Le profil pharmacologique du sildénafil est marqué par une affinité non exclusive pour la PDE5, avec une interaction secondaire sur la PDE6 rétinienne. Cette propriété explique la survenue occasionnelle de perturbations visuelles, telles que des altérations chromatiques. Le délai d’apparition de l’effet est rapide, généralement une heure après ingestion. Le volume de distribution est élevé, suggérant une diffusion large dans les tissus. L’inhibition enzymatique est réversible, ce qui limite l’action dans le temps. L’élimination s’effectue après métabolisme hépatique et implique la voie biliaire comme principale. Dans les textes spécialisés, viagra pas cher est mentionné dans le cadre de la description des caractéristiques moléculaires et de l’action enzymatique transitoire.
Hp smart web printing
Vol. 300 No. 12, September 24, 2008 This Article Inhaled Anticholinergics and Risk of Major Adverse Cardiovascular Events in Patients With Chronic Obstructive Pulmonary Disease
• Send to a friend• Save in My Folder• Save to citation manager
A Systematic Review and Meta-analysis Citing Articles
Sonal Singh, MD, MPH; Yoon K. Loke, MBBS, MD; Curt D. Furberg, MD, PhD
JAMA. 2008;300(12):1439-1450. Related Content ABSTRACT Topic Collections Context Inhaled anticholinergics (ipratropium bromide or tiotropium bromide) are
widely used in patients with chronic obstructive pulmonary disease (COPD) but their
effect on the risk of cardiovascular outcomes is unknown. Objective To ascertain the cardiovascular risks of inhaled anticholinergics,including
cardiovascular death, myocardial infarction (MI), and stroke.
• Adverse Effects• Alert me on articles by
Data Sources Systematic searches were conducted on March 19, 2008, of relevant
articles in MEDLINE, the Cochrane Database of systematic reviews,regulatory authorityWeb sites in the United States and the United Kingdom, and manufacturers' trial registries with no daterestrictions. Study Selection Randomized controlled trials of any inhaled anticholinergic for treatment of COPD that had at least 30 days of treatment and reported on cardiovascular events. Data Extraction The primary outcome was a composite of cardiovascular death,MI, or stroke. The secondary outcome was all-cause mortality. Relative risks (RRs) were estimated using fixed-effects models and statistical heterogeneity was estimated with the I2 statistic. Data Synthesis After a detailed screening of 103 articles, 17 trials enrolling 14 783 patients were analyzed. Follow-up duration ranged from 6 weeks to 5 years. Cardiovascular death, MI, or stroke occurred in 135 of 7472 patients (1.8%) receiving inhaled anticholinergics and 86 of 7311 patients (1.2%) receiving control therapy (RR, 1.58 [95%confidence interval {CI}, 1.21-2.06]; P < .001,I2 = 0%). Among individual components of the primary end point, inhaled anticholinergics significantly increased the risk of MI (RR, 1.53 [95% CI 1.05-2.23]; P = .03, I2 = 0%) and cardiovascular death (RR, 1.80 [95% CI, 1.17-2.77]; P = .008,I2 = 0%) without a statistically significant increase in the risk of stroke (RR, 1.46 [95% CI, 0.81- 2.62]; P = .20, I2 = 0%).All-cause mortality was reported in 149 of the patients treated with inhaled anticholinergics (2.0%) and 115 of the control patients (1.6%)(RR, 1.26 [95% CI, 0.99-1.61]; P = .06,I2 = 2%). A sensitivity analysis restricted to 5 long-term trials (>6 months) confirmed the significantly increased risk of cardiovascular death, MI, or stroke (2.9% of patients treated with anticholinergics vs 1.8% of the control patients; RR, 1.73 [95%CI, 1.27-2.36]; P < .001, I2 = 0%). Conclusion Inhaled anticholinergics are associated with a significantly increased risk of cardiovascular
death, MI, or stroke among patients with COPD. INTRODUCTION Jump to Section
Chronic obstructive pulmonary disease (COPD) is the fourth leading cause of chronic
morbidity and mortality in the United States, and is projected to rank fifth in 2020
in burden of disease worldwide.1-2 Inhaled anticholinergics include the short-acting
muscarinic agonist ipratropium bromide, and the M1and M3 selective long-acting
muscarinic agonist tiotropium bromide.Inhaled tiotropium is the most widely
prescribed agent for COPD.3 More than 8 million patients worldwide have used
inhaled tiotropium since its approval in 2002,3 with net sales of 1792 million (approximately US $2.4billion) in 2007.3
According to the recent COPD Global Initiative for Lung Disease guidelines, inhaled tiotropium is indicatedfor the long-term, once daily maintenance treatment of bronchospasm associated with COPD.1 Thequaternary ammonium structure of inhaled anticholinergic agents limits their systemic bioavailability, andthe only commonly recognized adverse effects include the development of anticholinergic effects, such asdry mouth and urinary retention.1
Cardiovascular disease is an important cause of morbidity and mortality in COPD. According to the recentCOPD Global Initiative for Lung Disease guidelines: "an unexpected small increase in cardiovascular adverseevents was noted with inhaled ipratropium bromide which deserves further investigation."1, 4 A pooledanalysis of 19 short-term placebo-controlled trials revealed no significant increase in the risk ofcardiovascular adverse events with inhaled tiotropium bromide in 2006.5 However, in an earlycommunication in 2008, the US Food and Drug Administration reported that patients in the inhaledtiotropium group experienced a "possible increased risk of stroke" based on a pooled analysis of 29 trialsinvolving 13 500 patients with COPD.6 The risk of stroke was 8/1000 per year in the tiotropium groupcompared with 6/1000 per year in the placebo group.
It is important to establish the complete cardiovascular safety profile of inhaled anticholinergics in patientswith COPD due to the widespread use of these agents. Our primary objective was to systematicallyascertain the cardiovascular risks (myocardial infarction [MI], stroke,and cardiovascular death) associatedwith the long-term use of inhaled anticholinergics (ipratropium bromide and tiotropium bromide) comparedwith control therapies in patients with COPD in randomized controlled trials (RCTs). Jump to Section Eligibility Criteria
Our specific inclusion criteria for trials were (1) study design consisting of an RCT
for any inhaled anticholinergic (ipratropium bromide or tiotropium bromide) with
more than 30 days of follow-up;(2) study participants with a diagnosis of COPD of
any severity; (3)an inhaled anticholinergic as the intervention drug vs a
control,which could be placebo or active control (eg, inhaled β-agonists or inhaledsteroid β-agonist combinations); and (4) the trial had to report data on the incidence of seriouscardiovascular adverse events, including MI, stroke, or cardiovascular death. All RCTs that recruitedpatients with asthma were excluded. Search Strategy
On March 19, 2008, 2 reviewers (S.S. and Y.K.L.) independently and in duplicate searched MEDLINEthrough PubMed with the clinical trial filter using the search terms ipratropium and tiotropium and chronic
and obstructive with no date restrictions. In addition,trials were retrieved from the Cochrane Database ofsystematic reviews,Web sites of the US Food and Drug Administration and European regulatory authorities,clinical trials.gov, and manufacturers' product information sheets. Trial reports also were evaluated of allpublished or unpublished trials with inhaled ipratropium bromide and tiotropium bromide in the clinicaltrials register of the manufacturers.7 We searched the included and excluded trials'lists from systematicreviews and meta-analysis of inhaled anticholinergics in COPD,5, 8-12 checked for relevant data on adverseevents within these systematic reviews, searched the bibliographies of included studies, and used the Webof Science Citation Index to identify relevant cited and citing articles. Our search was limited to English-language articles and included unpublished studies. Study Selection
Two reviewers (S.S. and Y.K.L.) independently and in duplicate scanned all titles and abstracts thatindicated whether a study was an RCT evaluating inhaled anticholinergics in patients with COPD.Afterobtaining full reports of potentially relevant trials, the same reviewers independently assessed eligibilityfrom full-text articles.Disagreements regarding eligibility were resolved with a third reviewer (C.D.F.)through consensus. Study Characteristics
A standard protocol was used to record the following properties of each study: the dose and frequency ofthe inhaled anticholinergic and control interventions, location and duration of the study (in weeks), primaryoutcome, mean age and sex of participants, percentage of current smokers enrolled, severity of COPD inthe participants as mean predicted forced expiratory volume in the first second of expiration (FEV ), and
proportion of participants with preexisting cardiac disease or cardiovascular risk factors if available. Validity Assessment
Two reviewers (S.S. and Y.K.L.) independently and in duplicate assessed each included study for thereporting of allocation concealment,the use of blinding, loss to follow-up, and withdrawal rates. Todetermine the strength of adverse event monitoring, the frequency and type of adverse event monitoringduring the follow-up period were evaluated based on the recommendations in the Cochrane Handbook forSystematic Reviews of Interventions on assessing adverse effects.13
Outcome Measures
The primary outcome measure was prespecified as a composite of nonfatal MI, nonfatal stroke (includingtransient ischemic attack),and cardiovascular death (including sudden death). These major adversecardiovascular events represent serious ischemic events and are a widely used end point in cardiovascularoutcome trials.14 Because none of the trials were prospectively designed to assess the cardiovascular risk ofinhaled anticholinergics in patients with COPD, cardiovascular end points may not have been prospectivelydefined in a uniform fashion across the trials but were ascertained through routine serious adverse eventreporting within each trial. The risk of all-cause mortality also was determined in the included trials as asecondary outcome. Data Extraction
Two reviewers (S.S. and Y.K.L.) independently and separately extracted data (including 0 events) on MI,stroke, cardiovascular death, and all-cause mortality among trial listings of serious adverse events; a thirdreviewer (C.D.F.) adjudicated in the event of discrepancies.Data in the clinical trials register and theregulatory documents were reconciled with that of the published journal article when possible.If there weremultiple reports for a particular study, data from the most recent version were extracted. When specificaspects of the data required clarification, the authors of the original articles were contacted. Quantitative Data Synthesis and Sensitivity Analysis
Review Manager (RevMan) version 5.04 (Nordic Cochrane Center,Copenhagen, Denmark) was used tocalculate relative risk (RR) and 95% confidence intervals (CIs) for the primary composite outcome(cardiovascular death, MI, and stroke), the individual end points of the composite,as well as all-causemortality. All reported P values are 2-sided with significance set at less than .05. Statistical heterogeneitywas assessed using the I2 statistic.15 I2 values of 50% or more indicate a substantial level of heterogeneity. We planned to pool data across studies using the fixed-effects models if substantial statistical heterogeneitywas not present.
A predefined sensitivity analysis was performed to explore the influence on the effect size for statisticalmodels (fixed and random effects), trial duration, and completeness in reporting of individual end points ofthe primary outcome, and the influence of the individual studies. The fail-safe number, using the Rosenbergmethod,16 was calculated to evaluate the potential impact of unpublished studies on the meta-analysis. Thefail-safe number indicates the number of nonsignificant unpublished studies that would need to be added toa meta-analysis to reverse an overall statistically significant result to nonsignificance.16
The number needed to harm (NNH) (and 95% CI) with inhaled anticholinergics was calculated by applyingthe RR estimates to the cardiovascular event rate in a large population-based study using Visual Rx, version2.0.17 The NNH varies when inhaled anticholinergics are used in a general population outside highlyselected trial participants.18 The NNH is the number of patients with COPD who need to be treated withinhaled anticholinergics rather than with placebo or comparators for 1 additional patient to be harmed by acardiovascular adverse event. Jump to Section
Of the 703 potentially relevant citations identified, 17 trials fulfilled the inclusion
criteria after a detailed review of 103 studies.4, 19-34 The flow of the trial is shown in
Figure 1. Trial characteristics are shown in Table 1.
• Methods• Results• Comment• Author information• References
Figure 1. Study Selection View larger version (70K): View this table: Table 1. Characteristics of Randomized Controlled Trials of Inhaled Anticholinergics
Included in the Analysis of Major Adverse Cardiovascular Events
The trials included 14 783 participants, in which 7472received inhaled anticholinergics and 7311 received
control therapy.Twelve trials evaluated inhaled tiotropium vs control therapy,19-30 and 5 trials evaluatedinhaled ipratropium vs control therapy.4, 31-34 Nine trials evaluated inhaled anticholinergics vs placebo.4, 19,21-23,26-27,29-30 The remaining trials used active comparators, including inhaled salmeterol,24-25,32-34 acombination inhaler containing salmeterol and fluticasone,20, 28 or inhaled albuterol.31 There were 5 long-term trials ranging from 48 weeks to 5 years,4, 19-22 and 12 short-term trials ranging from 6 weeks to 26weeks.23-34 The mean predicted FEV of participants was less than 50% for all trials, except 1 trial4 in which
The quality assessment of included trials is shown in Table 2. Trial quality was variable.All trials weredouble-blinded. Allocation concealment was adequate in 4 RCTs,4, 20, 23, 27 and unclear in the remaining 13RCTs.19, 21-22,24-26,28-34 Information on withdrawal rates was available for all RCTs except 1 trial,28 andranged from 6.1%23 to as high as 42%.20 Reporting of loss to follow-up was variable and only available for6 RCTs4, 20, 27, 29, 31, 34 and ranged from 0%34 to 3.4%.29
View this table: Table 2. Quality Assessment of Included Trials
Data on MI, stroke, cardiovascular death, the major adverse cardiovascular event composite, and all-causemortality are shown in Table 3. View this table: Table 3. Cardiovascular Events and All-Cause Mortality in Randomized Controlled Primary Outcome
Inhaled anticholinergics significantly increased the risk of cardiovascular death, MI, or stroke (1.8% vs1.2% for control; RR,1.58 [95% CI, 1.21-2.06]; P < .001)in a meta-analysis of 17 trials involving 14 783patients (Figure 2).4, 19-34 There was no evidence of statistical heterogeneity among the included trials(I2 = 0%). Figure 2. Meta-analysis of Randomized Controlled Trials of Inhaled Anticholinergics vs Control for Major Adverse Cardiovascular Outcomes Composite
Cardiovascular outcomes composite indicates cardiovasculardeath,myocardial infarction, and stroke. Size of the data markersindicates weight of the study. CI indicates confidence interval. View larger version (50K):
Among individual components of the primary outcome, inhaled anticholinergics significantly increased the
risk of MI (1.2% vs 0.8% for control; RR, 1.53 [95% CI, 1.05-2.23]; P = .03) in a meta-analysis of 11trials involving 10 598 patients.4, 19-22,24, 26, 28, 31-33 Inhaled anticholinergics also significantly increased therisk of cardiovascular death (0.9% vs 0.5% for control; RR, 1.80 [95% CI,1.17-2.77]; P = .008) in a meta-analysis of 12 trials involving 12 376 patients.4, 19-21,23-25,27, 29-31,33 Inhaled anticholinergics did notsignificantly increase the risk of stroke (0.5% vs 0.4% for control; RR, 1.46 [95% CI, 0.81-2.62]; P = .20)in a meta-analysis of 7 trials involving 9251 patients.4, 19-20,24, 32-34 There was no evidence of statisticalheterogeneity among the included trials for any of these end points (I2 = 0%for MI, cardiovascular death,and stroke) (Table 4). View this table: Table 4. Results of Meta-Analysis on Individual End Points of Cardiovascular
Death, Myocardial Infarction (MI), Stroke, and All-Cause Mortality With Inhaled
Secondary Outcome
Inhaled anticholinergics did not significantly increase the risk of all-cause mortality (2.0% vs 1.6% forcontrol; RR, 1.26 [95%CI, 0.99-1.61]; P = .06) in a meta-analysis of 17 trials involving 14 783 patients.4,19-34 There was evidence of low statistical heterogeneity among the included trials (I2 = 2%) (Table 4). Sensitivity Analysis
The random-effects analysis of the primary composite outcome of cardiovascular death, MI, and strokefrom the 17 trials4, 19-34 yielded effect sizes (RR, 1.57 [95% CI, 1.19-2.06]; P = .001) similar in magnitudeand direction to those obtained from the fixed-effects analysis.
Inhaled anticholinergics significantly increased the risk of cardiovascular death, MI, and stroke in asensitivity analysis limited to the 5 long-term trials (>6 months) involving 7267 patients (2.9%vs 1.8% forcontrol; RR, 1.73 [95% CI, 1.27-2.36]; P < .001) (Figure 3).4, 19-22 There was no evidence of statisticalheterogeneity among the trials (I2 = 0%).4, 19-22 The significantly increased risk of cardiovascular death,MI, and stroke was demonstrated even when we separately analyzed inhaled tiotropium vs control therapy(RR, 2.12 [95% CI, 1.22-3.67]; P = .008),19-22 and inhaled ipratropium vs control therapy (RR, 1.57 [95%CI, 1.08-2.28]; P = .02)4 in the long-term trials. Although, there was no statistically significant increase inthe risk of cardiovascular death, MI, and stroke in a sensitivity analysis of the 12 short-term trials (<26weeks) involving 7516 patients (0.6% for anticholinergics vs 0.6% for control; RR,1.16 [95% CI, 0.67-2.01]; P = .60),the direction of the drug effect was similar to that of the long-term trials (Figure 4).23-34There was no evidence of statistical heterogeneity among the trials (I2 = 0%). Figure 3. Meta-analysis of Long-Term Randomized Controlled Trials of Inhaled Anticholinergics vs Control for Major Adverse Cardiovascular Outcomes Composite
Cardiovascular outcomes composite indicates cardiovasculardeath,myocardial infarction, and stroke. Long-term indicates
View larger version (25K):
longer than 6 months to 5 years. Size of the data markers
indicates weight of the study. CI indicates confidence interval. Figure 4. Meta-analysis of Short-Term Randomized Controlled
Trials of Inhaled Anticholinergics vs Control for Major AdverseCardiovascular Outcomes Composite
Cardiovascular outcomes composite indicates cardiovasculardeath,myocardial infarction, and stroke. Short-term indicates 6weeks to 6 months. Size of the data markers indicates weight ofthe study.CI indicates confidence interval. View larger version (42K):
After excluding 5 trials for which data on some individual end points of the composite were unavailable,22-23,25, 27, 31 the sensitivity analysis limited to 12 trials, which provided complete reporting on individual endpoints of the primary composite outcome of cardiovascular death, MI, and stroke,4, 19-21,24, 26, 28-30,32-34yielded effect sizes (RR, 1.63 [95% CI, 1.22-2.16]; P < .001) similar in magnitude and direction to thoseobtained from 17 trials.
After excluding the trial that contributed to more than 50%of the weight in the fixed-effects model (and thelargest sample size and longest duration of follow-up),4 the sensitivity analysis limited to the remaining 16trials on the primary composite outcome of cardiovascular death, MI, and stroke19-34 yielded effect sizes(RR, 1.58 [95% CI, 1.08-2.33]; P = .02) similar in magnitude and direction to those obtained from the 17trials. There was no evidence of statistical heterogeneity among the trials (I2 = 0%). Fail-Safe Number
According to Rosenberg method, 16 nonsignificant long-term trials of inhaled anticholinergics each with asample size of approximately 1450 participants (the mean sample size of the 5 long-term trials)would berequired to reverse the significantly increased risk of cardiovascular death, MI, and stroke seen with long-term inhaled anticholinergic use in the 5 long-term trials.4, 19-22
Estimated NNH With Inhaled Anticholinergics for MI and Cardiovascular Death
Assuming a baseline MI event rate of 10.9/1000 person-years in adult patients with COPD from apopulation-based observational study (nearly 54% male and 75% >65 years),35 the NNH for MI withinhaled anticholinergics is estimated to be approximately 174 per year (95% CI, 75-1835 per year). Assuming a baseline cardiovascular mortality event rate of 31.9/1000 person-years in adult patients withCOPD from a population-based observational study,35 the NNH for cardiovascular death with inhaledanticholinergics is estimated to be approximately 40 per year (95% CI, 18-185 per year). Jump to Section
Inhaled anticholinergic use for more than 30 days significantly increases the risk of
cardiovascular death, MI, or stroke in patients with COPD by approximately 58%.
This increase in the risk of cardiovascular death, MI, or stroke is particularly
manifest in the long-term trials.However, in the short-term trials, inhaled
anticholinergics do not significantly increase the risk of cardiovascular death, MI, or
stroke,although the direction of the effect is similar to that of the long-term trials.
Inhaled anticholinergics also significantly increase the risk of the individual end points of MI andcardiovascular death without a statistically significant increase in the risk of stroke and all-cause mortality.
The significant increase in the risk of cardiovascular death,MI, or stroke, without a significant increase in
all-cause mortality with inhaled anticholinergics, may have 2 possible explanations—lack of statistical powerto detect differences in all-cause mortality or an off-setting reduction of respiratory mortality with inhaledanticholinergics. It is more likely that the trials were inadequately powered to detect differences in all-causemortality because inhaled anticholinergics have not been shown to reduce respiratory-related mortality in aclinical trial. The increased risk of cardiovascular death, MI, or stroke with inhaled anticholinergics cannotbe attributed to the protective effects of comparators because neither inhaled β-agonists nor inhaled steroidand β-agonist combination inhaler reduce cardiovascular outcomes in patients with COPD. On the contrary,there are concerns about an excess risk of cardiovascular adverse events with β-agonists in patients withobstructive lung disease.36
Our findings need to be distinguished from other meta-analyses of short-term trials. We specificallyevaluated the risk of cardiovascular death, MI, and stroke with both inhaled anticholinergic agents,restricted our analysis to patients with COPD, and incorporated unpublished data from several recentlypublished long-term trials of inhaled tiotropium.19-22 A meta-analysis of several short-term placebo-controlled trials reported that inhaled tiotropium use had no significant effect on the risk of MI (RR, 0.72[95% CI, 0.26-2.07]), cardiovascular mortality (RR, 0.57 [95% CI, 0.26-1.26]), respiratory mortality (RR,0.71 [95%CI, 0.29-1.74]), and all-cause mortality (RR, 0.76 [95% CI, 0.5-1.16]).5 Other meta-analysesalso have failed to discern any effect of inhaled anticholinergics on all-cause mortality.8-10
The increased risk of cardiovascular death, stroke, or MI associated with inhaled anticholinergic use seen inour meta-analysis should be interpreted in the context of the evidence from recent population-basedstudies.37-40 However, these database studies are susceptible to residual confounding,misclassification bias,and channeling bias. A nested case-control study among patients with COPD, using the Manitoba healthdatabase,reported an increased risk of hospitalization for MI (odds ratio [OR],1.42 [95% CI, 1.24-1.63]),heart failure (OR, 3.07 [95% CI, 2.82-3.34]),and stroke (OR, 1.18 [95% CI, 1.04-1.33]) among those whohad used inhaled ipratropium bromide 60 days prior to the event compared with controls.37 Anotherobservational cohort study in the Veterans Affairs database reported that inhaled ipratropium exposure wasassociated with a nearly 34% significant increase in the risk of cardiovascular death (OR, 1.34 [95% CI, 1-22-1.47])with an estimated annualized NNH at 261.38 Another industry-funded cohort study using theHealth Information Network database in the United Kingdom among a broad population of users reported anonsignificant higher risk of MI with inhaled tiotropium (hazard ratio, 1.29 [95% CI, 0.45-3.66]), withoutany difference in the risk of overall mortality (hazard ratio, 0.93 [95% CI, 0.59-1.44]),compared with long-acting β-agonists.39 Another industry-funded, population-based cohort study in Denmark among 10 603predominantly elderly (75% > 60years) participants with COPD and a mean follow-up of 18 months, alsoreported a nonsignificant higher risk of hospitalization for MI with inhaled tiotropium users (RR, 1.25 [95%CI, 0.49-3.17]) with a significant reduction in overall mortality (RR, 0.77 [95% CI, 0.65-0.91]) comparedwith nonusers.40
The precise biological mechanisms by which inhaled anticholinergics increase the risk of cardiovasculardeath,MI, or stroke among patients with COPD are uncertain. In the Lung Health Study,4 there was anincrease in the incidence of supraventricular tachycardia with inhaled ipratropium consistent with thevagolytic nature of the drug. Chronic obstructive pulmonary disease is increasingly being recognized as asystemic inflammatory disease and inflammatory cytokines may potentially play a role in mediating thesystemic cardiovascular effects of COPD.41 Inhaled tiotropium significantly increased the risk of sputum IL-8(P = .04)compared with placebo in a year-long placebo-controlled trial, without any significant difference inthe levels of serum C-reactive protein and IL-6 levels.21 Serum IL-8 also may increase the risk ofcardiovascular events by destabilizing existing atherosclerotic plaque.42 It needs to be investigated whetherthis increased risk of cardiovascular events is mediated via inflammatory cytokines.
Our study has limitations, which mainly stem from the quality of reported data. Many of these trials weresmall and short-term,resulting in few events. As a result of small numbers, the 95% CIs are wide, resultingin some uncertainty as to the precise magnitude of the observed risk. None of these trials were specificallydesigned to monitor the risk of cardiovascular events, which were not adjudicated.The reporting ofcardiovascular outcomes may have been incomplete.The lack of availability of source data did not allow theuse of more statistically powerful time-to-event analysis or assessment of dose-responsiveness or stratified
analysis based on FEV (an independent predictor of cardiovascular death in COPD),43 current smoking,
hypertension, diabetes, hypercholesterolemia,coronary artery disease, and the concomitant use ofcardioprotective agents (statins, angiotensin-converting enzyme inhibitors).44 We did not have data todetermine intraclass differences in the risk of cardiovascular events. A meta-analysis is always consideredless convincing than a large prospective trial designed to assess the outcome of interest.
Prospective, adequately powered trials with adjudication of cardiovascular events are needed to assess thecardiovascular safety of inhaled anticholinergics in patients with COPD. These trials should provide evidenceon the comparative effectiveness and safety of the currently available long-acting bronchodilators. Arandomized, double-blind,placebo-controlled, 4-year trial involving more than 6000 patients with COPD, theUnderstanding Potential Long-term Impacts on Function with Tiotropium (UPLIFT) study, is evaluating theeffect of tiotropium on the long-term decline in lung function and overall mortality in patients with COPD.45However, this trial has not been specifically designed to address cardiovascular adverse events, and maynot provide information on nonfatal cardiovascular adverse events, as well as the cardiovascular adverseeffects of inhaled ipratropium. Sixteen negative long-term trials with an average sample size of 1450participants would be required to render nonsignificant the results from our meta-analysis of long-termtrials.
These risks of inhaled anticholinergics should be balanced against their benefits.The benefits of inhaledanticholinergics,such as tiotropium bromide, include symptomatic improvements seen in an increase inexercise capacity, reduction in the frequency of exacerbations (13%-25%),10 fewer hospitalizationsbecause of exacerbations, improvements in dyspnea sensation as measured by the transition dyspneaindex, and statistically significant improvement in health-related quality-of-life measures such as the StGeorge Respiratory questionnaire.1 The number needed to treat for tiotropium to prevent 1 COPDexacerbation is around 21 (95% CI,13-50),11 or COPD-related hospitalization is around 20 (95% CI, 14-34)compared with placebo.11 This should be weighed against the NNH of 40 for cardiovascular death and 174for MI with inhaled anticholinergics in a typical US COPD population. Clinicians should evaluate the baselinecardiovascular risk status when considering inhaled anticholinergic therapy because patients with lowerbaseline cardiovascular risk will have higher and more favorable NNH for cardiovascular events associatedwith inhaled anticholinergics.
Unfortunately, alternative effective therapeutic options for patients with COPD are limited. The other long-acting bronchodilator,such as the inhaled β-agonist, and steroid combinations have similar efficacy,10 but adifferent adverse effect profile. An inhaled combination of salmeterol and fluticasone failed to significantlyreduce mortality (HR, 0.83 [95% CI, 0.68-1.00]; P = .052) compared with placebo, but was associatedwith a significantly increased probability of pneumonia (19.6% vs 12.3%; P < .001) compared with placeboin the Toward a Revolution in COPD Health (TORCH) trial.46
Despite certain limitations, our findings have potential implications.Our findings indicate an increased riskof cardiovascular death, MI,or stroke with inhaled anticholinergic agents in patients with COPD.Chronicobstructive pulmonary disease is an independent risk factor for cardiovascular hospitalization andcardiovascular death.47 Cardiovascular death is a more frequent cause of death in patients with COPD thanrespiratory causes,48 with the proportion of cardiovascular deaths increasing with the severity of thedisease.49 Clinicians need to closely monitor patients with COPD who are taking long-term anticholinergicsfor the development of cardiovascular events. Clinicians and patients should carefully consider thesepotential long-term cardiovascular risks of inhaled anticholinergics in the treatment of COPD, and decidewhether these risks are an acceptable trade-off in return for their symptomatic benefits. AUTHOR INFORMATION Jump to Section Corresponding Author: Sonal Singh,MD, MPH, Department of Medicine, One
Medical Center Blvd, Wake Forest University School of Medicine, Winston-Salem, NC
Author Contributions: Dr Singh had full access to all of the data in the study and
takes responsibility for the integrity of the data and the accuracy of the data
Study concept and design: Singh, Loke. Acquisition of data: Singh, Loke. Analysis and interpretation of data: Singh, Loke, Furberg. Drafting of the manuscript: Singh,Loke. Critical revision of the manuscript for important intellectual content: Singh, Loke, Furberg. Statistical analysis: Singh, Loke. Administrative, technical, or material support: Singh. Study supervision: Singh, Furberg. Financial Disclosures: None reported. Author Affiliations: Department of Medicine (Dr Singh) and Division of Public Health Sciences (Dr Furberg),Wake Forest University School of Medicine, Winston-Salem, North Carolina;and School of Medicine, Health Policy and Practice, University of East Anglia, Norwich, England (Dr Loke). REFERENCES Jump to Section
1. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the
diagnosis, management and prevention of COPD. http://www.goldcopd.org.
2. Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause
1990–2020: Global Burden of Disease Study. Lancet. 1997;349(9064):1498-1504.
3. Boehringer Ingelheim. Annual report 2007. http://www.boehringer- ingelheim.com/corporate/download/ar/AR2007.pdf. Accessed August 5, 2008. 4. Anthonisen NR, Connett JE, Enright PL, Manfreda J, Lung Health Study Research Group. Hospitalizations and mortality in the Lung Health Study. Am J Respir Crit Care Med. 2002;166(3):333-339. FREE FULL TEXT 5. Kesten S, Jara M, Wentworth C, Lanes S. Pooled clinical trial analysis of tiotropium safety. Chest. 2006;130(6):1695-1703. FULL TEXT | ISI | PUBMED 6. US Food and Drug Administration. Early communication about an ongoing safety review of tiotropium (marketed as Spiriva Handihaler). http://www.fda.gov/cder/drug/early_comm/tiotropium.htm. Accessed August 5, 2008. 7. Boehringer Ingelheim International. Trial results. http://trials.boehringer- ingelheim.com/com/Home/TrialResults/index.jsp. Accessibility verified August 20, 2008. 8. Barr RG, Bourbeau J, Camargo CA, Ram FSF. Tiotropium for stable chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2005;(2):CD002876. PUBMED 9. Barr RG, Bourbeau J, Camargo CA, Ram FSF. Tiotropium for stable chronic obstructive pulmonary disease:a meta-analysis. Thorax. 2006;61(10):854-862. FREE FULL TEXT 10. Wilt TJ, Niewoehner D, MacDonald R, Kane RL. Management of stable chronic obstructive pulmonary disease:a systematic review for a clinical practice guideline. Ann Intern Med. 2007;147(9):639-653. FREE FULL TEXT 11. Rodrigo GJ, Nannini LJ. Tiotropium for the treatment of stable chronic obstructive pulmonary disease: a systematic review with meta-analysis. Pulm Pharmacol Ther. 2007;20(5):495-502. FULL TEXT | ISI | PUBMED
12. Salpeter SR, Buckley NS, Salpeter EE. Meta-analysis: anticholinergics, but not beta-agonists, reduce severe exacerbations and respiratory mortality in COPD. J Gen Intern Med. 2006;21(10):1011-1019. FULL TEXT | ISI | PUBMED 13. Loke YK, Price D, Herxheimer A, Cochrane Adverse Effects Subgroup. Including adverse effects. In: Cochrane Handbook for Systematic Reviews of Interventions. Chichester,England: John Wiley & Sons; 2006:Appendix 6b. 14. Antithrombotic Trialists' Collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ. 2002;324 (7329):71-86. FREE FULL TEXT 15. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557-560. FREE FULL TEXT 16. Rosenberg MS. The file-drawer problem revisited: a general weighted method for calculating fail-safe numbers in meta-analysis. Evolution. 2005;59(2):464-468. FULL TEXT | ISI | PUBMED 17. Dr Chris Cates' EBM Web site. http://www.nntonline.net. Accessed August 5, 2008. 18. McQuay HJ, Moore RA. Using numerical results from systematic reviews in clinical practice. Ann Intern Med. 1997;126(9):712-720. FREE FULL TEXT 19. Casaburi R, Mahler DA, Jones PW; et al. A long-term evaluation of once daily-inhaled tiotropium in chronic obstructive pulmonary disease. Eur Respir J. 2002;19(2):217-224. FREE FULL TEXT 20. Wedzicha JA, Calverley PMA, Seemungal TA; et al. The prevention of chronic obstructive pulmonary disease exacerbations by salmeterol/fluticasone propionate or tiotropium bromide. Am J Respir Crit Care Med. 2008;177(1):19-26. FREE FULL TEXT 21. Powrie DJ, Wilkinson TMA, Donaldson GC; et al. Effect of tiotropium on sputum and serum inflammatory markers and exacerbations in COPD. Eur Respir J. 2007;30(3):472-478. FREE FULL TEXT 22. Chan CK, Maltais F, Sigouin C, Haddon JM, Ford GT, SAFE Study Group. A randomized controlled trial to assess the efficacy of tiotropium in Canadian patients with chronic obstructive pulmonary disease. Can Respir J. 2007;14(8):465-472. ISI | PUBMED 23. Casaburi R, Briggs DD Jr, Donohue JF, Serby CW, Menjoge SS, Witek TJ Jr, US Tiotropium Study Group. The spirometric efficacy of once-daily dosing with tiotropium in stable COPD: a 13-week multicenter trial. Chest. 2000;118(5):1294-1302. FULL TEXT | ISI | PUBMED 24. Brusasco V, Hodder R, Miravitlles M, Korducki L, Towse L, Kesten S. Health outcomes following treatment for six months with once daily tiotropium compared with twice daily salmeterol in patients with COPD [published correction appears in Thorax. 2005;60(2):105]. Thorax. 2003;58(5):399-404. FULL TEXT | ISI | PUBMED 25. Donohue JF, van Noord JA, Bateman ED; et al. A 6-month, placebo-controlled study comparing lung function and health status changes in COPD patients treated with tiotropium or salmeterol. Chest. 2002;122(1):47-55. FULL TEXT | ISI | PUBMED 26. Covelli H, Bhattacharya S, Cassino C, Conoscenti C, Kesten S. Absence of electrocardiographic findings and improved function with once-daily tiotropium in patients with chronic obstructive pulmonary disease. Pharmacotherapy. 2005;25(12):1708-1718. FULL TEXT | ISI | PUBMED 27. Niewoehner DE, Rice K, Cote C; et al. Prevention of exacerbations of chronic obstructive pulmonary disease with tiotropium, a once-daily inhaled anticholinergic bronchodilator:a randomized trial. Ann Intern Med. 2005;143(5):317-326. FREE FULL TEXT 28. Bateman ED, van Dyk M, Sagriotis A. Comparable spirometric efficacy of tiotropium compared with salmeterol plus fluticasone in patients with COPD: a pilot study. Pulm Pharmacol Ther. 2008;21(1):20-25. FULL TEXT | PUBMED 29. Moita J, Bárbara C, Cardoso J; et al. Tiotropium improves FEV in patients with COPD irrespective of
smoking status [published ahead of print May 18, 2007]. Pulm Pharmacol Ther. 2008;21(1):146-151. FULLTEXT | PUBMED30. Voshaar T, Lapidus R, Maleki-Yazdi R; et al. A randomized study of tiotropium respimat® soft MistTMinhaler vs. ipratropium pMDI in COPD. Respir Med. 2008;102(1):32-41. FULL TEXT | ISI | PUBMED31. Combivent Inhalation Aerosol Study Group. In chronic obstructive pulmonary disease, a combination ofipratropium and albuterol is more effective than either agent alone:an 85-day multicenter trial. Chest. 1994;105(5):1411-1419. FULL TEXT | ISI | PUBMED32. GlaxoSmithKline. Clinical trial register for a multicenter, randomized, double-blind,double-dummy,parallel group, 8-week comparison of salmeterol xinafoate versus ipratropium bromide versus salmeterol
xinafoate plus ipratropium bromide versus placebo in subjects with chronic obstructive pulmonary disease. http://ctr.gsk.co.uk/Summary/salmeterol/IV_SMS40315.pdf. Accessed August 5, 2008. 33. GlaxoSmithKline. Clinical trial register for a multicenter, randomized, double-blind,double-dummy, parallel-group, 8-week comparison of salmeterol xinafoate versus ipratropium bromide versus salmeterol xinafoate plus ipratropium bromide versus placebo in subjects with chronic obstructive pulmonary disease. http://ctr.gsk.co.uk/Summary/salmeterol/IV_SMS40314.pdf. Accessed August 5, 2008. 34. Mahler DA, Donohue JF, Barbee RA; et al. Efficacy of salmeterol xinafoate in the treatment of COPD. Chest. 1999;115(4):957-965. FULL TEXT | ISI | PUBMED 35. Curkendall SM, DeLuise C, Jones JK; et al. Cardiovascular disease in patients with chronic obstructive pulmonary disease, Saskatchewan, Canada, cardiovascular disease in COPD patients. Ann Epidemiol. 2006;16(1):63-70. FULL TEXT | ISI | PUBMED 36. Salpeter SR, Ormiston TM, Salpeter EE. Cardiovascular effects of beta-agonists in patients with asthma and COPD: a meta-analysis. Chest. 2004;125(6):2309-2321. FULL TEXT | ISI | PUBMED 37. Macie C, Wooldrage K, Manfreda J, Anthonisen N. Cardiovascular morbidity and the use of inhaled bronchodilators. Int J Chron Obstruct Pulmon Dis. 2008;3(1):163-169. PUBMED 38. Lee TA, US Department of Veterans Affairs. Outcomes associated with salmeterol use in obstructive lung disease (September 2007). http://www.hsrd.research.va.gov/research/abstracts.cfm? Project_ID=2141694968&UnderReview=no. Accessed August 5, 2008. 39. Jara M, Lanes SF, Wentworth C III, May C, Kesten S. Comparative safety of long-acting inhaled bronchodilators:a cohort study using the UK THIN primary care database. Drug Saf. 2007;30(12):1151- 1160. ISI | PUBMED 40. de Luise C, Lanes SF, Jacobsen J, Pedersen L, Sørensen HT. Cardiovascular and respiratory hospitalizations and mortality among users of tiotropium in Denmark. Eur J Epidemiol. 2007;22(4):267- 272. FULL TEXT | ISI | PUBMED 41. Sin DD, Man SF. Why are patients with chronic obstructive pulmonary disease at increased risk of cardiovascular diseases? the potential role of systemic inflammation in chronic obstructive pulmonary disease. Circulation. 2003;107(11):1514-1519. FREE FULL TEXT 42. Boekholdt SM, Peters RJ, Hack CE; et al. IL-8 plasma concentrations and the risk of future coronary artery disease in apparently healthy men and women: the EPIC-Norfolk prospective population study. Arterioscler Thromb Vasc Biol. 2004;24(8):1503-1508. FREE FULL TEXT 43. Ebi-Kryston KL. Respiratory symptoms and pulmonary function as predictors of 10-year mortality from respiratory disease, cardiovascular disease,and all causes in the Whitehall Study. J Clin Epidemiol. 1988;41 (3):251-260. FULL TEXT | ISI | PUBMED 44. Mancini GB, Etminan M, Zhang B, Levesque LE, FitzGerald JM, Brophy JM. Reduction of morbidity and mortality by statins, angiotensin-converting enzyme inhibitors, and angiotensin receptor blockers in patients with chronic obstructive pulmonary disease. J Am Coll Cardiol. 2006;47(12):2554-2560. FREE FULL TEXT 45. Decramer M, Celli B, Tashkin DP; et al. Clinical trial design considerations in assessing long-term functional impacts of tiotropium in COPD: the UPLIFT trial. COPD. 2004;1(2):303-312. PUBMED 46. Calverley PMA, Anderson JA, Celli B; et al. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med. 2007;356(8):775-789. FREE FULL TEXT 47. Sidney S, Sorel M, Quesenberry CP Jr; et al. COPD and incident cardiovascular disease hospitalizations and mortality: Kaiser Permanente medical care program. Chest. 2005;128(4):2068-2075. FULL TEXT | ISI | PUBMED 48. Huiart L, Ernst P, Suissa S. Cardiovascular morbidity and mortality in COPD. Chest. 2005;128(4):2640- 2646. FULL TEXT | ISI | PUBMED 49. Mannino DM. Epidemiology and global impact of chronic obstructive pulmonary disease. Semin Respir Crit Care Med. 2005;26(2):204-210. FULL TEXT | ISI | PUBMED
HOME | CURRENT ISSUE | PAST ISSUES | TOPIC COLLECTIONS | CME | SUBMIT | SUBSCRIBE | HELP
PRIMERA: NATURALEZA, NACIONALIDAD Y DENOMINACIÓN. La sociedad es de naturaleza anónima, de capital fijo, de nacionalidad salvadoreña y girará con la denominación de SCOTIA SEGUROS, SOCIEDAD ANÓNIMA, que podrá abreviarse SCOTIA SEGUROS, S.A. SEGUNDA: DOMICILIO DE LA SOCIEDAD. El domicilio principal de la Sociedad será la ciudad de San Salvador, Departamento de San Salvador, pero por a
Kérdezze meg orvosát… …gyógyszerészét Immunrendszerről és erősítéséről Az emberi test immunrendszere jól összehangolt működésével megvéd ben- Immunrendszerünk erősítése érdekében fontos, hogy táplálékunk minél több nünket a betegségektől. Egészségesnek lenni és maradni csak jól működő im- vitamint és ásványi anyagot tartalmaz


 Vol. 300 No. 12, September 24, 2008
Vol. 300 No. 12, September 24, 2008 death, MI, or stroke among patients with COPD.
death, MI, or stroke among patients with COPD. Review Manager (RevMan) version 5.04 (Nordic Cochrane Center,Copenhagen, Denmark) was used tocalculate relative risk (RR) and 95% confidence intervals (CIs) for the primary composite outcome(cardiovascular death, MI, and stroke), the individual end points of the composite,as well as all-causemortality. All reported P values are 2-sided with significance set at less than .05. Statistical heterogeneitywas assessed using the I2 statistic.15 I2 values of 50% or more indicate a substantial level of heterogeneity.
Review Manager (RevMan) version 5.04 (Nordic Cochrane Center,Copenhagen, Denmark) was used tocalculate relative risk (RR) and 95% confidence intervals (CIs) for the primary composite outcome(cardiovascular death, MI, and stroke), the individual end points of the composite,as well as all-causemortality. All reported P values are 2-sided with significance set at less than .05. Statistical heterogeneitywas assessed using the I2 statistic.15 I2 values of 50% or more indicate a substantial level of heterogeneity.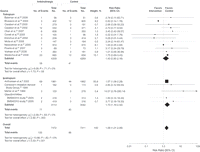 control therapy.Twelve trials evaluated inhaled tiotropium vs control therapy,19-30 and 5 trials evaluatedinhaled ipratropium vs control therapy.4, 31-34 Nine trials evaluated inhaled anticholinergics vs placebo.4, 19,21-23,26-27,29-30 The remaining trials used active comparators, including inhaled salmeterol,24-25,32-34 acombination inhaler containing salmeterol and fluticasone,20, 28 or inhaled albuterol.31 There were 5 long-term trials ranging from 48 weeks to 5 years,4, 19-22 and 12 short-term trials ranging from 6 weeks to 26weeks.23-34 The mean predicted FEV of participants was less than 50% for all trials, except 1 trial4 in which
The quality assessment of included trials is shown in Table 2. Trial quality was variable.All trials weredouble-blinded. Allocation concealment was adequate in 4 RCTs,4, 20, 23, 27 and unclear in the remaining 13RCTs.19, 21-22,24-26,28-34 Information on withdrawal rates was available for all RCTs except 1 trial,28 andranged from 6.1%23 to as high as 42%.20 Reporting of loss to follow-up was variable and only available for6 RCTs4, 20, 27, 29, 31, 34 and ranged from 0%34 to 3.4%.29
View this table:
control therapy.Twelve trials evaluated inhaled tiotropium vs control therapy,19-30 and 5 trials evaluatedinhaled ipratropium vs control therapy.4, 31-34 Nine trials evaluated inhaled anticholinergics vs placebo.4, 19,21-23,26-27,29-30 The remaining trials used active comparators, including inhaled salmeterol,24-25,32-34 acombination inhaler containing salmeterol and fluticasone,20, 28 or inhaled albuterol.31 There were 5 long-term trials ranging from 48 weeks to 5 years,4, 19-22 and 12 short-term trials ranging from 6 weeks to 26weeks.23-34 The mean predicted FEV of participants was less than 50% for all trials, except 1 trial4 in which
The quality assessment of included trials is shown in Table 2. Trial quality was variable.All trials weredouble-blinded. Allocation concealment was adequate in 4 RCTs,4, 20, 23, 27 and unclear in the remaining 13RCTs.19, 21-22,24-26,28-34 Information on withdrawal rates was available for all RCTs except 1 trial,28 andranged from 6.1%23 to as high as 42%.20 Reporting of loss to follow-up was variable and only available for6 RCTs4, 20, 27, 29, 31, 34 and ranged from 0%34 to 3.4%.29
View this table: risk of MI (1.2% vs 0.8% for control; RR, 1.53 [95% CI, 1.05-2.23]; P = .03) in a meta-analysis of 11trials involving 10 598 patients.4, 19-22,24, 26, 28, 31-33 Inhaled anticholinergics also significantly increased therisk of cardiovascular death (0.9% vs 0.5% for control; RR, 1.80 [95% CI,1.17-2.77]; P = .008) in a meta-analysis of 12 trials involving 12 376 patients.4, 19-21,23-25,27, 29-31,33 Inhaled anticholinergics did notsignificantly increase the risk of stroke (0.5% vs 0.4% for control; RR, 1.46 [95% CI, 0.81-2.62]; P = .20)in a meta-analysis of 7 trials involving 9251 patients.4, 19-20,24, 32-34 There was no evidence of statisticalheterogeneity among the included trials for any of these end points (I2 = 0%for MI, cardiovascular death,and stroke) (Table 4).
risk of MI (1.2% vs 0.8% for control; RR, 1.53 [95% CI, 1.05-2.23]; P = .03) in a meta-analysis of 11trials involving 10 598 patients.4, 19-22,24, 26, 28, 31-33 Inhaled anticholinergics also significantly increased therisk of cardiovascular death (0.9% vs 0.5% for control; RR, 1.80 [95% CI,1.17-2.77]; P = .008) in a meta-analysis of 12 trials involving 12 376 patients.4, 19-21,23-25,27, 29-31,33 Inhaled anticholinergics did notsignificantly increase the risk of stroke (0.5% vs 0.4% for control; RR, 1.46 [95% CI, 0.81-2.62]; P = .20)in a meta-analysis of 7 trials involving 9251 patients.4, 19-20,24, 32-34 There was no evidence of statisticalheterogeneity among the included trials for any of these end points (I2 = 0%for MI, cardiovascular death,and stroke) (Table 4).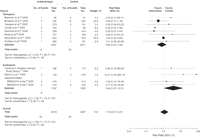 Trials of Inhaled Anticholinergics vs Control for Major AdverseCardiovascular Outcomes Composite
Cardiovascular outcomes composite indicates cardiovasculardeath,myocardial infarction, and stroke. Short-term indicates 6weeks to 6 months. Size of the data markers indicates weight ofthe study.CI indicates confidence interval.
Trials of Inhaled Anticholinergics vs Control for Major AdverseCardiovascular Outcomes Composite
Cardiovascular outcomes composite indicates cardiovasculardeath,myocardial infarction, and stroke. Short-term indicates 6weeks to 6 months. Size of the data markers indicates weight ofthe study.CI indicates confidence interval.