Children and adolescents infected with <i>wuchereria bancrofti</i> in greater recife, brazil: a randomized, year-long clinical trial of single treatments with diethylcarbamazine or diethylcarbamazineÂŒalbendazole
Annals of Tropical Medicine & Parasitology, Vol. 101, No. 5, 423–433 (2007)
Children and adolescents infected with Wuchereriabancrofti in Greater Recife, Brazil: a randomized,year-long clinical trial of single treatments withdiethylcarbamazine or diethylcarbamazine–albendazole
ˆ . RIZZO*,{, C. BELO{, R. LINS{ and G. DREYER{,1
*Rua do Sossego 715, CEP 50100-150, Recife, PE, Brazil{Centro de Pesquisas em Alergia e Imunologia Clı´nica, Ambulato´rio de Alergia, Hospital dasClı´nicas, Universidade Federal de Pernambuco, Avenida Moraes Rego s/n, Cidade Universita´ria,CEP 50740-900, Recife, PE, Brazil{Nu´cleo de Ensino, Pesquisa e Assisteˆncia em Filariose (NEPAF), Centro de Cieˆncias da Sau´de,Hospital das Clı´nicas, Universidade Federal de Pernambuco, Avenida Professor Moraes Rego s/n,Cidade Universita´ria, CEP 50740-900, Recife, PE, Brazil1Centro de Pesquisas Aggeu Magalha˜es – Fiocruz, Avenida Moraes Rego s/n, CidadeUniversita´ria, CEP 50670-420, Recife, PE, Brazil
Received 10 May 2006, Revised 20 November 2006,Accepted 23 November 2006
In filariasis-endemic areas beyond sub-Saharan Africa, the World Health Organization’s recommended strategy forinterrupting transmission of the causative parasites is annual, single-dose, mass treatment with a combination ofdiethylcarbamazine (DEC; given at 6 mg/kg) and albendazole (ALB; given at 400 mg) for 4–6 years (the minimumestimated life-span of the adult parasites). In an open, hospital-based, randomized and controlled trial, with ablinded evaluation of outcome, 82 children and adolescents from Recife, all with Wuchereria bancroftimicrofilaraemias, were given either DEC alone (6 mg/kg) or the same dose of DEC combined with ALB (at400 mg/patient). Every 90 days for 1 year after the single treatment, each patient was checked for microfilaraemiaby the filtration of up to 5 ml of venous blood collected at night. One year post-treatment, 16 (39%) of the 41patients given DEC alone and 20 (49%) of the 41 given DEC–ALB were found microfilaraemic (relative risk50.8,with a 95% confidence interval of 0.49–1.31) and the corresponding geometric mean levels of microfilaraemia were2.0% and 1.8% of the levels recorded immediately pre-treatment, respectively (P.0.05). In terms of theprevalences and intensities of microfilaraemia, therefore, the addition of ALB to the DEC appeared to offer nosignificant benefit.
In humans, lymphatic filariasis (LF) is a
South and Central America. It is considered
major cause of clinical morbidity, affecting
of permanent disability (WHO, 2003).
Wuchereria bancrofti is the most wide-spread
of the species of filariae that cause LF andone that infects approximately 100 millionpeople in tropical and sub-tropical areas,
Pesquisa e Assisteˆncia em Filariose (NEPAF), Centrode
Professor Moraes Rego s/n, Cidade Universita´ria,
tions occur years after initial infection, LF is
CEP 50740-900, Recife, PE, Brazil. E-mail [email protected]; fax: z55 81 3426 4348.
frequently viewed as an adult disease. The
# 2007 The Liverpool School of Tropical Medicine
earlier notion that LF is not a paediatric
(2001) found that many children in endemic
Most clinical and field trials investigating
the efficacy and tolerance of such DEC–
filaraemic, even when the detection method
ALB combinations, in bancroftian filariasis,
have used adult subjects (Ismail et al., 1998,
technique traditionally used for diagnosis:
2001; Pani et al., 2002; El Setouhy et al.,
2004; Kshirsagar et al., 2004; Fox et al.,
2005), and not all of them have included a
diagnostic tools, such as assays to detect
filarial antigens and ultrasound to visualize
living adult worms in their natural habitat,
even in the absence of microfilaraemia, has
included 24 children under 14 years of age
added further evidence of childhood infec-
in their study group of 54 individuals but
tion. In a cohort of Haitian children, for
did not give separate efficacy results for their
example, the prevalence of microfilaraemia
recent, community-based study, Fox et al.
1.3% between the ages of 2 and 4 years but
relatively short follow-up (6 months) and a
relatively insensitive method (the microsco-
pical examination of a 20-ml thick smear) to
(14%) of the 78 children they investigated.
appear to have been no randomized trials,
Living adult worms were detected, in nine
boys, in the intrascrotal lymphatic vessels
effects on microfilaraemia of single treat-
and those of the inguinal cord, demonstrat-
the present study, which was triggered partly
tasia) without overt clinical disease (Dreyer
lymphatic damage of infected children sets
Kumaraswami, 2004), was to fill this gap,
the stage for the pathological changes and
using, as subjects, children and adolescents
disability seen in adults. By treating the
possible to prevent many, if not all, ofthe chronic and often irreversible manifesta-tions of lymphatic dysfunction seen later inlife.
The research protocol was approved by the
Federal University of Pernambuco, Brazil,
and written informed consent was obtained
either from the subjects (if aged >16 years)
or their parents/guardians (for subjects aged
,16 years). The travel costs of the patients
DEC OR DEC–ALBENDAZOLE TREATMENT OF CHILDREN
and their parents were paid by the research
microfilaraemia clearance previously observed
1 year after a single treatment with DEC(40%; Andrade et al. 1995), and thecorresponding frequencies, of about 70%,
observed or predicted for ALB–ivermectin
(Bockarie et al., 1998) and DEC–ivermec-
tin (Ismail et al., 1998). In order to give a
(microfilaraemia prevalence and intensity),
using stratified, parallel groups of micro-
in the prevalence of microfilaraemia, it was
estimated that 42 patients would be needed
aim was to compare the effects on outcome,
up to 1 year post-treatment, of a single dose
study, the patients were stratified into four
groups according to the intensities of their
microfilaraemias (1–100, 101–250, 251–1000 and .1000 microfilarae/ml blood). A
restricted block-randomization list for each
To be enrolled, a patient had to be aged 9–
stratum was then generated (by an indivi-
19 years and to have been found microfilar-
dual who was not otherwise connected with
aemic (by the microscopical examination of
the research). At the Nu´cleo de Ensino,
a thick bloodsmear), by staff working for the
Pesquisa e Assisteˆncia em Filariose (NEPAF),
governmental programme for filariasis con-
trol, during screening in the city of Jaboata˜o
metropolitan area. Greater Recife lies in an
area of north–eastern Brazil where bancrof-
their baseline levels of microfilaraemia.
Patients were excluded if they: (1) had a
They were then sent to the paediatric ward
history of any previous treatment with DEC,
in the Hospital das Clı´nicas, for medical
ivermectin or any other anti-helminthic drug
history of severe asthma or seizures, cardio-
patient for microfilaraemia, and estimated
vascular, hepatic or renal disease, or other
conditions for which antifilarial drugs might
be contra-indicated; (3) were female and of
reproductive age and either refused to be
tested for pregnancy or gave a positive resultin a pregnancy (human chorionic gonado-
tropin) test; (4) reported personal or par-
All patients underwent an initial assessment
for inclusion and exclusion criteria, quanti-
fication of microfilaraemia at night, and amedical evaluation that included the taking
of a clinical history, a complete physical
examination, and a social interview. All the
females of reproductive age had a blood test
,0.05 was considered indicative of a statis-
supervision, between 08.30 and 09.30 hours.
Doses of DEC (Farmanguinhos, Rio deJaneiro, Brazil) were calculated as 6 mg/kgbody weight, rounded upwards to the
nearest 25 mg (i.e. half of a 50-mg tablet). Albendazole
Overall, 84 microfilaraemic patients aged 9–
single dose, irrespective of bodyweight. A
5-ml sample of venous ‘night’ blood was
the other 41 patients to the DEC–ALB arm.
At baseline, the patients in the two treat-
filtration of 1-ml aliquots of these blood
ment arms appeared similar (see Table).
membranes (Nuclepore, Pleasanton, CA).
days of follow-up. The two other patients
(who had pre-treatment microfilaraemias of
Giemsa’s stain so that the trapped micro-
five and 222 mff/ml) accepted their sched-
Kean, 1971). If a 1-ml aliquot of ‘night’
negative for microfilariae (mff), the remain-
ing sample (4 ml) was also checked for mff
by membrane filtration. (Sera isolated from
the blood samples collected are currently
arm significantly different from those in the
being checked for circulating filarial antigen
DEC–ALB arm. Patients in both treatment
arms showed statistically significant declinesin microfilaraemia intensity up to day 270
post-treatment but then a much less steep
and non-significant reduction between day
unpaired t-tests or x2 tests. Intensities of
270 and the final follow-up on day 360. At
the end of follow-up, prevalences of micro-
means (i.e. using the ‘nz1’ convention to
were 2.0% and 1.8% of their pre-treatment
transformed before comparison in unpaired
levels, respectively (P.0.05; Fig. 1).
intensities of microfilaraemia at different
Bonferroni’s correction. The prevalences of
interval of 34%–64%) of the 41 patients in
microfilaraemia in the two treatment arms
were compared using x2 tests. Within each
aemic (giving a relative risk of 0.8, with a
95% confidence interval of 0.49–1.31). The
was used to investigate the significance of
the temporal differences seen in the pre-
DEC OR DEC–ALBENDAZOLE TREATMENT OF CHILDREN
lence of microfilaraemia decreased steadily,
although this decrease was only statistically
recorded in the DEC arm were similar, both
in frequency and type, to those observed in
and not throughout the entire follow-up, as
function [as measured by forced expiratory
stratum for microfilaraemia intensity were
arms still appeared similar in terms of the
prevalence of microfilaraemia on day 360.
than the patients who had the lowest levels
mild dyspnoea but only one of them showed
a corresponding fall in FEV1. A localized
AE — an uncomfortable scrotal nodule —
was observed in three patients (two given
was observed in 81% of the patients. All of
the systemic AE observed began within 24 h
of treatment and, in all but one patient,had disappeared within 48 h of treatment. Almost all (85%) of these events were mild,
and only one patient was considered to havesuffered a severe AE and that was a cough
The present study appears to represent the
that disturbed the patient’s sleep until
trolled trial to evaluate and compare the
Descriptive data for the subjects in the two treatment groups, on enrolment
INTENSITY OF MICROFILARAEMIA (microfilariae/ml blood)
FIG. 1. The geometric mean intensities of microfilaraemia recorded, immediately pre-treatment (‘time 0’) andduring the post-treatment follow-up, among the patients given a single dose of diethylcarbamazine only (&) andthose given a single dose of diethylcarbamazine–albendazole (%).
year-long efficacies of single treatments with
microfilaraemia, only one of the 15 patients
children and adolescents with W. bancrofti
their microfilaraemias by day 360 (data not
intensities of microfilariaemia declined with
time in both treatment arms and were lowest
study was the lack of an adequate placebo
treatment. There were, in fact, no signifi-
tablets. All the checks for microfilaraemia
patients who had low baseline intensities of
DEC OR DEC–ALBENDAZOLE TREATMENT OF CHILDREN
FIG. 2. The prevalences of microfilaraemia recorded, immediately pre-treatment (‘time 0’) and during the post-treatment follow-up, among the patients given a single dose of diethylcarbamazine only (&) and those given asingle dose of diethylcarbamazine–albendazole (%).
attending physicians were always unaware of
the intensity of microfilaraemia (if any) in
each patient. The present study, with fewer
their blood was filtered, was tested again,
than 50 patients in each treatment arm, may
using a 4-ml sample of blood. On day 360,
also have failed to reveal between-treatment
however, only three more microfilaraemics
differences that, although relatively small,
(one in the DEC arm and two in the DEC–
may still be important in the context of mass
ALB) were detected as the result of testing
the 4-ml blood samples (data not shown).
results may indicate levels of efficacy that
of DEC–ALB to each of 11 adult patients
956 mff/ml and, after testing a 1-ml blood
(73%) of the patients still microfilaraemic
treatment on the prevalence of microfilar-
aemia observed 1 year post-treatment have
similar treatment to another 14 adults, with
varied between the published studies. One
difficulty in comparing the results of such
long-term follow-up, even from randomized
microfilaraemic 1 year later (Ismail et al.,
and controlled trials, is the between-study
2001). The prevalences of microfilaraemia
variation in the baseline intensities of micro-
recorded, by Ismail et al. (1998, 2001), 1
Simonsen et al., 2004). Another problem is
the between-study variation in the sensitivity
study among the patients with similar base-
of the method used to detect microfilarae-
line intensities of microfilaraemia (data
mias. Sensitivity may be affected, for exam-
ple, by the volume of blood tested/subject,
collected, and the way in which the samples
are checked for mff (Dreyer et al., 1996b).
In their three-arm trials, Pani et al. (2002)
studied the effects of single treatments with
over the following 12 months. It is a pity
who had relatively mild microfilaraemias at
that this study did not include a DEC-only
79.4 mff/ml, respectively). One year post-
benefit of adding albendazole to DEC, both
for a single treatment and for daily treat-
appeared similar in terms of the prevalence
and intensity of microfilaraemia, although,
study (Fig. 2), the prevalences of microfilar-
aemia recorded at the 1-year follow-up were
5–11 years, they found the combination to
relatively high (82.4% for DEC, 73.9% for
reducing the intensities (but not the pre-
valences) of microfilaraemia 6 months post-
reductions in the prevalences of microfilar-
treatment. Their evaluations were, however,
aemia, in all three treatment arms, during
based on the examinations of relatively small
the second year post-treatment (Pani et al.,
(20-ml) samples of fingerprick blood col-
2004). Unfortunately, Pani et al. (2002) did
lected early at night. As in the present study,
of W. bancrofti in Brazil, in their study of
subject, did not describe the method they
used to evaluate the prevalence or intensity
their efficacy results by age-group.
single, annual doses — as DEC–ALB (or
that 67% of 21 patients given a single dose
In a recent review, Gyapong et al. (2005)
of DEC and 59% of 22 patients given DEC–
cited five trials in which DEC and DEC–
microfilaraemia clearance are slightly higher
[including one, among adults from Recife,
than the corresponding values (of 61% and
which has since appeared in the scientific
51%, respectively) seen in the present study,
literature (Dreyer et al., 2006)]. Although
Kshirsagar et al. (2004) only used micro-
the authors of this review concluded that
blood/patient (at each follow-up) and prob-
ior to DEC alone, their analysis was flawed
meta-analysis. The effect of this error was to
increase the total patient number artificially,
doses as used singly in the present study)
was much more effective, in clearing blood
between-treatment difference where actually
microfilariae after 1 year, than a single dose
there was none (Critchley et al., 2005).
patients in the multi-dose group were given
a single dose of the combination, 1 year after
lished randomized trials in which the effi-
their week of treatment, and all but one was
found amicrofilaraemic a year later. In the
single-dose group, this single dose at 1 year
DEC OR DEC–ALBENDAZOLE TREATMENT OF CHILDREN
and pooling the prevalences and intensities
low levels over the year post-treatment. The
of microfilaraemia reported in the trials, the
treatment of microfilaraemic children and
adolescents from the metropolitan area of
improve effectiveness, and that, to date, the
Recife, Brazil, did not show any benefit in
most efficacious combination is DEC–iver-
terms of further reducing the prevalence or
intensity of microfilaraemia at 1 year post-
ever, that the relative efficacies of the
treatment. Clearly, considerable collateral
helminthiases may be realised if any anti-
large, conclusive studies on this topic. In
their Cochrane review, Critchley et al.
effects on intestinal helminths, regular treat-
the lack of consistent information on the
effects of ALB when used to treat LF.
regardless of whether LF is endemic in those
treatments for bancroftian filariasis, it is very
benefits of ALB do not, however, diminish
baseline intensities of microfilaraemia and
the need to elucidate the real effects on
the sensitivity of the detection method, as
the apparent efficacy of a treatment is very
dependent on both of these factors. This isadvisable even for population-based studies,since individuals with intense microfilarae-
the patients and their guardians for their
mias are unlikely to become amicrofilarae-
trust and co-operation, the Amaury Coutinho
mic, even after five or six annual treatment
financial support, and Dr E. Meireles, for
referring patients. They are also grateful to
et al., 1998; Ramaiah et al., 2002).
Sadly, although effective microfilaricidal
paediatric ward, Professor J. Natal Figueiroa,
drugs are available, no current treatment
for statistical advice, and Dr D. Addiss, for
regimen is completely successful at killing all
his critical reading and helpful discussion of
Noro˜es et al., 1997). This has importantimplications for the GPELF and calls forincreased attention to vector control, which
could hasten the elimination of LF andreduce the risk of a resurgence in transmis-sion, after treatment interruption, caused by
Andrade, L., Medeiros, Z., Pires, M. L., Pimentel, A.,
Figueiredo-Silva, J., Coutinho, A. & Dreyer, G.
a few individuals with low-level microfilar-
(1995). Comparative efficacy of three different
diethylcarbamazine regimens in lymphatic filariasis.
particularly long life-spans of microfilariae-
Transactions of the Royal Sociecty of Tropical Medicine
producing adult worms in settings with low
transmission pressure (Dreyer et al., 2005).
Bockarie, M. J., Alexander, N. D. E., Hyun, P.,
Dimber, Z., Bockarie, F., Ibam, E., Alpers, M. P.
& Kazura, J. W. (1998). Randomised community-
DEC–ALB appear equally effective in redu-
based trial of annual single-dose diethylcarbamazine
cing intensities of microfilaraemia to very
bancrofti infection in human beings and mosquitoes.
bancrofti. Transactions of the Royal Society of Tropical
Medicine and Hygiene, 100, 1118–1125.
Bradley, M. H.& Kumaraswami, V. (2004). Lymphatic
El Setouhy, M., Ramzy, R. M. R., Ahmed, E. A.,
Filariasis Research Forum. Towards a strategic plan
Kandii, M., Hussain, O., Farid, H. A., Helmy, H. &
for research to support the Global Program to
Weil, G. J. (2004). A randomized clinical trial
Eliminate Lymphatic Filariasis. Essential tools —
drugs and clinical drug trials. American Journal of
therapy with diethylcarbamazine and albendazole
Tropical Medicine and Hygiene, 71 (Suppl.), 7–11.
for treatment of bancroftiana filariasis. American
Critchley, J., Addiss, D., Gamble, C., Garner, P.,
Journal of Tropical Medicine and Hygiene, 70, 191–
Gelband, H. & Ejere, H. (2005). Albendazole for
Esterre, P., Plichart, C., Sechen, Y. & Nguyen, N. L.
Cochrane Database of Systematic Reviews 2005,
(2001). The impact of 34 years of massive DEC
Issue 19. Art. No. CD003753. Chichester, U.K.:
chemotherapy on infection and transmission: the
Maupiti cohort. Tropical Medicine and International
Dennis, D. T. & Kean, B. H. (1971). Isolation of
microfilariae: report of a new method. Journal of
Fox, L. M., Furness, B.W., Haser, J. K., Desire, D.,
De Rochars, M. B., Direny, A. N., Roberts, J. M.,
Lammie, P. J. & Beach, M. J. (2005). Tolerance
Addiss, D. G., Radday, J., Beach. M. J., Streit, T. G.,
and efficacy of combined diethylcarbamazine and
Dardith, D., Lafontant, J. G. & Lammie, P. J.
albendazole for treatment of Wuchereria bancrofti and
(2004). Community-wide reduction in prevalence
intestinal helminth infections in Haitian children.
and intensity of intestinal helminths as a collateral
American Journal of Tropical Medicine and Hygiene, 73,
benefit of lymphatic filariasis elimination programs.
American Journal of Tropical Medicine and Hygiene, 71,
Gyapong, J. O., Kumaraswami, V., Biswas, G. &
Ottesen, E. A. (2005). Treatment strategies under-
Ultrasonographic assessment of the adulticidal effi-
cacy of repeated high-dose ivermectin in bancroftian
filariasis. Tropical Medicine and International Health, 1,
Dreyer, G., Pimentel, A., Medeiro, Z., Be´liz, F.,
Rajaratnam, H. N., Amarasekera, N., De Silva,
D. C. L., Michalski, M. L. & Dissanaike, A. S.
Rocha, A., Silva, L. M. & Piessens, W. (1996b).
(1998). Efficacy of single dose combinations of
Studies on the periodicity and intravascular distribu-
albendazole, ivermectin and diethylcarbamazine for
tion of Wuchereria bancrofti microfilariae in paired
the treatment of bancroftian filariasis. Transactions of
samples of capillary and venous blood from Recife,
the Royal Society of Tropical Medicine and Hygiene, 92,
Brazil. Tropical Medicine and International Health, 1,
Ismail, M. M., Jayakody, R. L., Weil, G. J., Deepika, F.,
Dreyer, G., Addiss, D., Santos, A., Figueredo-Silva, J.
de Silva, M. S. G., de Silva, G. A. C. & Balasooriya,
˜ es, J. (1998). Direct assessment in vivo of the
W. K. (2001). Long-term efficacy of single-dose
efficacy of combined single-dose ivermectin and
combinations of albendazole, ivermectin and diethyl-
diethylcarbamazine against adult Wuchereria ban-
carbamazine for the treatment of bancroftian filar-
crofti. Transactions of the Royal Sociecty of Tropical
iasis. Transactions of the Royal Society of Tropical
Medicine and Hygiene, 92, 219–222.
Medicine and Hygiene, 95, 332–335.
Kshirsagar, N. A., Gogtay, N. J., Garg, B. S.,
Deshmukh, P. R., Rajgor, D. D., Kadam, V. S.,
Bancroftian filariasis in a paediatric population: an
Kirodian, B. G., Ingole, N. S., Mehendale, A. M.,
ultrasonographic study. Transactions of the Royal
Fleckenstein, L., Karbwang, J. & Lazdins-Helds, J. K.
Society of Tropical Medicine and Hygiene, 93, 633–636.
(2004). Safety, tolerability, efficacy and plasma
concentrations of diethylcarbamazine in a field study
longevity of adult Wuchereria bancrofti increase with
in an area endemic for lymphatic filarasis in India.
decreasing intensity of parasite transmission? Insights
Transactions of the Royal Society of Tropical Medicine
from clinical observations. Transactions of the Royal
Society of Tropical Medicine and Hygiene, 99, 883–892.
Lammie, P. J., Reiss, M. D., Dimock, K. A., Streit,
Dreyer, G., Addiss, D., Williamson, J. & Noro˜es, J.
T. G., Roberts, J. M. & Eberhard, M. L. (1998).
(2006). Efficacy of co-administered diethylcarbama-
Longitudinal analysis of the development of filarial
infection and antifilarial immunity in a cohort of
DEC OR DEC–ALBENDAZOLE TREATMENT OF CHILDREN
and adult parasites in asymptomatic microfilaremic
Medicine and Hygiene, 59, 217–221.
volunteers. Result of two-year follow-up. Indian
Shimada, M. (1998). Efficacy of five annual single
Ramaiah, K. D., Vanamail, P., Pani, S. P., Yuvaraj, J. &
dose of diethylcarbamazine for treatment of lympha-
Das, P. K. (2002). The effect of six rounds of single
tic filariasis in Fiji. Bulletin of the World Health
dose mass treatment with diethylcarbamazine or
ivermectin on Wuchereria bancrofti infection and its
Michael, E. (2000). The population dynamics and
implications for lymphatic filariasis elimination.
epidemiology of lymphatic filariasis. In Lymphatic
Tropical Medicine and International Health, 7, 767–
Filariasis, ed. Nutmann, T. pp. 42–80. London:
Shenoy, R. K., John, A., Babu, B. S., Suma, T. K. &
Molyneux, D. H. & Taylor, M. J. (2001). Current
Kumaraswami, V. (2000). Two-year follow-up of the
status and future prospects of the Global Lymphatic
microfilaraemia of asymptomatic brugian filariasis,
Filariasis Programme. Current Opinion in Infectious
after treatment with two, annual, single doses of
ivermectin, diethylcarbamazine and albendazole, in
Moulia-Pelat, J. P., Glaziou, P., Weil, G. J., Nguyen,
various combinations. Annals of Tropical Medicine and
Combination ivermectin plus diethylcarbamazine, a
Simonsen, P. E., Meyrowitsch, D. W., Mukoko, D. A.,
new effective tool for control of lymphatic filariasis.
Tropical Medicine and Parasitology, 46, 9–12.
Rwegoshora, R. T., Ouma, J. H., Masese, N.,
Noro˜es, J., Dreyer, G., Santos, A., Mendes, V. G.,
Jaoko, W. G. & Michael, E. (2004). The effect of
Medeiros, Z. & Addiss, D. (1997). Assessment of the
repeated half-yearly diethylcarbamazine mass treat-
efficacy of diethylcarbamazine on adult Wuchereria
ment on Wuchereria bancrofti infection and transmis-
bancrofti in vivo. Transactions of the Royal Society of
sion in two East African communities with different
Tropical Medicine and Hygiene, 91, 78–81.
levels of endemicity. American Journal of Tropical
Behbehani, K. (1997). Strategies and tools for the
Tisch, D. J., Michael, E. & Kazura, J. W. (2005). Mass
control/elimination of lymphatic filariasis. Bulletin of
chemotherapy options to control lymphatic filariasis:
the World Health Organization, 75, 491–503.
a systematic review. Lancet Infectious Diseases, 5, 514–
Pani, S. P., Reddy, G. S., Das, L. K., Vanamail, P.,
Hoti, S. L., Ramesh, J. & Das, P. K. (2002).
Witt, C. & Ottesen, E. A. (2001). Lymphatic filariasis:
Tolerability and efficacy of single dose albendazole,
an infection of childhood. Tropical Medicine and
diethylcarbamazine citrate (DEC) or co-administra-
tion of albendazole with DEC in clearance of
World Health Organization (1997). Fiftieth World
Wuchereria bancrofti in asymptomatic volunteers in
Health Assembly. Resolution 50.29. Geneva: WHO.
Pondicherry, South India: a hospital-based study.
World Health Organization (2000). Tropical Disease
Research. Fifteenth Programme Report. Progress 1999–
Pani, S. P., Reddy, S. R., Das, P. K. & Vanamail, P.
2000. Document TDR/GEN/01.5. Geneva: WHO.
(2004). Efficacy of single dose albendazole, diethyl-
World Health Organization (2003). Annual Report on
carbamazine citrate (DEC) or co-administration of
Lymphatic Filariasis 2002. Document WHO/CDS/
both in clearance of Wuchereria bancrofti microfilarial
To try and learn more about the genes involved tryptophan biosyntheisolate trp - mutants of E.coli . Briefly describe how you would isolate trp - mutants in your screen. (6pts) 1. Plate cells on nonselective rich media (that contains tryptophan). 2. Replica plate the cells onto media plates that lack tryptophan. 3. Colonies that did not grow on the plates without tryptophan but did grow on
2013 Student Ministry Event Permission Form - Cumming Baptist Church I________________________ give ________________________ permission to participate in student ministry sponsored events during 2013. In case of emergency, I give Chad Ireland or the person placed in charge of my child permission to have my child treated. I will not hold the individual, the attending physician, or Cumming Bapt
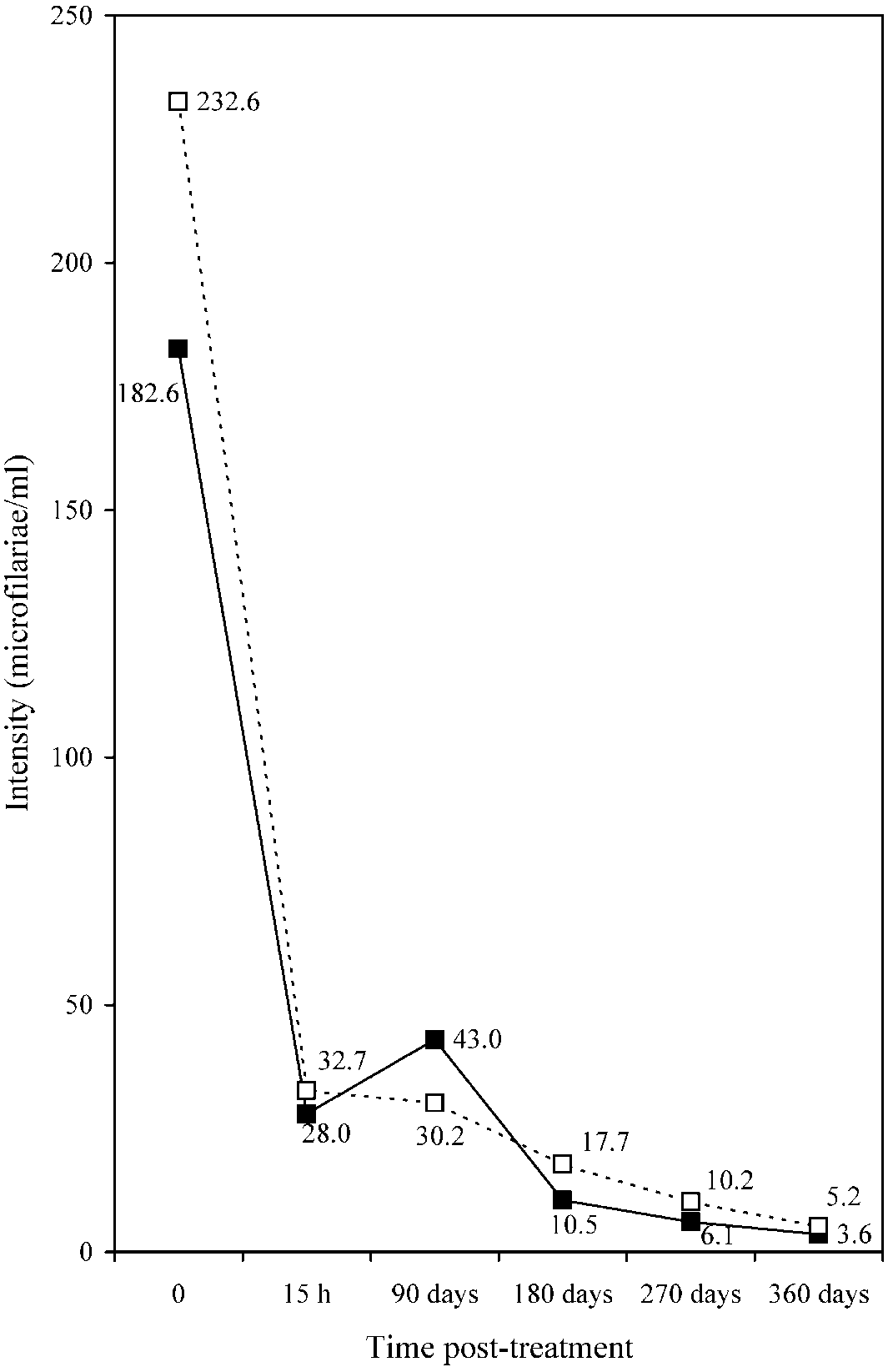 FIG. 1. The geometric mean intensities of microfilaraemia recorded, immediately pre-treatment (‘time 0’) andduring the post-treatment follow-up, among the patients given a single dose of diethylcarbamazine only (&) andthose given a single dose of diethylcarbamazine–albendazole (%).
FIG. 1. The geometric mean intensities of microfilaraemia recorded, immediately pre-treatment (‘time 0’) andduring the post-treatment follow-up, among the patients given a single dose of diethylcarbamazine only (&) andthose given a single dose of diethylcarbamazine–albendazole (%).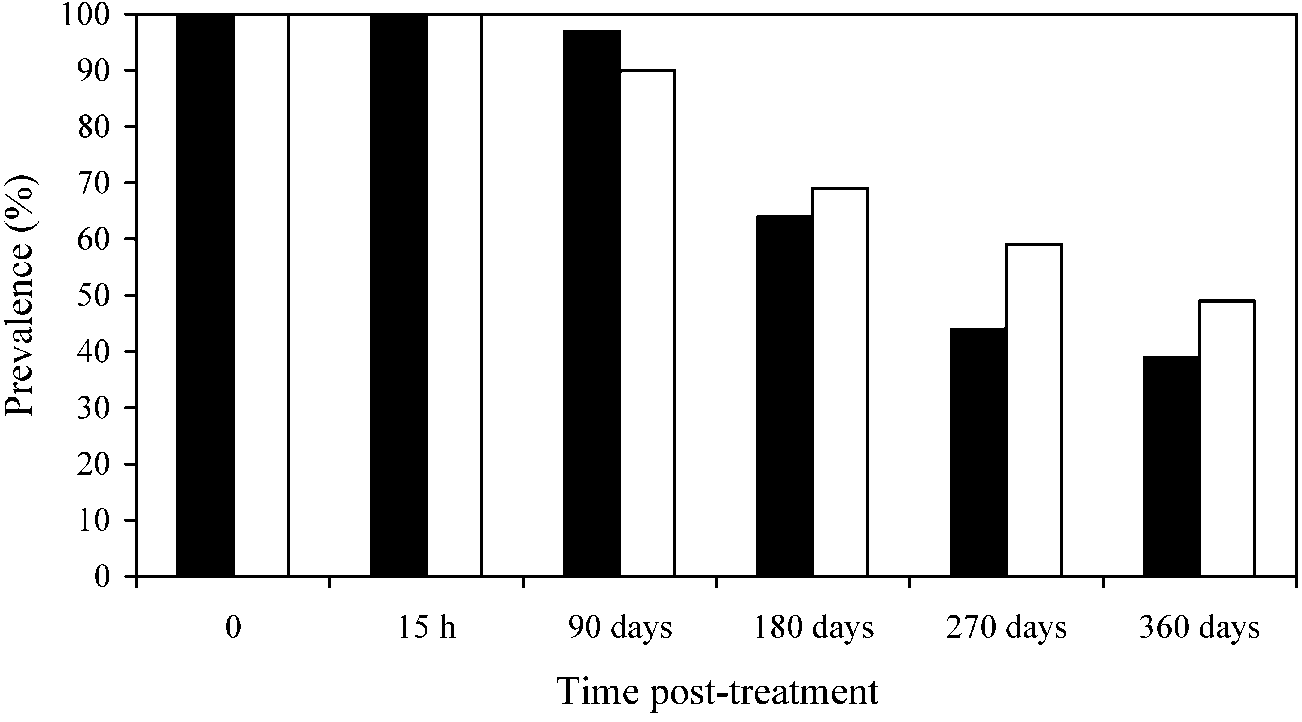 DEC OR DEC–ALBENDAZOLE TREATMENT OF CHILDREN
FIG. 2. The prevalences of microfilaraemia recorded, immediately pre-treatment (‘time 0’) and during the post-treatment follow-up, among the patients given a single dose of diethylcarbamazine only (&) and those given asingle dose of diethylcarbamazine–albendazole (%).
DEC OR DEC–ALBENDAZOLE TREATMENT OF CHILDREN
FIG. 2. The prevalences of microfilaraemia recorded, immediately pre-treatment (‘time 0’) and during the post-treatment follow-up, among the patients given a single dose of diethylcarbamazine only (&) and those given asingle dose of diethylcarbamazine–albendazole (%).