Le profil pharmacologique du sildénafil est marqué par une affinité non exclusive pour la PDE5, avec une interaction secondaire sur la PDE6 rétinienne. Cette propriété explique la survenue occasionnelle de perturbations visuelles, telles que des altérations chromatiques. Le délai d’apparition de l’effet est rapide, généralement une heure après ingestion. Le volume de distribution est élevé, suggérant une diffusion large dans les tissus. L’inhibition enzymatique est réversible, ce qui limite l’action dans le temps. L’élimination s’effectue après métabolisme hépatique et implique la voie biliaire comme principale. Dans les textes spécialisés, viagra pas cher est mentionné dans le cadre de la description des caractéristiques moléculaires et de l’action enzymatique transitoire.
Morbid obesity surgery info doc ver 2.2 aug 2009
Mercy Bariatrics Morbid obesity surgery Introduction By the time you have considered surgery for your obesity, you will probably have been battling with a weight problem most of your life. You may have tried all manner of diets, joined Weight Watchers or Jenny Craig’s and even tried acupuncture or hypnotherapy. Perhaps you have been prescribed appetite suppressants, antidepressants, Xenical or stimulants. If you are like most patients, any limited success you will have had with these techniques has been temporary and any lost weight rapidly regained and then exceeded! The simple truth is that the reason you suffer from morbid obesity is not that you are greedy, or lazy or slothful or any of the other negative misconceptions that a lot of people have about obesity. The main factor in morbid obesity is that your metabolism is genetically programmed to very efficiently lay down extra calories as fat. In the days of the caveman this was a distinct survival advantage……. In our world, with such free access to food, it results in a severe weight problem. A very few people, with the discipline of Ghandi and the endurance of Kieren Perkins might be able to overcome this programming by rigidly sticking to a diet. The majority cannot. Morbid obesity surgery is designed principally to make it easier for you to sufficiently modify your food intake to bring your weight down to a safer and more comfortable range. Why perform surgery for morbid obesity? Morbid obesity surgery is not cosmetic surgery. All doctors recognize that once a patient’s weight exceeds a certain range they are more likely to suffer from a wide range of illnesses such as diabetes, sleep apnoea, asthma, hypertension, arthritis, varicose veins and skin problems. Their chances of dying at a premature age, is also greatly increased. Their employment prospects, mobility and social acceptance also suffer. Depression is much more common in the morbidly obese. The main aim of this surgery is to bring your weight down to a safer range where most of these associated conditions are reduced in severity and many completely reversed. Along the way most people find an improvement in their mobility, body image, self-esteem and enjoyment of life. Who is a candidate for this surgery? There are a number of widely accepted criteria which make a patient suitable for this operation: • Weight greater than 45kg above the ideal body weight for sex, and height.
• BMI (Body mass index = wt (kg) / height (m)2 ) > 40 by itself, or >35 if there is an associated obesity
illness, such as diabetes or sleep apnoea. Sometimes, under special circumstances, we will accept people for surgery with BMI 30-35.
• Reasonable attempts at other weight loss techniques
• No psychiatric or drug dependency problems
• A capacity to understand the risks and commitment associated with the surgery. What type of surgery is done? Obesity surgery has been refined over several decades by a trial and error process. There are dozens of different operations and most Bariatric Surgeons concentrate on one or two varieties, which they have confidence in. Basically, most of these operations involve the following principles: A.
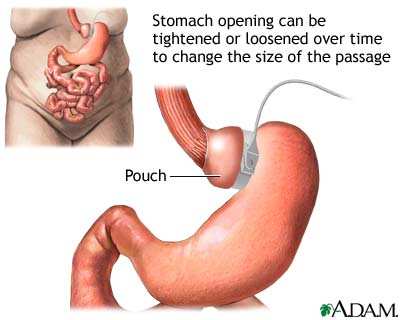
Gastric Restrictional Surgery (Stomach banding)
Lap Band
Advantages:
• Keyhole approach …. Less scarring or wound problems
• Adjustable : by filling port the outlet size can be reduced
• Reversible: By removing fluid or the band.
• Lowest risk 1:2500 surgical mortality Disadvantages:
• Easy to cheat …. if chocolates or sweets taken.
• Some foods can get stuck e.g. steak and bread
• Mechanical problems: prolapse, pouch dilatation,
slippage of the stomach through the band, erosion, infection
Revision rate? 10 -20%
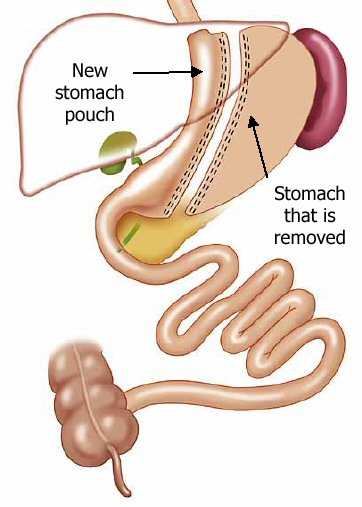
Ideal Gastric Pouch capacity 30mls Predicted Excess Weight Loss (EWL) 50-60% over 2 yrs. Laparoscopic “ Tube “ Gastrectomy ( Gastric Reductive operation)
A “reductive operation” : The stomach is reduced in size from a 1000mls bag to a 150-200 ml tube.
This is the first part of the BPD-DS (see over) and can be done with keyhole surgery
Advantages:
• Keyhole operation :4 days in hospital. Back at work 1-2 weeks
• Simply reduces the amount of food not the type of food
• Normal stomach emptying therefore no vomiting
• “Set and forget” operation : no adjustments required
• The Duodenal switch or gastric bypass can be added later if insufficient
• A good revision option in failed lap band
Disadvantages:
• Possible long term weight regain if tube stretches up
• Relatively new operation so long term results not defined
• Risk of bleeding or staple line leak immediately after operation
Ideal Gastric capacity 100-150 ml Predicted EWL 60-70% over 2yrs Combined Gastric Reductive and Intestinal Bypass. e.g. Scopinaro procedure and Duodenal switch operation and Gastric Bypass.These are more difficult surgeries and are usually reserved as revision operation for patients who have failed the lap band or sleeve. We do not generally offer them to first time patients.
It is possible to perform The BPD-DS with keyhole surgery in two stages performing the tube stomach first and the bypass 6-12 months later. Current studies indicate that the tube gastrectomy alone produces better weight loss than the lap band (64% EWL by one year) and further weight loss results if the intestinal bypass is then performed. This may be a good option for patients who are super obese ( BMI>50) because it allows all the benefits of Keyhole surgery and better eventual weight loss than a band alone. Which operation is chosen is largely a matter of patient preference but may be influenced by whether you have had previous surgery and what your eating patterns are like. • The most important thing to understand is that all of these operations will result in a dramatic reduction in the amount and rate at which you can eat. On average about a tea saucer full of food will leave you feeling satisfied for several hours. Any more than this and you may vomit or feel uncomfortable. • Although it is possible to undo or reverse some of these operations it is very difficult and most of the lost weight will be regained in six months. It is best to consider these operations as not reversible.
• Surgery only provides part of the cure. You must still be prepared to follow a sensible diet and exercise program. Most people find this becomes easier as their weight is shed. Is this surgery effective? In properly chosen patients, the purely restrictive operations (e.g. lap band) have a long-term success rate of about 60% to 70%. This means losing at least 50% of your excess weight and keeping it off for at least five years. The average excess weight loss with the restrictive operations is about 50-60% depending on the initial degree of obesity. The Gastric sleeve is achieving on average 65-70% EWL measured over 3 years. The more conservative combined procedures (such as the Roux-en-Y gastric bypass) have a long-term success rate approaching 80% and an average excess weight loss of between 60-70%. The Duodenal switch has the greatest weight loss with most people losing 70-90% of their excess weight over two years. This is a graph of my own results over the last 7 years as at Dec 2008. It is the percentage of excess weight lost over time ( Excess weight = Start weight – Ideal weight )
Most failures are due to poor dietary choices on the patient's part (high calorie liquids and/or fried, salty snacks), although a significant percentage of failures are due to a mechanical failure of the surgical procedure itself, such as stretching of the sleeve or pouch above the band.
What are the risks of the surgery?
• All surgery carries some risks and these sorts of operations are technically difficult and demanding.
• The risk of dying from the procedure is less than 1:2500 for the lap band and Lap tube but closer to
• There is a risk of bleeding, stomach or bowel injury or other organ injury from the laparoscopic
instruments or ports leading to peritonitis. This may require a blood transfusion or further surgery.
• There is a risk of leak from the staple lines or joins immediately after surgery. If this occurs you can
become very sick very quickly, you will require further surgery to correct the problem andspend many weeks in hospital recovering and many months before you are well again.
• Very rarely this leak can persist as a chronic fistula to the skin or another organ such as the colon or lung requiring further surgery and interventions.
• Sometimes transfer to another hospital then becomes necessary for reasons of funding or the
requirement for ICU. The leak rate for Primary sleeve Gastrectomy is between 2-3%. For revisional surgery eg band to tube it is as high as 15-20%.
• Other serious complications of this sort of surgery are deep venous thrombosis and pulmonary
embolism (blood clots to the legs and lungs). Any of these complications can be fatal, but fortunately they are uncommon. These complications occur early after surgery and require immediate attention.
• There is the risk of injury to the liver or bile duct during removal of the gallbladder if this is
required. This may result in leakage of bile or blockage of the liver and require further surgery to correct.
• The Spleen may be injured and may need to be removed.
• Minor complications include wound infection and hernias, collapse of the lung bases and bladder
• Late complications include staple line disruption, dilatation of the gastric tube, bowel obstruction
from adhesions and nutritional deficiency including osteoporosis and iron deficiency if supplements are not taken; these are rare and can be corrected. Reflux can become worse after surgery
• If you choose a malabsorptive operation like duodenal switch you will need to take at least two
Multivitamins, two calcium tablets and often two iron Tablets (if still menstruating) for the rest of your life.
• Risks pertaining more to the Lap band are slippage of the band, stretching of the gastric pouch above
the band. Disconnection of the tubing from the port and leakage of the tubing or band. Infection of the band or port and erosion of the band into the stomach. These risks are uncommon but may require repositioning, replacement or removal of your band or port.
These risks will be discussed with you during your consultations and we encourage you to ask questions or seek clarification on areas that concern you. What happens if I decide to proceed?
This is a major decision you are making that will radically affect your life. We will need to meet on more than one occasion to explain the procedures and consequences carefully, assess your health risks and eating behavior and make sure that you have made an informed decision to proceed. You will need to complete our pre-operative program prior to your surgery. This involves additional appointments with other members of the bariatric team including a specialist physician, dietitian, exercise physiologist and anaesthetist. If your BMI is greater than 40, we will usually ask you to undertake a 4-6 week preoperative Very Low Calorie Diet (VLCD) using Clinical to kick start your weight loss and shrink the size of your fatty liver. In some cases an examination of the stomach by endoscopy will be required. Costs:
In most cases the Hospital and theatre costs including purchase of the Lap band will be covered by your Health Fund if you have been a member for more than one year. Without Private Insurance the total cost of the procedure is in excess of $17,000.00, and it may be even more if a complication was to develop which required a prolonged hospital stay. If uninsured, full payment is required prior to surgery. The program and surgeon’s fee depends on which procedure you choose and ranges between $5,500.00 - $6,500.00. Your health fund will only cover a small portion of this. There will also be an out of pocket expense for the Anaesthetist and Surgical Assistant. Full Payment, to cover the Surgeon’s fee, is required prior to all surgery. The out of pocket costs for this surgery are significant, and there are several payment options available to you. There are companies who provide credit for surgical procedures, and accessing your superannuation is another alternative. Our Business Manager will be very happy to answer any queries you have regarding these options.
If you decide to proceed, we will provide you with a complete estimate for the surgical fee and bariatric program. More information can be obtained from the Internet on: www.mercybariatrics.com.au http://www.ossanz.com.au/ http://www.obesitylapbandsurgery.com/index.html http://www.lap-band.com/ There is a complete Video feed of a public information evening held in Jan 2007 on our website. www.mercybariatrics.com.au Key words to search: Lap Band Sleeve gastrectomy Lap tube gastrectomy Biliopancreatic bypass Duodenal switch BPD-DS Scopinaro operation Mr Leon Cohen. MBBS FRACS FRCS August 2009 Telephone: 9272 0420 Fax: 9272 0450 Email: [email protected]
Level 2, Suite 1A, Mercy Medical Centre, Ellesmere Road, Mount Lawley, WA 6050
Obesity information confirmation sheet 2.2 ( Aug 2009) I confirm that I have received and have read the obesity information sheet version 2.2 provided by Mr Leon Cohen, Mr Harsha Chandraratna and Dr Deborah Jenner. I have had the opportunity to ask, and have had answered questions arising from this information sheet. I understand that bariatric surgery is potentially risky and dangerous and complications and side effects can be experienced. There is a risk of death from these procedures or complications which may require hospitalisation for many weeks and further surgery. Transfer to another hospital may then be required. I also understand that, although the significant risks and complications have been described and discussed, it is beyond the scope of this sheet to cover all potential risks and complications from this surgery. I have been warned that the operations do not always work, and I will still need to modify my eating behaviour for maximum benefit. I understand that for the best results and safety, I must commit to regular follow-up and surveillance after surgery, and may require long term vitamin and mineral supplements. I understand that I must complete the Bariatric Program prior to surgery. I agree to have my data, relating to my surgery and follow-up treatment, included in future medical research and publications. I understand that my data will not be associated with my name, address or any other personally identifying information in the research. Only authorised Mercy Bariatrics personnel will have access to my data. Questions arising from this sheet: (Please bring this with you on your next consultation)
Sewage Sludge Contents / Tip of Iceberg Heavy Metals, Pathogens, Synthetic Chemicals, Hydrocarbons, Petrochemicals & Organochlorines, Pharmaceuticals, Steroids & Hormones. This list of contents represents only the “tip of the iceberg” of toxics concentrated in sewage sludge. Federal and most state and local land application regulations limit concentrations of only nine heavy me
土木学会中部支部研究発表会 (2009.3) Sorption of antibiotics and natural estrogens onto reservoir sediment Department of Civil Engineering, Gifu University Graduate School of Engineering, Gifu University River Basin Research Center, Gifu University Department of Civil Engineering, Gifu University 1. Introduction to the laboratory using a core container supplied Veterinary
 What type of surgery is done? Obesity surgery has been refined over several decades by a trial and error process. There are dozens of different operations and most Bariatric Surgeons concentrate on one or two varieties, which they have confidence in. Basically, most of these operations involve the following principles: A.
Gastric Restrictional Surgery (Stomach banding)
What type of surgery is done? Obesity surgery has been refined over several decades by a trial and error process. There are dozens of different operations and most Bariatric Surgeons concentrate on one or two varieties, which they have confidence in. Basically, most of these operations involve the following principles: A.
Gastric Restrictional Surgery (Stomach banding)