Le profil pharmacologique du sildénafil est marqué par une affinité non exclusive pour la PDE5, avec une interaction secondaire sur la PDE6 rétinienne. Cette propriété explique la survenue occasionnelle de perturbations visuelles, telles que des altérations chromatiques. Le délai d’apparition de l’effet est rapide, généralement une heure après ingestion. Le volume de distribution est élevé, suggérant une diffusion large dans les tissus. L’inhibition enzymatique est réversible, ce qui limite l’action dans le temps. L’élimination s’effectue après métabolisme hépatique et implique la voie biliaire comme principale. Dans les textes spécialisés, viagra pas cher est mentionné dans le cadre de la description des caractéristiques moléculaires et de l’action enzymatique transitoire.
The rise and decline of nonsteroidal antiinflammatory drug-associated gastropathy in rheumatoid arthritis
Vol. 50, No. 8, August 2004, pp 2433–2440
2004, American College of Rheumatology
Nonsteroidal Antiinflammatory Drug–Associated Gastropathy
James F. Fries, Kirsten N. Murtagh, Mihoko Bennett, Ernesto Zatarain,
Objective. Nonsteroidal antiinflammatory drug 42% of patients, a rise in the use of “safer” NSAIDs (NSAID)–associated gastropathy is a major cause of from 19% to 48% of patients, and increasing use of hospitalization and death. This study was undertaken to proton-pump inhibitors, but not with change in age, examine whether recent preventive approaches have NSAID exposure, or GI risk propensity score. been associated with a declining incidence of NSAID Conclusion. The risk of serious NSAID gastropa- gastropathy, and, if so, what measures may have caused thy has declined by 67% in these cohorts since 1992. We the decline. estimate that 24% of this decline was the result of lower Methods. We studied 5,598 patients with rheuma- doses of NSAIDs, while 18% was associated with the use toid arthritis (RA) over 31,262 patient-years at 8 sites. of proton-pump inhibitors and 14% with the use of less We obtained standardized longitudinal information on toxic NSAIDs. These declines in the incidence of NSAID the patients that had been previously used to establish gastropathy are likely to continue. the incidence of NSAID gastropathy, and also informa- tion on patient risk factors and differences in toxicity
Nonsteroidal antiinflammatory drug (NSAID)–
between NSAIDs. Consecutive patients were followed up
associated gastropathy, which is associated with gastro-
with biannual Health Assessment Questionnaires and
intestinal (GI) pathology involving hemorrhage, perfo-
medical record audits between 1981 and 2000. The
ration, or obstruction of the GI tract and related
major outcome measure was the annual rate of hospi-
conditions, is the most prevalent of serious drug side
talization involving bleeding, obstruction, or perforation
effects, resulting in an estimated 100,000 hospitaliza-
of the gastrointestinal (GI) tract and related conditions.
tions annually in the US (1). Although it was originally
Results. Rates of GI-related hospitalizations rose
considered to be rare, the incidence of NSAID gastropa-
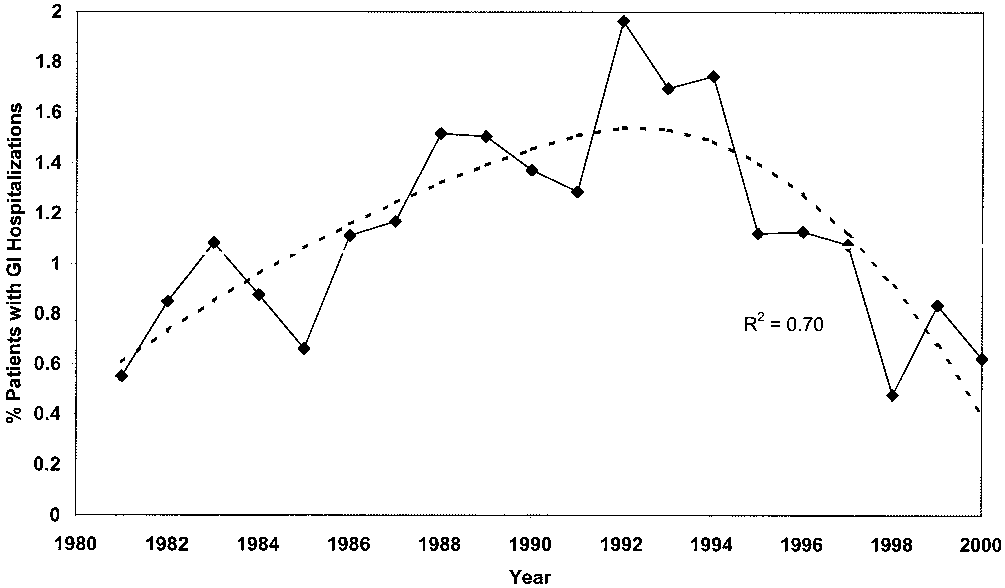
from 0.6% in 1981 to 1.5% in 1992 (P < 0.001), and then
thy is recognized to be ϳ1.2–1.6% per year in patients
declined to 0.5% in 2000 (P < 0.001). The fitted spline curve fit the data well (R2 ؍ 0.70). The period of rise was
with rheumatoid arthritis (RA), a relatively high-risk
mainly associated with increasing patient age and the
population. The relative risk of developing serious GI
GI risk propensity score. The period of decline was
complications in patients exposed to NSAIDs is 5–6
associated with lower doses of ibuprofen and aspirin, a
times that in those not exposed (2). The present status of
decline in the use of “more toxic” NSAIDs from 52% to
the epidemic (whether the incidence is rising, falling, orconstant) is not known. We hypothesized that recentpreventive approaches to NSAID gastropathy should
Supported by a grant from the NIH (AR-43584) to the
have led to a reduction in its incidence.
Arthritis, Rheumatism, and Aging Medical Information System.
James F. Fries, MD, Kirsten N. Murtagh, MS, Mihoko
Bennett, PhD, Ernesto Zatarain, MD, Bharathi Lingala, PhD, Bonnie
Medical Information System) investigators have been
Bruce, DrPH: Stanford University, Stanford, California.
following up consecutively enrolled RA patients from
Address correspondence and reprint requests to James F.
Fries, MD, Department of Medicine, Stanford University Medical
multiple settings since 1980, using systematic outcome
School, 1000 Welch Road, Suite 203, Palo Alto, CA 94304. E-mail:
assessment protocols (see the ARAMIS Web site at
http://www.ARAMIS.stanford.edu). We follow up pa-
Submitted for publication January 29, 2004; accepted in
tients longitudinally, audit hospitalizations, and collect
detailed data on drug use and adverse reactions (3,4). In
codes 531–535, 787, and 789. Attributions were validated by a
the present study, we sought to examine trends in the
physician who was blinded to each patient’s medication use. Statistical analysis. The percentage of patients with
incidence of NSAID gastropathy over time in this co-
GI-related hospitalizations (number of hospitalizations per
hort. We also sought to examine associations of NSAID
100 patient-years) was calculated as the total number of
gastropathy with changes in potentially explanatory vari-
incident GI-associated hospitalizations in a given year, divided
ables, which were prespecified as age, sex, GI risk
by the number of RA patients by year, and allowing only 1
propensity score, NSAID dose, use of specific NSAIDs,
hospitalization per patient per year. Since there was a period of
use of misoprostol, proton-pump inhibitors, and H
rising incidence followed by a period of declining incidence, we
used second-degree spline regression to determine the transi-
receptor antagonists, percentage of patients at each data
bank center, and frequency of NSAID exposure.
We identified patients receiving each NSAID for every
year at every site, including both prescription and over-the-counter use, and computed the percentage of patients receiv-
PATIENTS AND METHODS
ing each particular NSAID among all NSAID users. We
Patients. We studied 5,598 RA patients whose data
prespecified NSAIDs as relatively more toxic or relatively safer
were drawn from 8 ARAMIS data banks in the US and Canada
based on our own data (8), on the meta-analysis by Henry et al
(Stanford, California [2 data banks], Santa Clara County,
(9), and on the CLASS and VIGOR (Celebrex Long-Term
California, Wichita, Kansas, Saskatoon, Saskatchewan, Can-
Arthritis Safety and Vioxx Gastrointestinal Outcomes Re-
ada, Cincinnati, Ohio, Baltimore, Maryland, and Pittsburgh,
search) studies (10,11). Time trends also allowed classification
Pennsylvania), comprising 31,262 patient-years of observation.
of NSAIDs into those with increased use over time and thosewith decreased use over time. The percentage of patients
These centers are population-based (Saskatoon and Santa
receiving gastroprotective agents was calculated as the propor-
Clara County), university clinics with quite different charac-
tion of patients being treated with H receptor antagonists by
teristics (Stanford, Cincinnati, Baltimore, and Pittsburgh), and
prescription or over-the-counter, misoprostol, sucralfate,
private practice–based (Wichita), and thus are believed to be
and/or proton-pump inhibitors, divided by the number of
reasonably representative of RA patients in the US and
Canada. ARAMIS is a prospective, observational data bank
We also examined trends in average age, disease
system in which patients are enrolled consecutively under
duration, disability, the percentage of patients receiving
institutional review board approval, followed up for life, and
NSAIDs, the percentage of patients with increased use or
assessed prospectively by standard protocol for multiple vari-
decreased use of NSAIDs, the percentage of patients receiving
ables, including demographics, clinical and hospital outcomes,
prednisone, and the GI risk propensity score. GI risk propen-
mortality, and the frequency, dose, effectiveness, and toxicity
sity scores were computed using the method of Singh et al (12),
of specific treatments (5). The RA cohort reported herein was
based on age, disability, global health, prior GI-related hospi-
the subject of early reports establishing incidence rates, risk
talization, prednisone use, and prior NSAID-related GI side
factor models, and the relative toxicity of NSAIDs in gastropa-
effect. This score represents the likelihood of a patient having
thy, and thus provides a unique perspective from which to
a serious GI complication in the following year. Statistics were
computed using SAS for Windows, version 8.2 (Chicago, IL). Measures. Patients in the ARAMIS are asked to
complete the Health Assessment Questionnaire (HAQ) every6 months. The HAQ is a widely used, comprehensive, patient
self-reported outcome assessment instrument (6,7). Patientsreport on medication use, dosage, duration of use, and side
The major finding on the rates of hospitalization
effects. Information on both prescription and nonprescription
for NSAID gastropathy is apparent in Figure 1. By
aspirin and NSAID use is included. The protocol requires
conservatively using the fitted spline regression data,
followup of nonresponders, patient contact for missing infor-mation, acquisition of patient records for hospitalizations, and
rather than the raw values for each year, we found that
stringent quality control. Data from 1981 to 2000, during which
the rate of GI-related hospitalizations first increased
time prospective protocols were in place and remained con-
from 0.6% per year in 1981 to a peak of 1.5% in 1992,
and then decreased to 0.5% in 2000. The rate initially
Ascertainment of serious GI events. The primary out-
nearly tripled, then declined by 67% from its high point
comes were the number and incidence of serious GI eventsthat required hospitalization. Patients with bleeding of the
in 1992. The spline regression indicated a concave
upper or lower GI tract, clinically symptomatic gastritis, ulcers,
function that peaked in 1992. We therefore defined the
gastric outlet obstructions, and GI symptoms serious enough to
period of rise as 1981–1992 (the first period) and the
require hospitalization (abdominal pain, nausea, vomiting, or
period of decline as 1993–2000 (the second period).
diarrhea) were identified from medical records. GI-related
Trends over the period of rise and over the
hospitalizations were first determined by patient self-report ofhospitalization. Hospital records were then audited by trained
period of decline each were highly statistically significant
reviewers for identification of International Classification of
(P Ͻ 0.001), as was the fitted spline regression for these
Diseases, Ninth Revision, Clinical Modification diagnostic
trends (P Ͻ 0.001, R2 ϭ 0.70). GI-related hospitaliza-
tially explanatory variables. The average age of thepatients in the cohort increased by nearly 6 years from1981 to 1992, from 56.7 years to 62.2 years, and thenremained relatively constant thereafter. Composite GIrisk propensity scores followed a pattern of rise through1992 similar to that of the GI-related hospitalizationrates, followed by a plateau. The percentage of patientsreceiving NSAIDs declined from 87% to 76% by 1992,and thereafter remained fairly constant. Average HAQdisability index scores, on a 0–3 scale (7), rose slightly inthe first period and improved considerably in the secondperiod, which is consistent with recent findings of de-
Figure 1. Percentage of rheumatoid arthritis patients with serious
clining disability in RA associated with more aggressive
gastrointestinal (GI) events that required hospitalization, over time.
use of disease-modifying medications over the past 2
The dotted line is a second-degree spline-fitted curve for these data.
decades (13). Average pain scores, on a 0–3 visualanalog scale, and average patient global health assess-
tions as a percentage of all hospitalizations declined
ment scores, on a 0–100 scale, similarly rose and then
from 7.3% in 1981, to 5.7% in 1992, and to 4.8% in 2000.
fell, but differences were slight. Average disease dura-
When considering only those patients who were exposed
tion rose during the first period and subsequently de-
to NSAIDs, a curve that was higher than, but of similar
clined slightly. Prednisone use (average dosage ϳ7 mg/
shape as, that in Figure 1 was found, with a beginning
day throughout) increased in the second period; this
rate of GI-related hospitalizations of 0.5%, a peak of
would have been expected to increase the rates of
2.1% in 1992, and the final value of 0.5%. Results were
serious GI events during the period in which they were
consistent across the 8 data bank centers.
Table 1 summarizes the trends in some poten-
We also examined changes in drug dosage over
Characteristics of the study population by year*
* HAQ DI ϭ Health Assessment Questionnaire disability index; RA ϭ rheumatoid arthritis; NSAIDs ϭ nonsteroidal antiinflammatory drugs; GI ϭgastrointestinal. † See Figure 2. ‡ See Figure 3. Figure 2. Percentage of use of those drugs with increased usage over Figure 4. Percentage of rheumatoid arthritis (RA) patients taking
time (“less toxic” drugs), from among the total nonsteroidal antiin-
gastroprotective agents over time. H antagonists (H2) include cime-
tidine, ranitidine, and famotipine. Proton-pump inhibitors (PPI) in-clude omeprazole and lansoprozole. Misoprostol (Miso) is a syntheticprostaglandin, including misoprostol alone and in combination with
time. Ibuprofen and noncardiac aspirin dosages each
declined by ϳ40% in the second period and thus corre-lated with the decline in GI complications; other NSAIDdosages did not appreciably change. The percentage ofpatients taking low-dose (Յ325 mg per day) aspirin
2 years of the study. The 5 NSAIDs that showed an
increased from 3% in 1992 to 8% in 2000, while the
increase in use are all drugs that have been reported
average low-dose cardiac aspirin dosage declined from
to be among the least toxic of the NSAIDs (8–11).
ϳ200 mg per day to ϳ150 mg per day. We did not find
During our entire observation period, patients taking
increasing doses for any of the drugs in either period,
these drugs had a rate of serious GI events of 0.54%
and thus “dose creep” was eliminated as a possible cause
Figure 3 shows the time trends in market share
The proportion of use of each specific NSAID in
for the 8 drugs that were prespecified as more toxic. All
these cohorts was also calculated for each year. Figure 2
of these had reduced usage over the entire period.
shows trends for use of the drugs that were prespecified
Aspirin lost the largest share, although the greatest
as less toxic. The largest increase was in the use of
declines were in the usage of piroxicam, sulindac, and
ibuprofen (which showed, at the same time, a decline in
indomethacin. Each of these 8 drugs has been reported
dose) and in the use of the more specific cyclooxygenase
to have a higher-than-average toxic effect on the GI tract
1–sparing drugs rofecoxib and celecoxib over the last
(9,10). Over our observation period, patients takingthese drugs had a rate of serious GI events of 0.78% peryear.
Time trends in the use of gastroprotective agents
are shown in Figure 4. Two striking trends were evident:a rapid rise in the use of H receptor antagonists in the
first period, and a rapid rise in the use of proton-pumpinhibitors in the second period, which ended with a 16%use of proton-pump inihitors. Misoprostol (ϳ5%) andsucralfate were not widely used. Data on identificationor treatment of Helicobacter pylori infection were notreliably reported in the charts reviewed, but treatmentfor H pylori appeared to be rare. Figure 3. Percentage of use of drugs with decreased usage over time DISCUSSION
(“more toxic” drugs), from among the total nonsteroidal antiinflam-
The prevalence of serious GI events associated
matory drug (NSAID) use. The aspirin data exclude use of cardiopro-tective doses of aspirin.
with NSAID use in this large, longitudinal, multicenter
study of RA patients rose markedly from 0.6% of
NSAID gastropathy (24). Results were disappointing
patients per year in 1981 to 1.5% per year in 1992, and
when regular doses were used, but prevention was
then fell to 0.5% per year in 2000. Both the rise and the
subsequently documented with double doses of H an-
decline were steady, were consistent, and have plausible
tagonists (25). Misoprostol, a synthetic prostaglandin
explanations. The decline in NSAID-related GI prob-
analog, was studied by Graham et al in 1988, and those
lems, if generalizable, represents a substantial improve-
authors showed that endoscopic ulcers decreased follow-
ment in the health of the public. These improvements
ing this therapy (26). Decreases in GI complications of
are likely to be the result of the joint efforts of epide-
ϳ40% with the use of misoprostol were shown by
miologists, gastroenterologists, rheumatologists, regula-
Silverstein et al in 1995 (27). A meta-analysis of preven-
tion trials by Koch et al in 1996 suggested that the newer
A number of relevant events over the past de-
proton-pump inhibitors would be more effective preven-
cades may have directly influenced these trends (14). We
tive agents (28), and this was confirmed by Yeomans et
have taken note of a few of the earliest reports and those
al in 1998 (29). Treatment of H pylori infection has been
that may have had some of the greatest impacts. The
found to be as effective as proton-pump inhibitors in
earliest hints of NSAID-related GI problems are found
some studies (30–32), although the incidence of this
in the observations of Douthwaite and Lintott in 1938
(15), and these observations were repeated in a more
modern era by Sun et al in 1974 (16). Levy noted the
broad use during the period of declining incidence of
association between aspirin use and major GI bleeding
NSAID gastropathy in this study, and all of these agents
in 1974 (17). The high prevalence of NSAID-associated
were promoted as being safer than their predecessors.
endoscopic erosions and ulcers led Roth and Bennett to
They included nabumetone and etodolac in 1991, Ar-
coin the term NSAID gastropathy in 1987 and to suggest
throtec (which combined diclofenac and misoprostol) in
that it might be quite common (18). The potentially
1997, celecoxib in 1998, and rofecoxib in 1999 (30).
life-threatening nature of these problems was suggested
Studies have suggested that the cyclooxygenase
by Armstrong and Blower in 1987 (19). In 1988, Griffin
1–sparing agents celecoxib and rofecoxib have toxic
and colleagues noted the association of NSAID use and
effects on the GI tract that are only half that of the
mortality linked to peptic ulcer disease in the elderly
traditional NSAIDs (10,11,33,34). Even newer agents
(20). In 1989, our group, using the patient cohorts of this
have since entered the market but were not available
current report, began to quantitate the epidemiology of
during the present study period. A change in treatment
NSAID gastropathy, finding a GI-related hospitalization
strategy for RA patients from one based on NSAIDs to
incidence of 1.6% per year in RA patients and a relative
one based on disease-modifying antirheumatic drugs
risk of 5.2 (21); these data are approximated in the
(DMARDs) occurred over this period of observation
present study by the average values in the period of
(35–37) and likely explains the decline in NSAID usage
In 1991, our group extended these observations
The period of rising frequency of NSAID gas-
and identified age and other variables that were associ-
tropathy was associated with a strong trend toward
ated with increased risk of NSAID gastropathy (2).
increasing age with NSAID use in these cohorts. Age has
Griffin and colleagues also observed the strong associa-
consistently been identified as the most important risk
tion with age in the Tennessee Medicaid data set in 1991
factor for NSAID gastropathy, other than prior GI-
(22). We also analyzed differences in toxicity among the
related hospitalization, and acts exponentially as a risk
NSAIDs in 1991, finding up to 4-fold differences (8)
factor (2,22). The average age of RA patients in these
between each NSAID despite a prevailing prior view
cohorts rose by 5.5 years from 1981 to 1992, which is
that there were no such differences (23). By 1996, Henry
sufficient by itself to account for a near doubling of the
et al were able to identify 12 sets of studies consistently
incidence of serious GI events. The percentage of
showing differential toxicity among the NSAIDs, with a
NSAID-receiving patients older than age 75 years rose
similar magnitude of differences and with similar order-
from 4% to 14% over this same period. There also was
a smaller trend toward more use of NSAIDs in women,
These findings, even before they were published
and an increase in average disability levels, in pred-
and disseminated, began to affect the development of
nisone use, and in the overall GI risk propensity score.
new treatments. Roth and colleagues began, in 1987, to
Nevertheless, the percentage of RA patients tak-
explore the uses of H antagonists in the prevention of
ing NSAIDs in these cohorts was steadily decreasing,
which should have acted to lower the risks; this decline
tional 2%. After accounting for the increased GI risk
in NSAID use was likely to be related to the increasing
propensity scores, from a mean of 14 to a mean of 16,
emphasis on use of DMARDs to control disease activity
among those patients taking proton-pump inhibitors (8),
the estimate of the effects of gastroprotection sums to
creased during the period of rise, these agents have been
ϳ12% overall, and 18% of the observed decline.
found to be of little value, in regular doses, when used as
Third, conservatively assuming a linear dose-
prophylaxis against serious NSAID gastropathy (28).
response curve for NSAID complications, the 40%
The frequency of prednisone use, another risk factor,
reduction in dose for aspirin and ibuprofen, which made
increased during the period of rising incidence. There-
up 40% of the NSAID market share, would account for
fore, some originally plausible explanatory factors, such
a reduction of 16%, or 24% of the observed reduction.
as sex or increasing NSAID exposure, do not appear to
Thus, we estimate that 24% of the observed decline was
have played a role in the development of the epidemic.
due to lower doses of some NSAIDs, 18% was due to use
Increases in patient age, prednisone use, and the GI risk
of proton-pump inhibitors, and 14% was due to use of
propensity score are the most likely explanations for the
safer NSAIDs. We therefore have suggestive evidence to
explain about two-thirds (66%) of the observed decline.
In the period of declining frequency of serious GI
What factors may have contributed to the re-
complications, the frequency of NSAID use, average
mainder of the decline? These are more speculative
age, and GI risk propensity score all reached a plateau,
because of limitations in our data. It could be explained,
and therefore could not have made major contributions
in part, by uncaptured aspects of the 3 dominant forces.
to the decline. Disability levels declined somewhat,
For example, within the “more toxic NSAID” category,
possibly suggesting that the patients were sturdier. Im-
were there greater decreases in use of the most toxic
pressively, there was a striking shift in the use of specific
drugs? Were proton-pump inhibitors used almost exclu-
NSAIDs, with a decrease in use of the more toxic drugs
sively in the highest-risk patients, which would increase
and an increase in use of those with lesser toxicity. There
effects beyond what we projected? Were dose reductions
was a 40% decrease in the dosage of both aspirin and
in the most toxic, but less frequently used, agents, for
ibuprofen, both of which have a high frequency of use.
which we did not have sufficient data, important? Inter-
Moreover, a steady stream of new drugs entered the
action terms, which go beyond our data, could have
market, including nabumetone and etodolac, and the
made material contributions. Moreover, our explana-
cyclooxygenase 1–sparing drugs rofecoxib and celecoxib
tions are not entirely mutually exclusive, so that we
achieved large market shares toward the end of our
might have overestimated some contributions. What
were the effects, if any, of increasing use of endoscopy or
Which of these various trends may have contrib-
generally declining hospitalization rates? As disability
uted to the decline in serious GI events? The answers
levels in RA decline as a result of increasing DMARD
are intrinsically speculative, and therefore we discuss
use, do RA patients become more resistant to GI
them here, rather than presenting them as results. There
complications? There are many other potential contri-
are 3 particularly suggestive associations. First, we ob-
butions to the decline that we could not measure.
served a shift away from the use of NSAIDs with an
For example, we do not have data on H pylori
incidence of serious toxicity in the GI tract of 0.78% per
prevalence over time. Treatment of H pylori infection or
year toward NSAIDs with an average incidence of
reduction in prevalence of H pylori could have had an
0.54%, yielding a blended toxicity incidence rate of
effect. We tend to discount a major effect of H pylori,
0.72% in 1992 and of 0.65% in 2000, which is sufficient
however, since its prevalence in our cohort is likely to
to explain a reduction of ϳ14% of the overall 67%
have been low (US and Canadian patients with access to
decline in the incidence of serious GI events (a decline
care) and the relationship of H pylori to serious NSAID-
related GI events itself remains controversial. Overall, it
Second, use of proton-pump inhibitors rose from
appears to be reasonable to assume that most of the
none in 1992 to 16% in 2000. Assuming a preventive
decline in serious NSAID effects came from lower doses
benefit of 50% from the use of proton-pump inhibitors,
of safer drugs in conjunction with greater use of gastro-
their use would reduce the incidence of serious GI
complications by 8%. Assuming a 40% protection rate
National effects upon the epidemic of NSAID
from the use of misoprostol, with its lower frequency of
gastropathy are less encouraging. The national market
use, the incidence rates would be reduced by an addi-
for NSAIDs (in millions of tablets/capsules) rose from
2,836 in 1981 to 4,242 in 1993 and to 6,305 in 2000 (Fort
inflammatory drug treatment in rheumatoid arthritis. Arch Intern
J: personal communication). Thus, even if the results in
2. Fries JF, Williams CA, Bloch DA, Michel BA. NSAID-associated
our RA cohorts can be generalized, much of the decline
gastropathy: incidence and risk factor models. Am J Med 1991;91:
in incidence will have been countered by the increases in
exposure, and the estimate of more than 100,000 hospi-
3. Fries JF. The ARAMIS (American Rheumatism Association
Medical Information System) post-marketing surveillance pro-
talizations annually in the US (2) may still be relatively
current. Continued introduction and marketing of newer
4. Fries JF, Spitz PW, Williams CA, Bloch DA, Singh G, Hubert HB.
NSAIDs, even though they are safer, may increase the
A toxicity index for comparison of side effects among different
frequency of exposures to NSAIDs in the future. Migra-
drugs. Arthritis Rheum 1990;33:121–30.
5. Fries JF. ARAMIS and toxicity measurement. J Rheumatol
tion of products from prescription to over-the-counter
use may also increase exposures, although this may be
6. Fries JF, Spitz P, Kraines RG, Holman HR. Measurement of
offset by lower doses. New guidelines for use of low-dose
patient outcome in arthritis. Arthritis Rheum 1980;23:137–45.
7. Bruce B, Fries JF. The Stanford Health Assessment Question-
aspirin for cardioprotection in essentially the same pop-
naire: a review of its history, issues, progress, and documentation.
ulation as that which uses the most NSAIDs will act to
limit declines in the incidence of serious GI effects (38);
8. Fries JF, Williams CA, Bloch DA. The relative toxicity of non-
steroidal antiinflammatory drugs. Arthritis Rheum 1991;34:
low-dose aspirin use itself, even while protecting the
heart, increases the relative risk of these events by a
9. Henry D, Lim LL, Rodriguez LA, Gutthann SP, Carson JL,
Griffin M, et al. Variability in risk of gastrointestinal complications
How, then, may we continue and even accelerate
with individual non-steroidal anti-inflammatory drugs: results of acollaborative meta-analysis. Br Med J 1996;312:1563–6.
these declines? At least 5 complementary approaches
10. Silverstein FE, Faich G, Goldstein JL, Simon LS, Pincus T,
may be recommended, building on the immediate past
Whelton A, et al. Gastrointestinal toxicity with celecoxib vs
(40,41). First, we recommend even more selective use of
nonsteroidal anti-inflammatory drugs for osteoarthritis and rheu-matoid arthritis. The CLASS study: a randomized controlled trial.
NSAIDs, particularly in high-risk patients. Much of the
NSAID use is still for simple analgesia in noninflamma-
11. Bombardier C, Laine L, Reicin A, Shapiro D, Burgos-Vargas R,
tory conditions. Second, introduction of newer and safer
Davis B, et al, VIGOR Study Group. Comparison of uppergastrointestinal toxicity of rofecoxib and naproxen in patients with
agents should be continued, although, for the reasons
rheumatoid arthritis. N Engl J Med 2000;343:1520–8.
mentioned above, a limit may soon be reached. Third,
12. Singh G, Ramey DR, Triadafilopoulus G, Brown BW, Balise RR.
we recommend aggressive, continued migration of the
GI score: a simple self-assessment instrument to quantify the riskof serious NSAID-related GI complications in RA and OA
NSAID market share from more toxic to less toxic
[abstract]. Arthritis Rheum 1998;41 Suppl 9:S75.
NSAIDs. This migration so far appears relatively slight.
13. Krishnan E, Fries JF. Reduction in long-term functional disability
Fourth, use of proton-pump inhibitors for prophylaxis
in rheumatoid arthritis 1977-1998: longitudinal study of 3035patients. Am J Med 2003;115:371–6.
should be substantially increased, particularly in high-
14. Rostom A, Dube C, Wells G, Tugwell P, Welch V, Jolicouer E, et
risk patients. These drugs appear to be greatly underuti-
al. Prevention of NSAID-induced gastroduodenal ulcers. Cochran
lized and are becoming available in generic versions.
Database Syst Rev 2002;(4):CD002296.
15. Douthewaite AH, Lintott SA. Gastroscopic observation of the
However, if H antagonists are used for prevention, the
effect of aspirin and certain other substances on the stomach.
dose must be twice the standard doses, to avoid promul-
gation of a false sense of security. Systematic diagnosis
16. Sun DC, Roth SH, Mitchell CS, Englund DW. Upper gastrointes-
tinal disease in rheumatoid arthritis. Am J Dig Dis 1974;19:405–10.
and treatment of H pylori infection may have a role,
17. Levy M. Aspirin use in patients with major upper gastrointestinal
although these findings remain controversial. Fifth, the
bleeding and peptic ulcer disease. N Engl J Med 1974;290:
lowest effective dose should be used for any NSAID.
18. Roth SH, Bennett RE. Nonsteroidal anti-inflammatory drug gas-
Developments in reducing the incidence of
tropathy. Arch Intern Med 1987;147:2093–100.
NSAID gastropathy to date are gratifying. As long as
19. Armstrong CP, Blower AL. Nonsteroidal anti-inflammatory drugs
trends continue toward the use of safer NSAIDs, more
and life threatening complications of peptic ulceration. Gut 1987;28:527–32.
frequent use of proton-pump inhibitors, and de-
20. Griffin MR, Ray WA, Schaffner W. Non-steroidal anti-
escalation of dosages, particularly in high-risk patients,
inflammatory drug use and death from peptic ulcer in elderly
the trend toward reduction in the incidence of NSAID
persons. Ann Intern Med 1988;109:359–63.
21. Fries JF, Miller SR, Spitz PW, Williams CA, Hubert HB, Bloch
DA. Toward an epidemiology of gastropathy associated withNSAID use. Gastroenterology 1989;96:647–55. REFERENCES
22. Griffin MR, Piper JM, Daugherty JR, Snowden M, Ray WA.
Non-steroidal anti-inflammatory drug use and increased risk for
1. Singh G, Ramey DR, Morfeld D, Shi H, Hatoum HT, Fries JF.
peptic ulcer disease in elderly persons. Ann Intern Med 1991;114:
23. Brooks PM, Day RO. Nonsteroidal anti-inflammatory drugs:
with Helicobacter pylori infection who are taking low-dose aspirin
differences and similarities. N Engl J Med 1991;324:1716–25.
or naproxen. N Engl J Med 2001;344:967–73.
24. Roth SH, Bennett RE, Mitchell CS, Hartmann RJ. Cimetidine
32. Lai KC, Lam SK, Chu KM, Wong BC, Hui WM, Hu WH, et al.
therapy in non-steroidal anti-inflammatory drug gastropathy:
Lansoprazole for the prevention of recurrences of ulcer complica-
double-blind long-term evaluation. Arch Intern Med 1987;147:
tions from long-term low-dose aspirin use. N Engl J Med 2002;
25. Taha AS, Hudson N, Hawkey CJ, Swannell AJ, Trye PN, Cottrell
33. Langman MJ, Jensen DM, Watson DJ, Harper SE, Zhao PL,
J, et al. Famotidine for the prevention of gastric and duodenal
Quan H, et al. Adverse upper gastrointestinal effects of rofecoxib
ulcers caused by nonsteroidal antiinflammatory drugs. N Engl
compared with NSAIDs. JAMA 1999;282:1929–33.
34. Goldstein J, Agrawal NM, Silverstein F, Burr M, Verburg KM.
26. Graham D, Agrawal NM, Roth SH. Prevention of NSAID-induced
Celecoxib is associated with a significantly lower incidence ofclinically significant upper gastrointestinal (UGI) events in osteo-
gastric ulcer with misoprostol: multicentre, double-blind, placebo-
arthritis and rheumatoid arthritis patients as compared with
controlled trial. Lancet 1988;2:1277–80.
NSAIDs. Gastroenterology 1999;116:A174.
27. Silverstein F, Graham D, Senior J, Davies H, Struthers B, Bittman
35. Hoffmeister RT. Methotrexate in rheumatoid arthritis [abstract].
R, et al. Misoprostol reduces gastrointestinal complications in
patients with rheumatoid arthritis receiving non-steroidal anti-
36. Wilske KR, Healey LA. Remodeling the pyramid: a concept whose
inflammatory drugs: a randomized, double-blind, placebo-
time has come. J Rheumatol 1989;16:565–7.
controlled trial. Ann Intern Med 1995;123:241–9.
37. Fries JF. Reevaluating the therapeutic approach to rheumatoid
28. Koch M, Dezi A, Ferrario F, Capurso I. Prevention of non-
arthritis: the sawtooth strategy. J Rheumatol 1990;17:12–5.
steroidal anti-inflammatory drug-induced gastrointestinal mucosal
38. U. S. Preventive Services Task Force. Aspirin for the primary
injury: a meta-analysis of randomized controlled clinical trials.
prevention of cardiovascular events: recommendation and ration-
ale. Ann Intern Med 2002;136:157–60.
29. Yeomans ND, Tulassay Z, Juhassz L, Racz I, Howard J. A
39. Hayden M, Pignone M, Phillips C, Mulrow C. Aspirin for the
comparison of omeprazole with ranitidine for ulcers associated
primary prevention of cardiovascular events: a summary of the
with non-steroidal anti-inflammatory agents. N Engl J Med 1998;
evidence for the U.S. Preventive Services Task Force. Ann Intern
30. Food and Drug Administration, US Department of Health and
40. Lanza FL. A guideline for the treatment and prevention of
Human Services. Approved drug products with therapeutic equiv-
NSAID-induced ulcers. Am J Gastroenterol 1998;93:2037–46.
alence evaluations. Available from URL: http://www.fda.gov/cder/
41. American College of Rheumatology Subcommittee on Rheuma-
toid Arthritis Guidelines. Guidelines for the management of
31. Chan FKL, Chung S, Suen BY, Lee YT, Leung WK, Leung VK, et
rheumatoid arthritis: 2002 update. Arthritis Rheum 2002;46:
al. Preventing recurrent upper gastrointestinal bleeding in patients
(z)-4-bromo-2-((naphthalene-1-ylimino) methyl) phenolDispersive liquid-liquid microextraction followed by high-performance liquid chromatography as an efficient and sensitive technique for the simultaneous determination of alprazolam, oxazepam and diazepam Ultrasound-Assisted Emulsification Microextraction Of Oxazepam, Alprazolam And Diazepam From Urine Samples Followed By Quantification
Reply Form To: Sino Haijing Holdings Limited (the “Company”) I/We would like to receive the Corporate Communications (Note 3) of the Company in the manner as indicated below:( Please tick ONLY ONE box ) To receive Corporate Communications via the Company’s website (the “Company Website”) and to receive the notification of publication of Corporate Communications (the “
 tially explanatory variables. The average age of thepatients in the cohort increased by nearly 6 years from1981 to 1992, from 56.7 years to 62.2 years, and thenremained relatively constant thereafter. Composite GIrisk propensity scores followed a pattern of rise through1992 similar to that of the GI-related hospitalizationrates, followed by a plateau. The percentage of patientsreceiving NSAIDs declined from 87% to 76% by 1992,and thereafter remained fairly constant. Average HAQdisability index scores, on a 0–3 scale (7), rose slightly inthe first period and improved considerably in the secondperiod, which is consistent with recent findings of de-
Figure 1. Percentage of rheumatoid arthritis patients with serious
tially explanatory variables. The average age of thepatients in the cohort increased by nearly 6 years from1981 to 1992, from 56.7 years to 62.2 years, and thenremained relatively constant thereafter. Composite GIrisk propensity scores followed a pattern of rise through1992 similar to that of the GI-related hospitalizationrates, followed by a plateau. The percentage of patientsreceiving NSAIDs declined from 87% to 76% by 1992,and thereafter remained fairly constant. Average HAQdisability index scores, on a 0–3 scale (7), rose slightly inthe first period and improved considerably in the secondperiod, which is consistent with recent findings of de-
Figure 1. Percentage of rheumatoid arthritis patients with serious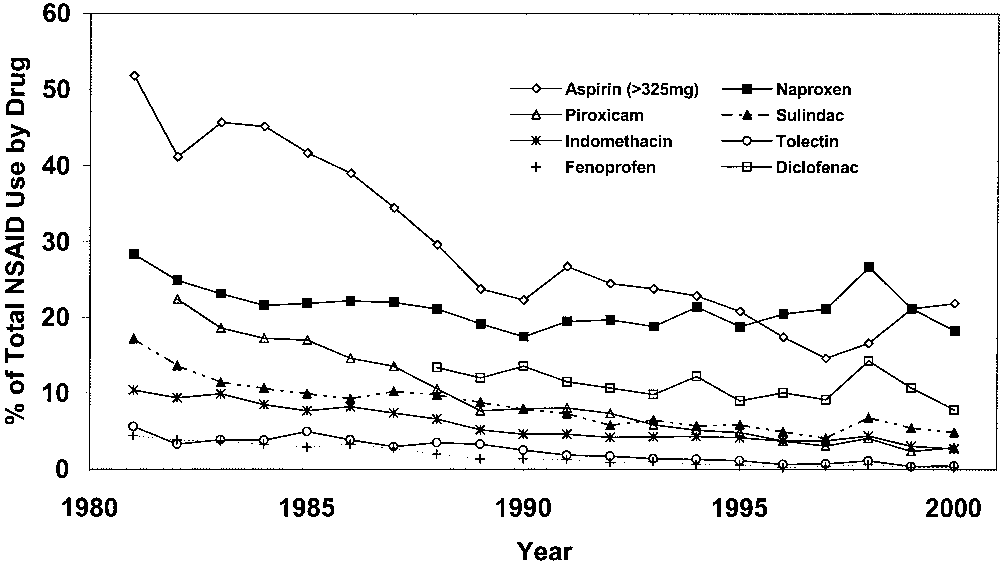
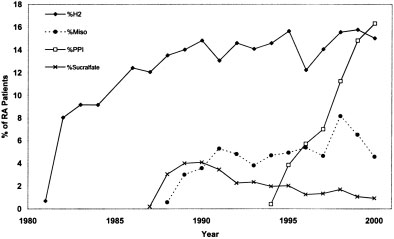
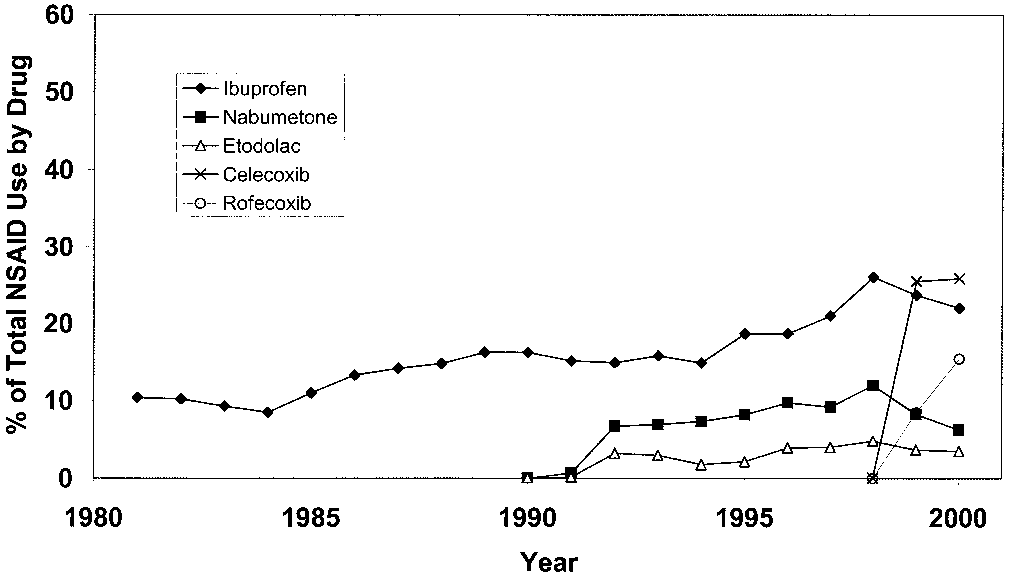 Figure 2. Percentage of use of those drugs with increased usage over
Figure 2. Percentage of use of those drugs with increased usage over