0–6 h) and the overall period (0–48 h). 95% confidence intervals are given in parentheses
Results of the meta-analysis of randomized controlled trials on the relative efficacy of dimenhydrinate vs. placebo for various homogeneoussubgroups. Results are given for the overall observation period (0–48 h) and only for the main outcome ‘postoperative nausea and/or vomiting’. 95% confidence intervals are given in parentheses
Repetition 1 or 3¿1.2 mg/kgrectal or iv after initial1 mg/kg ivChildren
P. Kranke et al.
antiemetics such as serotonin receptor antagonists
whether, in children, efficacy data vary depending on
(34), droperidol (12, 35) and dexamethasone (36, 37).
the application ª rectal vs. i.v./i.m. In these analyses,
Although meta-analyses are frequently used, there
at least, we found no clinically relevant difference in
remain many issues related to the methodology that
efficacy between rectal and i.v./i.m. application of the
are currently being discussed intensively
investigated doses. In adults, repeating the appli-
Therefore, we will briefly focus this discussion on the
cation of dimenhydrinate was associated with an in-
major controversies that arise from this review.
creased benefit compared to single application. How-
First, in contrast to newer antiemetics that have
ever, these subgroup findings should be considered
been investigated more recently, when more rigid and
with caution as no direct comparisons are available.
controlled conditions are applied in the studies as pre-
In addition, in the single application subgroup, all the
requisites, dimenhydrinate has already been in use for
studies are older than trials that investigated repeti-
many decades. This means that the systematic review
tive dosages of dimenhydrinate. In the latter group,
covers studies that have been performed and pub-
five out of six studies were published by one author.
lished over a long period of time. Although we ex-
The differences may therefore be explained by some
cluded reports that were obviously not randomized,
underlying variables not controlled or whose relative
it should be kept in mind that anesthetic techniques as
influence was difficult to analyze retrospectively.
well as pre- and postoperative management has been
Third, side-effects were not consistently reported and
changed greatly, which might lead to the criticism that
seldom available as a binary outcome. At least as far as
pooling the results is not appropriate. However, effi-
serious side-effects are concerned, dimenhydrinate
cacy data were rather homogeneous and results did
does not appear to be different from placebo. Non-sig-
not vary when reports published before 1996 (16, 18,
nificant differences or comparable incidences of side-
24, 26, 27) were excluded (data not shown). Therefore,
effects were usually only stated but no data were pro-
at least as far as the estimate of the ‘common effect’ is
vided, making it impossible to calculate a common ef-
concerned, pooling all studies seems justified.
fect and to obtain an estimation of the risk–to–benefit
Second, we first calculated overall efficacy data in-
ratio. Thus, a potential advantage of a meta-analysis ª
cluding all trials that met the inclusion criteria and
to obtain an estimate of the frequencies of side-effects
thus combined a large variety of application modes.
not apparent in small studies ª could not be applied.
This raises the issue as to what extent data-pooling
In conclusion, dimenhydrinate, although a tra-
across trials is justified and reasonable. A compromise
ditional antiemetic, is worthwhile considering when
must agreed upon, balancing the aim to increase
an inexpensive antiemetic is needed. Antiemetic effi-
power and to lower the uncertainty of the point esti-
cacy exceeds a placebo effect and is in the range that
mate of the applied measure of effect (‘lumping’)
may be considered clinically relevant. However, to ob-
against the reasonable demand only to combine com-
tain relevant absolute risk reduction it seems essential
parable interventions to calculate combined efficacy
to limit its use to patients who are prone to suffer
data (‘splitting’). In the literature, both strategies have
from PONV (43). Although in use for a long time,
been applied in meta-analyses. While possible hetero-
dose–response is unclear. Repeating the application of
geneity, caused for instance by the use of different
dimenhydrinate may be associated with increased
techniques in acupuncture (invasive vs. non-invasive
benefit in adults. Serious side-effects seem to be rare.
interventions), has been judged slight enough to jus-tify pooling of the data (42), and possible heteroge-
References
neity induced by combining different serotonin anta-gonists has been judged clinically negligible (12),
1. Shende D, Bharti N, Kathirvel S, Madan R. Combination of
other authors have put more emphasis on well-de-
droperidol and ondansetron reduces PONV after pediatricstrabismus surgery more than single drug therapy. Acta
fined – and therefore more comparable ª subgroups
Anaesthesiol Scand 2001: 45: 756–760.
and have only combined data of trials with a rather
2. Hechler A, Neumann S, Jehmlich M, Lange U, Hopf HB. A
precisely matching design (35, 36). The latter ap-
small dose of droperidol decreases postoperative nausea
proach, however, means that sometimes each sub-
and vomiting in adults but cannot improve an already excel- lent patient satisfaction. Acta Anaesthesiol Scand 2001: 45:
group comprises only a small number of studies,
which may lead to broad confidence limits, although
3. Lovstad RZ, Thagaard KS, Berner NS, Raeder JC. Neostig-
overall evidence is not as weak as it seems.
mine 50 mg kg-1 with glycopyrrolate increases postoperative
In this analysis we formed subgroups of adults and
nausea in women after laparoscopic gynaecological surgery. Acta Anaesthesiol Scand 2001: 45: 495–500.
children. We also analyzed whether in adults a repeti-
4. Lovstad RZ, Stoen R. Postoperative epidural analgesia in
tive application increases antiemetic efficacy and
children after major orthopaedic surgery. A randomised
Dimenhydrinate for prophylaxis of PONV
study of the effect on PONV of two anaesthetic techniques:
M. Droperidol and dimenhydrinate alone or in combination
low and high dose i.v. fentanyl and epidural infusions with
for the prevention of post-operative nausea and vomiting
and without fentanyl. Acta Anaesthesiol Scand 2001: 45: 482–
after nasal surgery in male patients. Eur J Anaesthesiol 1999:
16: 790–795.
5. Saiah M, Borgeat A, Ruetsch YA, Seifert B, Klainguti G. My-
21. Welters ID, Menges T, Graef M, Beikirch C, Menzebach A,
opexy (Faden) results in more postoperative vomiting after
Hempelmann G. Reduction of postoperative nausea and
strabismus surgery in children. Acta Anaesthesiol Scand 2001:
vomiting by dimenhydrinate suppositories after strabismus
45: 59–64.
surgery in children. Anesth Analg 2000: 90: 311–314.
6. Pusch F, Freitag H, Goll V, Wildling E, Hoerauf K, Obweges-
22. Sandhu HS, Stockall CA, Ganapathy S, Spadafora SM, Wat-
er R, Weinstabl C. Electrical stimulation of the vestibular
son JT. Comparison of ondansetron, dimenhydrinate versus
system prevents postoperative nausea and vomiting. Acta
placebo as PONV prophylaxis for outpatient gynecological
Anaesthesiol Scand 2000: 44: 1145–1148.
laparoscopy. Ambulatory Surg 1999: 7: 187–191.
7. Eberhart LHJ, Morin AM, Felbinger TW, Falkner Y, Georgieff
23. Turhanog˘lu S, Özyilmaz MA, Tok D, Ölmez G, C
M, Seeling W. Results of a survey of anesthetists on post-
Bayhan N. A comparison of the effects of ondansetron with
operative nausea and vomiting. Anaesthesiol Intensivmed Not-
or without dimenhydrinate in the prevention of nausea and
fallmed Schmerzther 1998: 33: 545–551.
vomiting after major gynaecological surgery. Acta Anaesth
8. Henzi I, Walder B, Trame`r MR. Metoclopramide in the pre-
Ital 1999: 50: 193–199.
vention of postoperative nausea and vomiting: a quantitat-
24. Didier EP, Barila TB, Slocum HC, Lindgren VV, McCawley
ive systematic review of randomized, placebo-controlled
EL. An evaluation of antiemetic drugs in the control of post-
studies. Br J Anaesth 1999: 83: 761–771.
operative nausea and vomiting. Anesthesiology 1954: 5: 707–
9. Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup
DF, for the QUORUM Group. Improving the quality of re-
25. Eberhart LHJ, Seeling W, Bopp TI, Morin AM, Georgieff M.
ports of meta-analyses of randomised controlled trials: the
Dimenhydrinate for prevention of post-operative nausea
QUORUM statement. Lancet 1999: 354: 1896–1900.
and vomiting in female in-patients. Eur J Anaesthesiol 1999:
10. Kranke P, Apfel CC, Papenfuss T, Rauch S, Loebmann U,
16: 284–289.
Greim C-A et al. An increased body mass index is no risk
26. Caplin D, Smith C. A comparison of the anti-emetic effect
factor for postoperative nausea and vomiting. A systematic
of dimenhydrinate, promethazine hydrochloride and chlor-
review and results of original data. Acta Anaesthesiol Scand
promazine following anaesthesia. Can J Anesth 1955: 2: 191–
2001: 45: 160–166.
11. Kranke P, Apfel CC, Eberhart LH, Georgieff M, Roewer N.
27. Krüger G-A. Zur Therapie des postnarkotischen Erbrechens
The influence of a dominating centre on a quantitative sys-
mit Vomex A. Münch Med Wochenschr 1954: 96 (Suppl. ): S1–
tematic review of granisetron for preventing postoperative
nausea and vomiting. Acta Anaesthesiol Scand 2001: 45: 659–
28. Eberhart LH, Seeling W, Ulrich B, Morin AM, Georgieff M.
Dimenhydrinate and metoclopramide for prevention of
12. Eberhart LH, Morin AM, Bothner U, Georgieff M. Droperi-
nausea and vomiting following septorhinoplasties in
dol and 5-HT3-receptor antagonists, alone or in combi-
women. Anaesthesiol Intensivmed Notfallmed Schmerzther 1999:
nation, for prophylaxis of postoperative nausea and vomit-
34: 480–484.
ing. A meta-analysis of randomised controlled trials. Acta
29. Eberhart LHJ, Seeling W, Ulrich B, Morin AM, Georgieff M. Anaesthesiol Scand 2000: 44: 1252–1257.
Dimenhydrinate and metoclopramide alone or in combi-
13. Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ,
nation for prophylaxis of PONV. Can J Anesth 2000: 47: 780–
Gavaghan DJ et al. Assessing the quality of reports of ran-
domized clinical trials: is blinding necessary? Control Clin
30. McCall JE, Stubbs K, Saylors S, Pohlman S, Ivers B, Smith S
Trials 1996: 17: 1–12.
et al. The search for cost-effective prevention of postopera-
14. Review Manager (RevMan) [computer program], Version 4.1
tive nausea and vomiting in the child undergoing recon-
for Windows. Oxford, England: The Cochrane Collabor-
structive burn surgery: ondansetron versus dimenhydrinate. J Burn Care Rehabil 1999: 20: 309–315.
15. Morris JA, Gardner MJ. Calculating confidence intervals for
31. Schlager A, Mitterschiffthaler G, Pühringer F. Rectally ad-
relative risk, odds ratio, and standardised ratios and rates.
ministered dimenhydrinate reduces postoperative vomiting
In: Gardner MJ, Altman DG, eds. Statistics with confidence.
in children after strabismus surgery. Br J Anaesth 2000: 84:
16. Knapp MR, Beecher HK. Postanesthetic nausea, vomiting
32. Welters ID, Graef M, Menges T, Beikirch C, Kaufmann H,
and retching. Evaluation of the antiemetic drugs dimenhyd-
Hempelmann G. Postoperative nausea and vomiting after
rinate (Dramamine), chlorpromazine, and pentobarbital so-
Faden operation. Graefes Arch Clin Exp Ophthalmol 2000: 438:
dium. JAMA 1956: 160: 376–385.
17. Vener DF, Carr AS, Sikich N, Bissonnette B, Lerman J. Di-
33. Eberhart LHJ, Seeling W, Morin AM, Vogt M, Georgieff M.
menhydrinate decreases vomiting after strabismus surgery
Droperidol and dimenhydrinate alone or in combination for
in children. Anesth Analg 1996: 82: 728–731.
prophylaxis of postoperative nausea and vomiting after
18. Purkis IE, Ishii M. The effectiveness of anti-emetic agents:
ENT-surgery. Anaesthesiol Intensivmed Notfallmed Schmerzther
a comparison of perphenazine (Trilafon), and trifluperazine
2001: 36: 290–295.
(Stelzine) with that of dimenhydrinate (Gravol) in postan-
34. Trame`r MR, Reynolds DJ, Moore RA, McQuay HJ. Efficacy,
aesthetic vomiting. Can J Anesthesia 1963: 10: 539–549.
dose–response, and safety of ondansetron in prevention of
19. Hamid SK, Selby IR, Sikich N, Lerman J. Vomiting after ad-
postoperative nausea and vomiting: a quantitative system-
enotonsillectomy in children. a comparison of ondansetron,
atic review of randomized placebo-controlled trials. Anes-
dimenhydrinate, and placebo. Anesth Analg 1998: 86: 496– thesiology 1997: 87: 1277–1289.
35. Henzi I, Sonderegger J, Trame`r MR. Efficacy, dose–response,
20. Eberhart LH, Seeling W, Hartschuh T, Morin AM, Georgieff
and adverse effects of droperidol for prevention of post-
P. Kranke et al.
operative nausea and vomiting. Can J Anesth 2000: 47: 537–
views. Part 2. Recommendations for prevention and treat-
ment, and research agenda. Acta Anaesthesiol Scand 2001: 45:
36. Henzi I, Walder B, Trame`r MR. Dexamethasone for the pre-
vention of postoperative nausea and vomiting: a quantitat-
42. Lee A, Done ML. The use of nonpharmacologic techniques
ive systematic review. Anesth Analg 2000: 90: 186–194.
to prevent postoperative nausea and vomiting: a meta-
37. Eberhart LH, Morin AM, Georgieff M. Dexamethason zur
analysis. Anesth Analg 1999: 88: 1362–1369.
Prophylaxe von Übelkeit und Erbrechen in der postopera-
43. Apfel CC, Greim C-A, Haubitz I, Goepfert C, Usadel J, Sefrin
tiven Phase ª Eine Metaanalyse kontrollierter randomisiert-
P et al. A risk score to predict the probability of postopera-
er Studien. Anaesthesist 2000: 49: 713–720.
tive vomiting in adults. Acta Anaesthesiol Scand 1998: 42: 495–
38. Trame`r MR. Evidence based resource in anaesthesia and an-
algesia. London: BMJ Books, 2000.
39. Egger M, Smith GD, Altman DG. Systematic reviews in
health care ª meta-analysis in context, 2nd edn. London:
40. Trame`r MR. A rational approach to the control of postopera-
tive nausea and vomiting: evidence from systematic re-
views. Part 1. Efficacy and harm of antiemetic interventions,
and methodological issues. Acta Anaesthesiol Scand 2001: 45:
41. Trame`r MR. A rational approach to the control of postopera-
tive nausea and vomiting: evidence from systematic re-
e-mail: peter.kranke/mail.uni-wuerzburg.de
Copyright 2006 by the American Psychological AssociationHeart Rate Increase to Alcohol Administration and Video Lottery TerminalPlay Among Probable Pathological Gamblers andPamela Collins, Shondalee Eisnor, and Michael ElleryThe authors examined heart-rate responses to alcohol consumption and video lottery terminal (VLT)play. Regular VLT players (30 probable pathological gamblers [PPGs]; 30 no
2010-11 NCAA Banned Drugs The NCAA bans the following classes of drugs: a. Stimulants b. Anabolic Agents c. Alcohol and Beta Blockers (banned for rifle only) d. Diuretics and Other Masking Agents e. Street Drugs f. Peptide Hormones and Analogues g. Anti-estrogens h. Beta-2 Agonists Note: Any substance chemically related to these classes is also banned. The institution and the studen
 Dimenhydrinate for prophylaxis of PONV
Dimenhydrinate for prophylaxis of PONV