Visual perception in Parkinson disease dementia and dementia with Lewy bodies
U.P. Mosimann, MD; G. Mather, PhD; K.A. Wesnes, PhD; J.T. O’Brien, DM; D.J. Burn, MD;
Abstract—Objective: To quantify visual discrimination, space-motion, and object-form perception in patients with Parkin- son disease dementia (PDD), dementia with Lewy bodies (DLB), and Alzheimer disease (AD). Methods: The authors used a cross-sectional study to compare three demented groups matched for overall dementia severity (PDD: n ϭ 24; DLB: n ϭ 20; AD: n ϭ 23) and two age-, sex-, and education-matched control groups (PD: n ϭ 24, normal controls [NC]: n ϭ 25). Results: Visual perception was globally more impaired in PDD than in nondemented controls (NC, PD), but was not different from DLB. Compared to AD, PDD patients tended to perform worse in all perceptual scores. Visual perception of patients with PDD/DLB and visual hallucinations was significantly worse than in patients without hallucinations. Conclusions: Parkinson disease dementia (PDD) is associated with profound visuoperceptual impairments similar to dementia with Lewy bodies (DLB) but different from Alzheimer disease. These findings are consistent with previous neuroimaging studies reporting hypoactivity in cortical areas involved in visual processing in PDD and DLB.
Parkinson disease (PD) is associated with a higher
visual impairment in DLB11 and a recent study
risk of developing dementia compared to healthy el-
found similar impairments in pentagon copying in
derly controls; longitudinal studies suggest that up
DLB and PDD.12 Some of these studies used con-
to 78% of PD patients will develop dementia after
struction tasks as evidence, but this may not be le-
nearly two decades of motor symptoms.1 Once de-
gitimate given the motor impairments in these
mentia is established, clinical symptoms of PD de-
patients. Studies quantifying visual perception of
mentia (PDD) may show, apart from a longer
DLB and PDD using tasks without motor require-
duration of motor features, considerable overlap with
dementia with Lewy bodies (DLB). The postural
Peripheral structures such as the retina, the optic
nerve and tract, and primary visual cortex are mul-
represented in PDD and DLB2 and both disorders
timodal in their function, whereas the visual associ-
show similar fluctuation of attention3 and response
ation cortex is more specialized.13 Low-level visual
discrimination is mainly processed in visual area V1/
Studies comparing visual perception and visual
V2, whereas high-level visual functions require addi-
construction of PDD with Alzheimer disease (AD)
tional activation of large extrastriatal cortical
have revealed contradictory results. Some studies re-
networks.14 Two visual pathways can be distin-
port PDD to be more impaired,6,7 whereas other stud-
guished: the ventral occipito-temporal pathway,
ies found no differences.8,9 Similar inconsistencies
which is required for detailed analysis and identifi-
have been found when perception of PD patients was
cation of objects and forms, and the dorsal occipito-
compared with healthy controls.10 Since operational-
parietal pathway, required for spatial vision and
ized criteria to define the clinical boundaries be-
motion perception.14 Task selection of the present
study took these theoretical considerations into ac-
refinement, these inconsistencies may be partly due
count. We aimed to quantify perceptual differences
to diagnostic heterogeneity. When DLB was com-
in PDD, DLB, and AD patients matched for overall
pared with AD, studies consistently reported greater
dementia severity, and in non-demented controls(PD and NC). We tested visual discrimination,
Additional material related to this article can be found on the Neurology
object-form perception, and space-motion perception
Web site. Go to www.neurology.org and scroll down the Table of Con-
to assess impairments in different visual cortical
tents for the December 14 issue to find the title link for this article.
pathways. Since PDD and DLB have combined motor
From the Institute for Ageing and Health (Drs. Mosimann, O’Brien, Burn, and McKeith), Newcastle upon Tyne; Psychology Department (Dr. Mather), LifeSciences School, University of Sussex, Brighton; and Cognitive Drug Research Ltd. (Dr. Wesnes), Oxon, UK.
Supported by the UK Medical Research Council, the Swiss National Science Foundation, and the Swiss Parkinson Foundation. Cognitive Drug Research(CDR) provided the test battery and computers required for free.
G.M. received a research grant in excess of $10,000 from CDR for the programming of the test battery used in the present study. K.A.W. is the Chiefexecutive of CDR. I.G.M. has previously received research support from CDR.
Received May 8, 2004. Accepted in final form August 13, 2004.
Address correspondence and reprint requests to Dr. Urs P. Mosimann, Institute for Ageing and Health, Wolfson Research Centre, Newcastle GeneralHospital, Newcastle upon Tyne NE4 6BE, UK; e-mail: [email protected]
Copyright 2004 by AAN Enterprises, Inc. Table 1 Demographics and clinical description of the sample
Post-hoc Bonferroni tests compared NC vs PD, PDD vs PD, PDD vs DLB, PDD vs AD, and DLB vs AD, and significant group differ-ences are reported.
* PDD vs AD: p ϭ 0.047; DLB vs AD: p ϭ 0.001. † PDD vs PD Ͻ 0.0001. ‡ PD vs NC Ͻ 0.0001; PDD vs AD: p Ͻ 0.0001; DLB vs AD: p Ͻ 0.0001. § PDD vs PD Ͻ 0.0001; PDD vs AD: p ϭ 0.001; DLB vs AD: p ϭ 0.027. ¶ PDD vs PD Ͻ 0.0001; DLB vs AD: p ϭ 0.026.
NC ϭ normal controls; PD ϭ non-demented Parkinson disease; PDD ϭ Parkinson disease dementia; DLB ϭ Dementia with Lewy bod-ies; AD ϭ Alzheimer disease; NS ϭ not significant (p Ͼ 0.05); MMSE ϭ Mini-Mental State Examination; UPDRS ϭ Unified ParkinsonDisease Rating Scale; NPI ϭ Neuropsychiatric Inventory; Fluctuation ϭ One Day Fluctuation Assessment Scale; Bristol-ADL ϭ BristolActivities of Daily Living scale.
and visuoperceptual impairments, all tasks used in
cluded spiral, pentagon, three-dimensional house and clock copy-
the present study did not require motor responses
ing. Parkinsonism in DLB was defined as bradykinesia, plus oneor more of rest tremor, muscular rigidity, and postural instability
and were not time driven. Based on previous neuro-
without other explanation. Severity of extrapyramidal features
imaging findings,15,16 we hypothesized similar visual
was assessed with the Unified PD Rating Scale (UPDRS) motor
impairments in PDD and DLB and expected impair-
score (part III).22 A cutoff score of more than 6 in the one-day
ments to exceed those of matched AD patients.
fluctuation assessment scale defined fluctuation.23 The Neuropsy-chiatric Inventory (NPI)24 was used to determine whether a sub-ject was experiencing recurrent visual hallucinations during the
Methods.
All subjects were recruited from the New-
month previous to the assessment. Analyzing questions 2 or 3 in
castle MRC prospective outpatient cohort.2 Characteristics of the
the hallucination section of the NPI identified recurrent visual
sample are summarized in table 1. The UK PD Society Brain
hallucinations. In patients with recurrent visual hallucinations,
Bank Clinical Diagnostic Criteria17 were used to make the diagno-
the caregiver agreed with either of these questions and reported a
sis of PD, the National Institute of Neurologic and Communicative
frequency and severity of at least one. The Bristol Activities of
Disorders and Stroke and AD and Related Disorders Association
Daily Living Scale (Bristol ADL)25 was used to assess impairments
(NINCDS-ADRDA)18 for AD, and the DLB Consensus guidelines
in activities of daily living. The neuro-ophthalmologic assessment
for DLB,19 following the recommendation that patients with par-
included external inspection of the eyes, assessment of pupil reac-
kinsonian features preceding cognitive impairment for more than
tions, light reflex (penlight), measurement of near vision (Landolt
12 months should be diagnosed with PDD.19 PDD patients had to
broken rings, test distance 40 cm), assessment of ocular move-
have PD for more than 12 months before developing dementia.19
ments, and estimation of the visual field by confrontation test.
Patients were required to have a caregiver providing regular care
The red reflex and ocular fundus were assessed with direct
and support and to score at least 10 on the Mini-Mental StateExamination (MMSE).
20 Subjects with coexisting medical illness
or a history of visual impairment due to cataract, glaucoma, or
macular degeneration were excluded. The only antiparkinsonian
presented in a multiple-choice format on a 14-inch computer
medication allowed was levodopa. Patients stabilized on cholines-
screen in a standardized, darkened environment. Subjects sat 40
terase inhibitors (ChE-I) were eligible for the study provided they
cm in front of the computer screen. Tasks were not time driven,
were on a stable dose for more than 3 months. The percentage of
subjects responded verbally, and the examiner handled all but-
demented patients on long-term ChE-I was not different between
tons. The instruction of each task was read while an example was
the diagnostic groups (PDD: 58%, DLB: 65%, and AD: 69%). All
presented on the screen. Once the correct answer was given, the
patients with PDD were treated with levodopa, but only 43% of
task started and no further feedback was given. Different random
DLB were on dopaminergic treatment. Of 146 subjects invited,
arrangements of stimulus presentation were used in each task.
118 gave written informed consent; 2 patients had to be excluded
The assessment lasted about 30 to 45 minutes. Figure E-1 on the
because they did not understand the task instructions. The local
Neurology Web site (www.neurology.org) gives an overview of all
research ethics committee granted ethical approval.
Global cognitive impairment was assessed with
Length and size discrimination tasks.
the Cambridge Cognitive Examination (CAMCOG)21 and for the
Pairs of lines/circles were presented side-by-side on the screen and
purpose of this study, tests assessing apraxia were analyzed sepa-
subjects had to decide which of the lines/circles, left or right, were
rately from tests measuring visuoconstructional ability, i.e.,
longer/larger. The stimulus field dimensions were 140 mm wide
praxis and construction scores. CAMCOG visual construction in-
and 150 mm tall. Reference stimulus (70 mm) and comparison
December (1 of 2) 2004
stimulus were separated by 70 mm and the position of the longer
pathway (space-motion perception score). The Statistical Package
line/larger circle varied randomly. To eliminate cues based on the
for Social Sciences (SPSS Version 11) was used for statistical
absolute position of the stimulus features such as end-lines, the
analysis. The distribution of the data was examined for normality
position of each stimulus was randomly jittered from trial to trial
(Kolmogorov-Smirnov test). Provided the data did not deviate
with a diameter of 7 mm. The test used an adaptive psychophysi-
from normal distribution, the five groups were compared with
cal procedure to find the stimulus difference required for a subject
parametric tests (i.e., one-way analysis of variance [ANOVA]) and
to achieve reliable discrimination. Each correct response led to a
subsequently post hoc Bonferroni tests were used for two-group
decrease in the stimulus difference for the next trial (by 1 mm),
comparisons. Means and SD were calculated to represent central
and each incorrect response led to an increase in the difference for
tendency and dispersion. Pearson-rank-correlation was used for
the next trial (by 3 mm). As a result, the test converged on an
correlative analysis. All reported p values were two-tailed and a p
estimate of the threshold, expressed as difference of size or length
value of less than 0.05 was considered statistically significant.
(in %), that the subject detected with 75% accuracy.26 Thirteentrials were presented in each task. Results.
were well matched with respect to age, sex, and education
of Benton’s task.27 Our task used 5 (instead of 11) standard linesat 30 deg (instead of 18 deg) intervals, with subjects judging one
and the three dementia groups did not differ in global
comparison line (instead of two) in each trial. The stimulus field
cognitive impairment (see table 1). Compared to the AD
dimensions were 180 mm wide and 150 mm tall. Twenty trials
group, the DLB and PDD groups had higher UPDRS motor
were presented. Subjects were required to match the angle of the
scores, higher fluctuation scores, shorter dementia dura-
single line to one of five lines forming a semicircle.
tion, and greater impairment in activities of daily living
overlapping figures task was described by De Renzi et al.28 In each
(Bristol ADL). No differences in these scores were found
trial a series of four unique pictures of animals, utensils, clothing,
when DLB was compared with PDD. The frequencies of
or fruits were presented on the screen and subjects decided which
the core clinical features—fluctuation of cognition (PDD
of the four pictures was included in the simultaneously presented
54%; DLB 35%; AD 8%), recurrent visual hallucinations
overlapping figure. The stimulus field dimensions were 180 mmwide and 150 mm tall. Thirteen trials were presented.
(PDD 75%; DLB 90%; AD 8%), and extrapyramidal fea-
tures (PDD 100%; DLB 85%; AD 13%)—were similar in the
block design subtest.29 Two boxes with slightly different forms
DLB and PDD groups (chi square or Fisher’s exact t-test:
were presented side-by-side and the subject had to decide in which
p Ͼ 0.05; NS) but different from AD (Fisher’s exact t-test
quadrant the two boxes were different. Stimuli were not matchedsystematically for mean luminance. Each box was 60 mm wide
for comparison PDD vs AD and DLB vs AD: p Ͻ 0.05).
and 60 mm tall, and the two boxes were separated by 20 mm.
Visual acuity did not differ between groups (controls
0.40 Ϯ 0.16; PD 0.40 Ϯ 0.14; PDD 0.34 Ϯ 0.11; DLB 0.37 Ϯ
0.18; AD 0.42 Ϯ 0.17) (ANOVA: NS) and other neuro-ophthal-
based on the dot position task of Warrington and James.30 In eachtrial, two squares were presented side-by-side, one containing a
mologic assessments did not reveal impairments interfer-
dot and the other five different numbers at random position. The
position of the dot exactly matched the position of a number and
Table 2 summarizes CAMCOG data. One-way ANOVA
the subject was required to name this number. Each square was
revealed significant group differences in all except the
70 ϫ 70 mm and the squares were separated by 30 mm. Thirteen
praxis score. PD was similar to controls and different from
PDD in all but the CAMCOG abstract thinking score. In
signed to match those used in Vaina31 as closely as possible. In
abstract thinking PD were similar to PDD and more im-
each trial, two black squares (70 ϫ 70 mm) were presented side by
paired than controls. Group comparison did not reveal any
side on the screen, separated by 30 mm. Each square contained 12
differences between PDD and DLB. Compared to AD, PDD
small (3 mm diameter) white dots in random positions, moving inrandom directions and bouncing off the sides of the square. Within
and DLB patients were significantly less impaired in mem-
a square all dots moved with the same velocity, but the dots
ory scores, but more impaired in the visual construction
moved with different velocities in the two squares. Four velocities
scores, and the DLB group scored lower in the perception
were presented: 15 mm/second, 20 mm/second, 44.8 mm/second,
score compared to AD. Visual construction CAMCOG
and 60 mm/second. The velocity ratios were the ratio of two differ-
scores did not correlate with UPDRS-motor scores in PDD
ent velocities presented in a trial: 1.33 ϭ 20/15; 2.24 ϭ 44.8/20; 3
ϭ 60/20. When the ratio was 3, for example, all dots in one square
group (Pearson correlation: r ϭ Ϫ0.190, p Ͼ 0.05, NS) but
moved at three times faster than the dots in the other square. The
correlated in the DLB group (Pearson correlation: r ϭ
side on which each velocity appeared was selected randomly.
There were 12 trials—i.e., four presentations of each velocity ra-
tio—and subjects determined which of the two squares containedthe faster moving dots.
form, and space-motion perception are summarized in the
figure, A through C. Visual discrimination scores (z-
visual counting task used by Fujimori et al.32 The stimulus in each
values) were different between the groups (ANOVA: p Ͻ
trial consisted of 10 to 12 colored shapes (white, green, blue,
0.0001) and DLB and PDD patients were more impaired
triangles and squares). There were between 1 and 5 target stimuli
than AD (post-hoc Bonferroni tests: DLB vs AD: p ϭ 0.007;
in each trial (average 3.5). In each of the 13 trials the subjectneeded to count the number of shapes containing one of five pos-
PDD vs AD: p ϭ 0.051), but were not different from each
sible attributes (e.g., how many squares). The stimulus field di-
other (post-hoc Bonferroni tests PDD vs DLB: NS) (see
figure 1A). Between-group differences were also found in
Outcome measures were errors (in percent) in
object-form and space-motion perception (ANOVA: p Ͻ
all tasks except the line and size discrimination tasks. Standard-ized z-values were calculated to compare thresholds in the size/
0.0001). The impairment in object-form perception (see fig-
length discrimination tasks and percentage of errors in the angle
ure 1B) of PDD and DLB patients was greater compared
discrimination task. The mean of the three z-values was the dis-
with AD patients (post-hoc Bonferroni tests: DLB vs AD:
crimination score. To get a measure of the impairment in the
p ϭ 0.003; PDD vs AD: p ϭ 0.001), but not different in
ventral visual pathway, mean errors of the overlapping figure and
DLB and PDD patients (post-hoc Bonferroni tests PDD vs
form perception tasks were calculated (object-form perceptionscore). The mean errors in motion, dot position, and visual count-
DLB: NS). Space-motion perception (see figure 1C) re-
ing tasks were a measure of the impairment in the dorsal visual
vealed a similar pattern of impairment in that the DLB
December (1 of 2) 2004 Table 2 CAMCOG data
Post-hoc Bonferroni tests compared NC vs PD, PDD vs PD, PDD vs DLB, PDD vs AD, and DLB vs AD, and significant group differ-ences are reported:
* PDD vs PD: p Ͻ 0.0001; PDD vs AD: p ϭ 0.004. † PDD vs PD: p Ͻ 0.0001. ‡ NC vs PD: p ϭ 0.01. § PDD vs PD: p Ͻ 0.0001; PDD vs AD: p ϭ 0.006; DLB vs AD: p ϭ 0.002. ¶ PDD vs PD: p Ͻ 0.0001; DLB vs AD: p Ͻ 0.0001.
PDD vs PD: p Ͻ 0.0001; PDD vs AD: p Ͻ 0.001; DLB vs AD: p ϭ 0.003.
CAMCOG ϭ Cambridge Cognitive Examination Scale; NC ϭ normal controls; PD ϭ non-demented Parkinson disease; PDD ϭ Parkin-son disease dementia; DLB ϭ Dementia with Lewy bodies; AD ϭ Alzheimer disease; NS ϭ not significant (p Ͼ 0.05).
group did not differ from PDD but tended to be more im-
ble 3. Global cognitive impairment of patients with visual
paired compared to AD (post-hoc Bonferroni tests: DLB vs
hallucinations (MMSE) was not different from patients
AD: p ϭ 0.074). PD was similar to controls but less im-
without hallucinations and the two groups did not differ
paired than PDD in all scores (post-hoc Bonferroni tests for
with regard to education, frequency of extrapyramidal
all: p Ͻ 0.0001). The PDD group made more errors in
symptoms, or fluctuation. Patients with RVH were signifi-
object-form perception compared to space-motion percep-
cantly more impaired in visual discrimination, space-
tion (paired sample t-test: p Ͻ 0.0001), a difference also
motion perception, and object-form perception compared to
found in the DLB group (paired sample t-test: p Ͻ 0.0001)
patients without visual hallucinations.
but not in the AD group (paired sample t-tests: NS). The
Within each dementia group, patients on ChE-I did not
raw data of all tasks are summarized in table E-1 on the
perform differently compared to patients not taking ChE-I
in visual discrimination, object-form perception, or space-
There were few patients without recurrent hallucina-
motion perception. DLB patients taking levodopa did not
tions (RVH) in the DLB and PDD groups; therefore the
differ in any visual score compared to those patients not
PDD and DLB groups were pooled to compare patients
taking levodopa; such comparison was not feasible in PDD,
with and without hallucinations. Results are shown in ta-
since all patients were taking levodopa. Figure. (A through C) Mean and 95% CI of the discrimination score (A), of errors in object-form perception (B), and er-rors in space-motion perception (C). There was no difference in any of these scores between the DLB and PDD groups, butDLB and PDD tended to perform worse compared to AD patients. PDD and DLB patients made more errors in object-form perception than in space-motion perception. NC ϭ normal controls; PD ϭ Parkinson disease; PDD ϭ PD dementia;DLB ϭ Dementia with Lewy bodies; AD ϭ Alzheimer disease.December (1 of 2) 2004 Table 3 Comparison of DLB/PDD patients with and without recurrent visual hallucinations (RVH)
Values are mean Ϯ SD. DLB ϭ Dementia with Lewy bodies; PDD ϭ Parkinson disease dementia; NS ϭ not significant (p Ͼ 0.05); MMSE ϭ Mini-Mental StateExamination. Discussion.
Visual impairments in DLB patients with visual
tients with PDD and DLB compared with AD and
hallucination exceed those without hallucination, es-
two control groups—NC and nondemented PD pa-
pecially in the overlapping figure task39 and in the
tients. PDD and DLB had similar visuoperceptual
line orientation task.40 Barnes and David41 compared
impairments but were more impaired compared to
visual imagery, visual perception, and recognition
patients with AD. Visual perception of PDD/DLB pa-
memory in nondemented PD patients with and with-
tients with visual hallucinations was worse than in
out hallucinations and found that PD patients with
visual hallucinations were more impaired in object
Combined retinal and cortical changes need to be
perception. In the present study, hallucinating DLB/
addressed to understand the extent of perceptual im-
PDD patients were more impaired in all visual
pairment affecting all test scores. PDD and DLB are
scores compared to patients without hallucinations.
both associated with profound cortical cholinergic
The interpretation of this finding needs caution, be-
deficits and cortical Lewy body pathology in areas
cause as in previous studies,39,40 the number of de-
involved in visual perception33,34 and functional im-
mented patients without hallucinations in this study
aging studies have reported hypoperfusion in the oc-
The neuropsychological (CAMCOG) data confirm
consistently exceeding those found in AD.15,16 These
previous findings showing that visuoconstructional
findings suggest abnormal function of visual cortical
abilities are more impaired in PDD and DLB com-
areas. Additional retinal changes cannot be ex-
pared to AD and that memory function is relatively
cluded, since some visual abnormalities, such as im-
preserved.11,42,43 In contrast to most previous studies,
paired contrast vision, are mediated by disruption of
which reported additional frontal impairment in
dopaminergic processes in the retina35,36 and are un-
PDD and DLB, we did not find differences in the
likely to be discovered during routine neurologic ex-
attentional scores. The numerical tasks used to as-
amination or by ordinary high contrast visual acuity
sess attention in the CAMCOG battery may be in-
The dissociation between performance in object-
demented patients. One study44 which compared the
form and space-motion perception found in PDD and
cognitive profile of AD and DLB patients using the
DLB but not in AD patients may indicate a deficit in
CAMCOG battery also did not find attentional differ-
the ventral visual pathway in these groups. This
ences. Since CAMCOG visual construction scores in
finds support in studies reporting profound cholin-ergic deficits and greater Lewy body density in the
DLB also correlated with the severity of extrapyra-
temporal lobes.34,37,38 However, it is possible that the
midal motor symptoms, it is likely that some of the
differences observed are partly related to non-
visual constructional impairment is related to motor
specific visuocognitive deficits. Object-form percep-
impairment in the DLB group. This underpins the
tion tasks may be more sensitive than space-motion
need for tasks that are independent of motor func-
perception tasks because they may contain more vi-
tion when testing visual perception in patients with
sual information or require more complicated solu-
combined extrapyramidal and cognitive impairment.
tion strategies.10 The better perfusion seen onSPECT imaging in DLB/PDD in the ventral stream
Acknowledgment
compared with the dorsal stream16 does not necessar-ily equate with better function, since it may reflect
The authors thank the patients and controls for their participa-tion, Lorraine Bowman for help with testing, Daniel Collerton for
compensatory increase in activity in structurally al-
help with data analysis, Simon Kometa for statistical advice, and
Jordan Bowen for help with recruiting. December (1 of 2) 2004 References
21. Roth M, Tym E, Mountjoy CQ, et al. CAMDEX. A standardised instru-
ment for the diagnosis of mental disorder in the elderly with special refer-
1. Aarsland D, Andersen K, Larsen JP, Lolk A, Kragh-Sorensen P. Preva-
ence to the early detection of dementia. Br J Psychiatry 1986;149:698 –709.
lence and characteristics of dementia in Parkinson disease: an 8-year
22. Fahn S, Elton R, UPDRS program members. Unified Parkinson’s dis-
prospective study. Arch Neurol 2003; 60:387–392.
ease rating scale. Florham Park, NJ: Macmillan Healthcare Informa-
2. Burn DJ, Rowan EN, Minett T, et al. Extrapyramidal features in Parkin-
son’s disease with and without dementia and dementia with Lewy bodies:
23. Walker MP, Ayre GA, Cummings JL, et al. The Clinician Assessment of
a cross-sectional comparative study. Mov Disord 2003;18:884 – 889.
Fluctuation and the One Day Fluctuation Assessment Scale. Two meth-
3. Ballard CG, Aarsland D, McKeith I, et al. Fluctuations in attention: PD
ods to assess fluctuating confusion in dementia. Br J Psychiatry 2000;
dementia vs DLB with parkinsonism. Neurology 2002;59:1714 –1720.
4. Aarsland D, Laake K, Larsen JP, Janvin C. Donepezil for cognitive
24. Cummings JL, Mega M, Gray K, Rosenberg-Thompson S, Carusi DA,
impairment in Parkinson’s disease: a randomised controlled study.
Gornbein J. The Neuropsychiatric Inventory: comprehensive assess-
J Neurol Neurosurg Psychiatry 2002;72:708 –712.
ment of psychopathology in dementia. Neurology 1994;44:2308 –2314.
5. McKeith I, Del Ser T, Spano P, et al. Efficacy of rivastigmine in demen-
25. Bucks RS, Ashworth DL, Wilcock GK, Siegfried K. Assessment of activ-
tia with Lewy bodies: a randomised, double-blind, placebo-controlled
ities of daily living in dementia: development of the Bristol Activities of
international study. Lancet 2000;356:2031–2036.
Daily Living Scale. Age Ageing 1996;25:113–120.
6. Starkstein SE, Sabe L, Petracca G, et al. Neuropsychological and psy-
26. Kaernbach C. Simple adaptive testing with the weighted up-down
chiatric differences between Alzheimer’s disease and Parkinson’s dis-
method. Percept Psychophys 1991;49:227–229.
ease with dementia. J Neurol Neurosurg Psychiatry 1996;61:381–387.
27. Benton AL, Varney NR, Hamsher KD. Visuospatial judgment. A clini-
7. Mohr E, Litvan I, Williams J, Fedio P, Chase TN. Selective deficits in
cal test. Arch Neurol 1978;35:364 –367.
Alzheimer and parkinsonian dementia: visuospatial function. Can
28. De Renzi E, Scotti G, Spinnler H. Perceptual and associative disorders
of visual recognition. Relationship to the side of the cerebral lesion.
8. Gnanalingham KK, Byrne EJ, Thornton A, Sambrook MA, Bannister P.
Motor and cognitive function in Lewy body dementia: comparison with
29. Caplan B, Caffery D. Fractionating block design: development of a test
Alzheimer’s and Parkinson’s diseases. J Neurol Neurosurg Psychiatry
of visuospatial analysis. Neuropsychology 1992;6:385–394.
30. Warrington EK, James M. Visual apperceptive agnosia: a clinico-
9. Pillon B, Dubois B, Ploska A, Agid Y. Severity and specificity of cogni-
anatomical study of three cases. Cortex 1988;24:13–32.
tive impairment in Alzheimer’s, Huntington’s, and Parkinson’s diseases
31. Vaina LM. Selective impairment of visual motion interpretation follow-
and progressive supranuclear palsy. Neurology 1991;41:634 – 643.
ing lesions of the right occipito-parietal area in humans. Biol Cybern
10. Crucian GP, Okun MS. Visual-spatial ability in Parkinson’s disease.
32. Fujimori M, Imamura T, Yamashita H, Hirono N, Mori E. The distur-
11. Collerton D, Burn D, McKeith I, O’Brien J. Systematic review and
bances of object vision and spatial vision in Alzheimer’s disease. De-
meta-analysis show that dementia with Lewy bodies is a visual-
ment Geriatr Cogn Disord 1997;8:228 –231.
perceptual and attentional-executive dementia. Dement Geriatr Cogn
33. Bohnen NI, Kaufer DI, Ivanco LS, et al. Cortical cholinergic function is
more severely affected in parkinsonian dementia than in Alzheimer
12. Cormack F, Aarsland D, Ballard C, Tovee MJ. Pentagon drawing and
disease: an in vivo positron emission tomographic study. Arch Neurol
neuropsychological performance in dementia with Lewy bodies, Alzhei-
mer’s disease, Parkinson’s disease and Parkinson’s disease with demen-
34. Harding AJ, Broe GA, Halliday GM. Visual hallucinations in Lewy
tia. Int J Geriatr Psychiatry 2004;19:371–377.
body disease relate to Lewy bodies in the temporal lobe. Brain 2002;
13. Wurtz RH, Kandel ER. Central visual pathways. In: Kandel ER,
Schwartz JH, Jessell TM, eds. Principles of neural science. Fourth ed.
35. Nguyen-Legros J. Functional neuroarchitecture of the retina: hypothe-
New York: McGraw-Hill, 2000;523–547.
sis on the dysfunction of retinal dopaminergic circuitry in Parkinson’s
14. Ungerleider LG, Haxby JV. ‘What’ and ‘where’ in the human brain.
disease. Surg Radiol Anat 1988;10:137–144.
Curr Opin Neurobiol 1994;4:157–165.
36. Bodis-Wollner I, Tagliati M. The visual system in Parkinson’s disease.
15. Donnemiller E, Heilmann J, Wenning GK, et al. Brain perfusion scin-
tigraphy with 99mTc-HMPAO or 99mTc-ECD and 123I-beta-CIT
37. Perry EK, Irving D, Kerwin JM, et al. Cholinergic transmitter and
single-photon emission tomography in dementia of the Alzheimer-type
neurotrophic activities in Lewy body dementia: similarity to Parkin-
and diffuse Lewy body disease. Eur J Nucl Med 1997;24:320 –325.
son’s and distinction from Alzheimer disease. Alzheimer Dis Assoc Dis-
16. Firbank MJ, Colloby SJ, Burn DJ, McKeith IG, O’Brien JT. Regional
cerebral blood flow in Parkinson’s disease with and without dementia.
38. Tiraboschi P, Hansen LA, Alford M, et al. Cholinergic dysfunction in
diseases with Lewy bodies. Neurology 2000;54:407– 411.
17. Gibb WR, Lees AJ. The relevance of the Lewy body to the pathogenesis
39. Mori E, Shimomura T, Fujimori M, et al. Visuoperceptual impairment
of idiopathic Parkinson’s disease. J Neurol Neurosurg Psychiatry 1988;
in dementia with Lewy bodies. Arch Neurol 2000;57:489 – 493.
40. Simard M, van Reekum R, Myran D. Visuospatial impairment in de-
18. McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan
mentia with Lewy bodies and Alzheimer’s disease: a process analysis
EM. Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-
approach. Int J Geriatr Psychiatry 2003;18:387–391.
ADRDA Work Group under the auspices of Department of Health and
41. Barnes J, David AS. Visual hallucinations in Parkinson’s disease: a
Human Services Task Force on Alzheimer’s Disease. Neurology 1984;
review and phenomenological survey. J Neurol Neurosurg Psychiatry
19. McKeith IG, Galasko D, Kosaka K, et al. Consensus guidelines for the
42. Emre M. Dementia associated with Parkinson’s disease. Lancet Neurol
clinical and pathologic diagnosis of dementia with Lewy bodies (DLB):
report of the consortium on DLB international workshop. Neurology
43. McKeith I, Mintzer J, Aarsland D, et al. Dementia with Lewy bodies.
20. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state.” A practical
44. Walker Z, Allen RL, Shergill S, Katona CL. Neuropsychological perfor-
method for grading the cognitive state of patients for the clinician.
mance in Lewy body dementia and Alzheimer’s disease. Br J Psychiatry
December (1 of 2) 2004
2MB 82.69% 2MN 84.15% 3CW 97.93% 3SS 90.34% 4SS 96.90% 4PH 95.56 % Mansfield Green News WINNER : 3CW We are nearly at the end of the year and I would like to thank you all for your support throughout this year. School has come a long way and you have helped us to get there. Standards are improving and I know that the Staff have worked very hard on Overall At
Association for Responsible Health Information and Advertising (ARHIA) 1. The Director General Department of Health; 2. The Registrar Medicines Control Council; Private Bag X828 PRETORIA 0001 23 October 2011 Dear Madame Director General, Dear Mrs Hela, Complementary Medicines: Regulations and Guidelines I am writing on behalf of the Association for Responsible Health I
 Visual perception in Parkinson disease
Visual perception in Parkinson disease Table 1 Demographics and clinical description of the sample
Table 1 Demographics and clinical description of the sample stimulus were separated by 70 mm and the position of the longer
pathway (space-motion perception score). The Statistical Package
line/larger circle varied randomly. To eliminate cues based on the
for Social Sciences (SPSS Version 11) was used for statistical
absolute position of the stimulus features such as end-lines, the
analysis. The distribution of the data was examined for normality
position of each stimulus was randomly jittered from trial to trial
(Kolmogorov-Smirnov test). Provided the data did not deviate
with a diameter of 7 mm. The test used an adaptive psychophysi-
from normal distribution, the five groups were compared with
cal procedure to find the stimulus difference required for a subject
parametric tests (i.e., one-way analysis of variance [ANOVA]) and
to achieve reliable discrimination. Each correct response led to a
subsequently post hoc Bonferroni tests were used for two-group
decrease in the stimulus difference for the next trial (by 1 mm),
comparisons. Means and SD were calculated to represent central
and each incorrect response led to an increase in the difference for
tendency and dispersion. Pearson-rank-correlation was used for
the next trial (by 3 mm). As a result, the test converged on an
correlative analysis. All reported p values were two-tailed and a p
estimate of the threshold, expressed as difference of size or length
value of less than 0.05 was considered statistically significant.
stimulus were separated by 70 mm and the position of the longer
pathway (space-motion perception score). The Statistical Package
line/larger circle varied randomly. To eliminate cues based on the
for Social Sciences (SPSS Version 11) was used for statistical
absolute position of the stimulus features such as end-lines, the
analysis. The distribution of the data was examined for normality
position of each stimulus was randomly jittered from trial to trial
(Kolmogorov-Smirnov test). Provided the data did not deviate
with a diameter of 7 mm. The test used an adaptive psychophysi-
from normal distribution, the five groups were compared with
cal procedure to find the stimulus difference required for a subject
parametric tests (i.e., one-way analysis of variance [ANOVA]) and
to achieve reliable discrimination. Each correct response led to a
subsequently post hoc Bonferroni tests were used for two-group
decrease in the stimulus difference for the next trial (by 1 mm),
comparisons. Means and SD were calculated to represent central
and each incorrect response led to an increase in the difference for
tendency and dispersion. Pearson-rank-correlation was used for
the next trial (by 3 mm). As a result, the test converged on an
correlative analysis. All reported p values were two-tailed and a p
estimate of the threshold, expressed as difference of size or length
value of less than 0.05 was considered statistically significant.
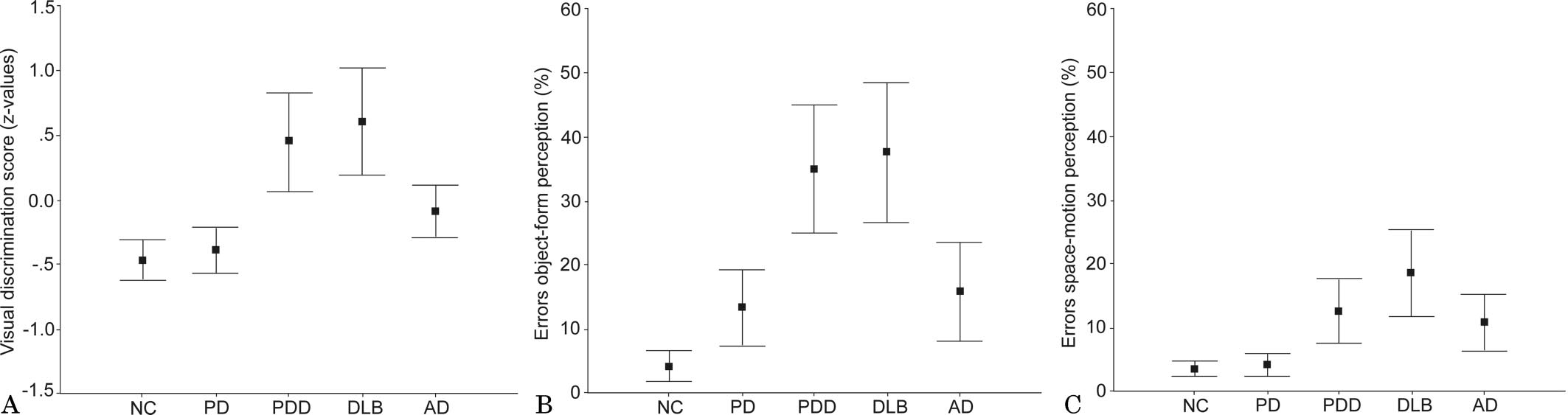 Table 2 CAMCOG data
Table 2 CAMCOG data Table 3 Comparison of DLB/PDD patients with and without recurrent visual hallucinations (RVH)
Table 3 Comparison of DLB/PDD patients with and without recurrent visual hallucinations (RVH) References
References