Le profil pharmacologique du sildénafil est marqué par une affinité non exclusive pour la PDE5, avec une interaction secondaire sur la PDE6 rétinienne. Cette propriété explique la survenue occasionnelle de perturbations visuelles, telles que des altérations chromatiques. Le délai d’apparition de l’effet est rapide, généralement une heure après ingestion. Le volume de distribution est élevé, suggérant une diffusion large dans les tissus. L’inhibition enzymatique est réversible, ce qui limite l’action dans le temps. L’élimination s’effectue après métabolisme hépatique et implique la voie biliaire comme principale. Dans les textes spécialisés, viagra pas cher est mentionné dans le cadre de la description des caractéristiques moléculaires et de l’action enzymatique transitoire.
Sboc livro 7.qxd
Choque Hemorrágico comoManifestação Inicial de TumorEstromal Gastrointestinal
Mulher de 43 anos é admitida no serviço de emergência por
sangramento e aumentando a chance de recorrência. d) A simples
apresentar quadro de hemorragia digestiva (hematêmese e ente-
enucleação do tumor deve ser evitada. e) Ressecções segmentares
rorragia). Negava episódios prévios, bem como utilização crônica de
do estômago ou intestino devem ser realizadas a fim de se obterem
medicamentos. Previamente hígida. Ao exame: pálida, sudorética
margens microscópicas negativas. f) Margem macroscópica de 1 a
com freqüência cardíaca de 130 bpm, pressão arterial de 90/50
2 cm é suficiente. g) Linfadenectomia raramente é indicada, pois o
mmHg. Realizado ressuscitação volêmica vigorosa (cristalóide e
comprometimento linfonodal é incomum. Em séries que incluem
três unidades de concentrado de hemácias) e iniciado omeprazol.
cirurgias eletivas, a ressecção macroscópica completa é possível
Hemoglobina 4,7 g/dl. Endoscopia digestiva alta demonstrou sangue
em cerca de 85% dos pacientes com tumores localizados. Margens
vermelho vivo refluindo em grande quantidade, distalmente à
microscópicas negativas são obtidas em 70 a 95% desses pacientes.
segunda porção duodenal, em segmento não passível de avaliação
Entretanto, após a ressecção completa, pelo menos 50% dos pacientes
endoscópica. Submetida a laparotomia por instabilidade hemodi-
apresentam recorrência (1). O adequado seguimento pós-opera-
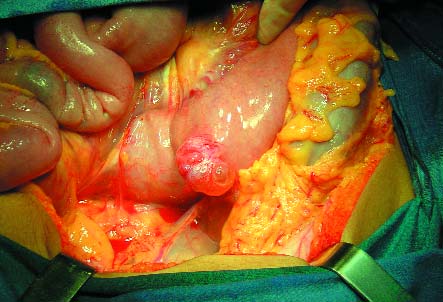
nâmica. Presença de tumoração exofítica ao nível do ângulo de
tório ainda é desconhecido. A utilização da tomografia computa-
Treitz (foto). Realizado enterectomia com entero-entero anastomose
dorizada de abdome e pelve tem sido recomendada a cada 3 a 6
termino-terminal. Resolução do choque. Evolução pós-operatória
meses inicialmente, conforme o potencial de malignidade do tumor,
sem intercorrências. Anatomopatológico: nódulo transmural de
e anualmente a seguir (1-3). O advento do imatinib (inibidor específico
1,7X4,0 cm, com protrusão intra e extraluminal. Envolvimento
da tirosina quinase) trouxe grande avanço no tratamento da doença
transmural por neoplasia fusocelular com focos de degeneração
metastática , com taxa de resposta superior a 50% e estabilização
mixóide e ulceração. Achados sugestivos de tumor estromal gastro-
da doença em mais de 70% dos casos (4, 5). Ensaios clínicos estão em
intestinal (GIST). Imunohistoquímica C-kit positivo – perfil imuno-
andamento avaliando o uso do imatinib como terapia neoadjuvante
histoquímico próprio de GIST. Seis meses após a cirurgia a
bem como a duração de sua manutenção.
paciente encontra-se bem e sem sinais de recorrência.
Apesar de raro, o GIST é o tumor mesenquimal mais freqüente
do trato gastrointestinal. Os GISTs são provavelmente origináriosdas células intersticiais de Cajal, localizadas próximas ao plexomioentérico e presumivelmente o marcapasso da peristalse intestinal. Anteriormente confundidos com leiomiomas e leiomiossarcomas,suas características imunofenotípicas (a mais notável delas omarcador immunohistológico KIT (CD 117) – presente em 95% doscasos) hoje permitem sua correta distinção (1). Os GISTs apresentamuma leve predominância no sexo masculino, com uma média deidade de 60 anos. Podem ocorrer em qualquer local ao longo dotrato gastrointestinal, mas se encontram mais freqüentemente noestômago (65%) ou intestino delgado (25%). Cólon e reto são alocalização de 5 a 10% e esôfago em cerca de 5%. Locais infreqüentesincluem omento, mesentério e retroperitônio. Sua apresentação évariável, cerca de 70% dos pacientes tem sintomas, 20% são assin-tomáticos e 10% são achados em autópsias. Tumores sintomáticostendem a ser maiores e seus sintomas usualmente são inespe-
cíficos e relacionados ao seu efeito de massa ou sangramento. Quando os GISTs erodem para o lúmen do trato gastrointestinal
REFERÊNCIAS
podem induzem hemorragia significativa ou sangramento oculto
1. Gold JS, DeMatteo RP. Combined Surgical and Molecular
nas fezes. Sua ruptura para o peritônio pode causar hemorragia
Therapy: The Gastrointestinal Stromal Tumor Model. Ann
com risco de morte. No presente caso aplicam-se as diretrizes
habituais de investigação e manejo da hemorragia digestiva, bem
2. DeMatteo RP, Brennan MF. Gastrointestinal Stromal Tumors.
como os princípios para adequada ressecção de um GIST. No
In: Cameron JL. Current Surgical Therapy. 8 th ed. Philadelphia,
manejo cirúrgico, mesmo na urgência deve-se obedecer aos seguintes
princípios, conforme ditar a condição clínica do paciente (2):
3. Blay JY, Bonvalot S, Casali P, et al. Consensus meeting for
a) Considerar que a cirurgia representa a única chance de cura.
the management of gastrointestinal stromal tumors: Report of
b) A exploração abdominal deve ser completa, observar principal-
the GIST Consensus Conference of 20-21 March 2004, under
mente o peritônio e fígado (locais freqüentes de metástase). c) A
the auspices of ESMO. Ann Oncol. 2005;16:566 -578.
técnica de ressecção deve ser meticulosa, os GISTs são freqüente-
4. Joensuu H, Roberts PJ, Sarlomo-Rikala M, et al. Effect of the
mente friáveis, sua cápsula rompe facilmente podendo ser causa de
tyrosine kinase inhibitor STI571 in a patient with a metastaticgastrointestinal stromal tumor. N Engl J Med. 2001;344:1052-1056.
5. Demetri GD, Von Mehren M, Blanke CD, et al.: Efficacy and
** Chefe do PRM de Oncologia Cirúrgica do Hospital Nossa Senhora da
safety of imatinib mesylate in advanced gastrointestinal
Conceição. Porto Alegre - RS, Brasil.
stromal tumors. N Engl J Med. 2002;347:472-480.
Rev. Bras. Oncologia Clínica 2006 . Vol. 3 . N.º 7 (Jan/Abr) 37-38 | 37
Hemorrhagic Shock as theInitial Presentation OfGastrointestinal Stromal Tumor
A 43 year-old-woman present to the emergency department
tumor rupture ensuing, increasing the recurrence rate; d) Simple
for sustaining gastrointestinal hemorrhage (hematemesis and
enucleation of the tumor should be avoided; e) Segmental
enterorrhagia). She denies previous episodes, as well as chronic
resection of the stomach or intestine should be performed to
medical usage. She was previously health. Physical examination
achieve negative microscopic margins; f) A 1 to 2 cm grossly
revealed: pallor, diaphoresis, a cardiac rate of 130 bpm, and a
margin is enough; g) Lymphadenectomy is rarely indicated
blood pressure of 90/50 mmHg. Vigorous volemic resuscitation
because lymph node metastasis are rare.
was undertaken (crystalloid and three blood units) as well as
Considering that, in series including elective surgical
omeprazole. Hemoglobin: 4.7 g/dl. Upper gastrointestinal
procedures, complete gross resection is possible in approximately 85%
endoscopy showed great amount of bright red blood, distal to the
of patients with primary localized tumors. Negative microscopic
second portion of the duodenum, not amenable to endoscopic
margins are achieved in 70 to 95% of these completely resected cases.
evaluation. Due to hemodynamic instability the patient underwent
Although after a complete resection of a localized GIST, at least 50% of
laparotomy. An exophytic tumor at the Treitz level was found.
patients develop recurrence (1). The adequate follow up strategy is
The patient was submitted to a small bowel resection with end-to-
still unknown. Computed tomography scans of the abdomen and
end anastomosis.The shock was controlled and the post-operative
pelvis every 3 to 6 months according to the malignant potential of the
recovery was uneventful. Histopathologic study: 1.7X4.0 cm
tumor have been advocated. The interval can be extended after the
transmural nodule, with intra and extraluminal protrusion,
third year (1-3). The development of imatinib brought great advance
transmural involvement by fusocelular neoplasia with myxoid
in the treatment of the metastatic disease, with a response rate of
degeneration foci and ulceration.The findings are suggestive of
more than 50% and stabilization of the disease in more than 70% (4,
gastrointestinal stromal tumor (GIST).Immunohistochemical
5). Ongoing trials are evaluating the expanding use of imatinib as
panel: positive C-KIT. Six months after the surgical procedure the
neoadjuvant therapy as well as how long should it be used.
patient is doing well with no signs of recurrence.
Despite its rarity, GIST is the most common mesenquimal
tumor of the gastrointestinal tract. GISTs are probably originatedfrom the interstitial cells of Cajal, located in and around themyenteric plexus and thought to function as the intestinalperistalsis pacemaker. Previously misclassified as leiomyomas orleiomyosarcomas, its ultra structural features andimmunophenotypical markers (the most notable is KIT (CD 117) –with at least 95% staining positive) now distinct this entity (1). GIST has a slight male predominance, with a median age ofapproximately 60 years. GIST can occur anywhere along thegastrointestinal tract but most commonly arises in the stomach(65%) or small intestine (25%). Colon and rectum are the location of5 to 10% and another 5% are found in the esophagus. Uncommonly,GISTs can develop in the omentum, mesentery, or retroperitoneum. The clinical presentation varies widely. Approximately 70% ofpatients are symptomatic, 20% are asymptomatic, and 10% of thecases are detected at autopsy. Symptomatic tumors tend to be larger
and the symptoms are most commonly related to mass effect orbleeding. When GISTs erode into the lumen of the GI tract, they can
REFERENCES
induce significant hemorrhage or occult blood loss. Its rupture into
1. Gold JS, DeMatteo RP. Combined Surgical and Molecular
the peritoneum can be life-threatening. In the present case,
Therapy: The Gastrointestinal Stromal Tumor Model. Ann
guidelines for the assessment and management of gastrointestinal
bleeding apply, as well as the surgical resection principles.
2. DeMatteo RP, Brennan MF. Gastrointestinal Stromal Tumors.
Regarding the surgical management, even in the emergency setting,
In: Cameron JL. Current Surgical Therapy. 8 th ed. Philadelphia,
one should obey the following principles, according to the clinical
3. Blay JY, Bonvalot S, Casali P, et al. Consensus meeting for
a) Consider the surgery as the unique chance of cure; b) The
the management of gastrointestinal stromal tumors: Report of
abdominal exploration must be complete with particular attention
the GIST Consensus Conference of 20-21 March 2004, under
to the peritoneum and the liver (frequent sites of metastasis); c)
the auspices of ESMO. Ann Oncol. 2005;16:566 -578.
The surgical resection technique must be meticulous because
4. Joensuu H, Roberts PJ, Sarlomo-Rikala M, et al. Effect of the
GISTs are often friable, its capsule is easily torn with bleeding and
tyrosine kinase inhibitor STI571 in a patient with a metastaticgastrointestinal stromal tumor. N Engl J Med. 2001;344:1052-1056.
5. Demetri GD, Von Mehren M, Blanke CD, et al.: Efficacy and
** Chief of the Surgical Oncology - Hospital Nossa Senhora da Conceição,
safety of imatinib mesylate in advanced gastrointestinal
stromal tumors. N Engl J Med. 2002;347:472-480.
38 |Rev. Bras. Oncologia Clínica 2006 . Vol. 3 . N.º 7 (Jan/Abr) 37-38
Publikationen - Auswahl der letzten 5 Jahre Peginterferon alfa-2a/ribavirin for 48 or 72 weeks in hepatitis C genotypes 1 and 4 patients with slow virologic response. Ferenci P, Laferl H, Scherzer TM, Maieron A, Hofer H, Stauber R, Gschwantler M, Brunner H, Wenisch C, Bischof M, Strasser M, Datz C, Vogel W, Löschenberger K, Steindl-Munda P; Gastroenterology. 2010 Feb;138(2):503-12,
Ernährungsempfehlungen bei einem empfindlichen Magen-Darm-Trakt Bei einer Schonkost geht es um die Frage, welche Nahrungsmittel man besser nicht verzehrt, um das Verdauungssystem zu schonen. Dafür gibt es verschiedene allgemeine Empfehlungen; aber gerade bei einem empfindlichen Verdauungssystem müssen natürlich individuelle Nahrungsmittelunverträglichkeiten berücksichtigt werden: V
 Choque Hemorrágico comoManifestação Inicial de TumorEstromal Gastrointestinal
Mulher de 43 anos é admitida no serviço de emergência por
sangramento e aumentando a chance de recorrência. d) A simples
apresentar quadro de hemorragia digestiva (hematêmese e ente-
enucleação do tumor deve ser evitada. e) Ressecções segmentares
rorragia). Negava episódios prévios, bem como utilização crônica de
do estômago ou intestino devem ser realizadas a fim de se obterem
medicamentos. Previamente hígida. Ao exame: pálida, sudorética
margens microscópicas negativas. f) Margem macroscópica de 1 a
com freqüência cardíaca de 130 bpm, pressão arterial de 90/50
2 cm é suficiente. g) Linfadenectomia raramente é indicada, pois o
mmHg. Realizado ressuscitação volêmica vigorosa (cristalóide e
comprometimento linfonodal é incomum. Em séries que incluem
três unidades de concentrado de hemácias) e iniciado omeprazol.
Choque Hemorrágico comoManifestação Inicial de TumorEstromal Gastrointestinal
Mulher de 43 anos é admitida no serviço de emergência por
sangramento e aumentando a chance de recorrência. d) A simples
apresentar quadro de hemorragia digestiva (hematêmese e ente-
enucleação do tumor deve ser evitada. e) Ressecções segmentares
rorragia). Negava episódios prévios, bem como utilização crônica de
do estômago ou intestino devem ser realizadas a fim de se obterem
medicamentos. Previamente hígida. Ao exame: pálida, sudorética
margens microscópicas negativas. f) Margem macroscópica de 1 a
com freqüência cardíaca de 130 bpm, pressão arterial de 90/50
2 cm é suficiente. g) Linfadenectomia raramente é indicada, pois o
mmHg. Realizado ressuscitação volêmica vigorosa (cristalóide e
comprometimento linfonodal é incomum. Em séries que incluem
três unidades de concentrado de hemácias) e iniciado omeprazol.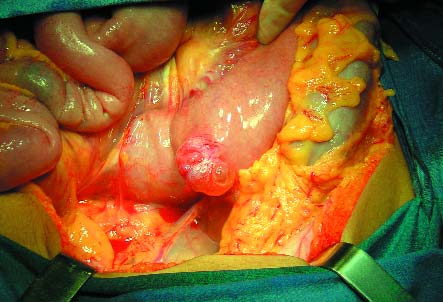 Hemorrhagic Shock as theInitial Presentation OfGastrointestinal Stromal Tumor
A 43 year-old-woman present to the emergency department
tumor rupture ensuing, increasing the recurrence rate; d) Simple
for sustaining gastrointestinal hemorrhage (hematemesis and
enucleation of the tumor should be avoided; e) Segmental
enterorrhagia). She denies previous episodes, as well as chronic
resection of the stomach or intestine should be performed to
medical usage. She was previously health. Physical examination
achieve negative microscopic margins; f) A 1 to 2 cm grossly
revealed: pallor, diaphoresis, a cardiac rate of 130 bpm, and a
margin is enough; g) Lymphadenectomy is rarely indicated
blood pressure of 90/50 mmHg. Vigorous volemic resuscitation
because lymph node metastasis are rare.
Hemorrhagic Shock as theInitial Presentation OfGastrointestinal Stromal Tumor
A 43 year-old-woman present to the emergency department
tumor rupture ensuing, increasing the recurrence rate; d) Simple
for sustaining gastrointestinal hemorrhage (hematemesis and
enucleation of the tumor should be avoided; e) Segmental
enterorrhagia). She denies previous episodes, as well as chronic
resection of the stomach or intestine should be performed to
medical usage. She was previously health. Physical examination
achieve negative microscopic margins; f) A 1 to 2 cm grossly
revealed: pallor, diaphoresis, a cardiac rate of 130 bpm, and a
margin is enough; g) Lymphadenectomy is rarely indicated
blood pressure of 90/50 mmHg. Vigorous volemic resuscitation
because lymph node metastasis are rare.