The Effects of Acid Perfusion of the Esophagus on Ventilation and Respiratory Sensation STEPHEN K. FIELD, JOHN A. EVANS, and LORNE M. PRICE
Department of Medicine, Foothills Hospital and University of Calgary, Calgary, Alberta, Canada
The relationship between gastroesophageal reflux (GER) and asthma remains controversial. Asthma symptoms worsen with GER, but are not consistently related to changes in lung function. The pur- pose of this study was to determine whether acid perfusion (AP) of the esophagus alters ventilation and causes respiratory symptoms. Nonasthmatic patients with normal lung function and esophageal disease (16 females and nine males, FEV 1 %predicted 9.6), underwent a Bernstein test after motility testing. Airflow, rib cage (Vrc), and abdominal (Vab) tidal volumes, esophageal (Pes) and gastric (Pga) pressure, and surface (Es) and esophageal (Edi) diaphragm electromyographic (EMG) signals were measured. Throat, swallowing, chest, and stomach discomfort and respiratory sensation were estimated with the Borg scale. Minute ventilation (VE) increased during AP and declined during recovery with saline perfusion of the esophagus (7.1 Ϯ 1.5 to 8.5 Ϯ 2.4 to 7.3 Ϯ 2.1 L/min; n ϭ 25; p ϭ 0.0002). Respiratory rate (RR) went from 13.6 Ϯ 2.6 to 15.8 Ϯ 3.4 to 15.3 Ϯ 3.1 breaths/min (n ϭ 25; p ϭ 0.0002) during AP. VE was greater in the Bernstein-positive patients during AP. Tidal volume (VT), Vrc, Vab, Pes, Pga, Es, and Edi did not change during AP. Chest discomfort (D) correlated with ventilation (VE ϭ 0.7 ϩ 0.8 D; r ϭ 0.67; p Ͻ 0.001) and respiratory effort sensation (B) (B ϭ 0.2 ϩ 0.4 VE; r ϭ 0.70; p Ͻ 0.001) during AP. AP did not inhibit diaphragm activity. Increased VE may explain the paradox of GER worsening respiratory symptoms without changing lung function. Field SK, Evans JA, Price LM. The effects of acid perfusion of the esophagus on ventilation and respi- ratory sensation. AM J RESPIR CRIT CARE MED 1998;157:1058–1062.
The prevalence of symptomatic gastroesophageal reflux
chial reactivity in asthmatic individuals (8). The importance of
(GER) is greater in asthmatic individuals than in other patient
GER in asthma severity has been questioned (9).
populations (1). Abnormal GER as reflected by ambulatory
The problem, then, is how best to explain the paradox of
pH monitoring criteria has been reported in over 80% of asth-
GER worsening asthma symptoms without a clinically impor-
matic individuals (2). Some asthma patients experience reflux-
tant change in lung function. Studies of respiratory sensation
associated respiratory symptoms (RARS), including dyspnea,
in other clinical conditions suggest that respiratory effort is its
wheezing, and cough (1, 3). These are often severe enough to
most important determinant (10). In some conditions, increased
warrant additional -agonist use (1, 3). Moreover, Irwin and
ventilation causes breathlessness in the absence of changes in
coworkers found that treating GER was the most important
lung function (11). The purpose of the present study was to
intervention for improving patients with difficult-to-control
determine whether AP could alter ventilation and respiratory
asthma who were referred to their clinic (4).
The strong association between GER and asthma suggests
a causal relationship between the two conditions. Most inves-
tigators have assumed that the relationship is due to GER
The subjects were nonasthmatic patients with normal lung function,
triggering bronchospasm. Proposed mechanisms include mi-
who were referred for motility testing as part of an investigation for
croaspiration or a vagally mediated esophagobronchial reflex
esophageal disease. They were willing to give informed written con-
(5). However, despite causing respiratory symptoms, both spon-
sent for their participation after the experimental protocol was ex-
taneous GER and acid perfusion (AP) of the esophagus have
plained to them. Instructions to the participants were as complete as
only minimal (6, 7) or no effect on either lung function or bron-
possible, but specific details about the Bernstein test were withheld toavoid biasing their responses. Because anxiety can contribute tobreathlessness, the patients were reassured and made as comfortableas possible prior to beginning the study. The study was approved bythe Conjoint Ethics Committee of the University of Calgary and Foot-
(Received in original form July 21, 1997 and in revised form October 27, 1997)
Presented in abstract form at the American Thoracic Society meeting, May 19,
Ventilation was measured with a No. 2 Fleisch pneumotachometer
(Gould Systems, Cleveland, OH) and a CD15 demodulator Ϯ 2 cm H2O
Supported by the Alberta Lung Association and Foothills Hospital Foundation.
pressure transducer (Validyne, Northridge, CA). Flow was integrated
Correspondence and requests for reprints should be addressed to Stephen K.
with a model 8815A Hewlett Packard integrator (Waltham, MA). The
Field, M.D., F.R.C.P.C., Clinical Professor of Medicine, University of Calgary Med-
patients breathed through a mouthpiece attached to the pneumot-
ical School, 1403 29th St. NW, Calgary, AB, T2N 2T9 Canada.
achometer, and wore a noseclip. Rib cage and abdominal anteroposte-
Am J Respir Crit Care Med Vol 157. pp 1058–1062, 1998
rior diameters were measured with pairs of magnetometers (GMG Sci-
Field, Evans, and Price: Effects of Acid Perfusion of the Esophagus
entific, Burlington, MA) placed at the levels of the middle of the body ofthe sternum and just above the umbilicus, respectively. The magnetome-ters were calibrated for volume by the isovolume method (12).
Gastric (Pga) and esophageal (Pes) pressures were measured with
a four-channel, water-filled catheter (Mui Scientific, Mississauga, On-tario, Canada). The most distal port was 1 cm from the end of thecatheter. The other three ports were 5 cm from each other, and 6, 11,and 16 cm from the distal end of the catheter, respectively. The proxi-mal ends of three of the channels were attached to pressure transduc-ers (Pressure/perfusion motility system TDS-4000; Sandhill, Littleston,CO). The most proximal channel was used to perfuse the esophaguswith either normal saline or 0.1 N HCl.
Diaphragm electromyographic (EMG) signals were measured
both with an esophageal catheter (13) and with surface electrodes. The surface electrodes were attached on the right side in the seventh,eighth, or ninth intercostal interspaces between the mid- and posterioraxillary lines. The signals were contaminated with expiratory muscleactivity with more anterior placement of the surface electrodes. Thesignals were amplified, bandpass-filtered between 100 and 2,000 Hz,rectified, and integrated, with a 100-ms time constant (1500 systemwith 15C01 EMG amplifiers; DISA, Denmark). All signals were re-corded on an eight-channel paper recorder (7758B recording system;
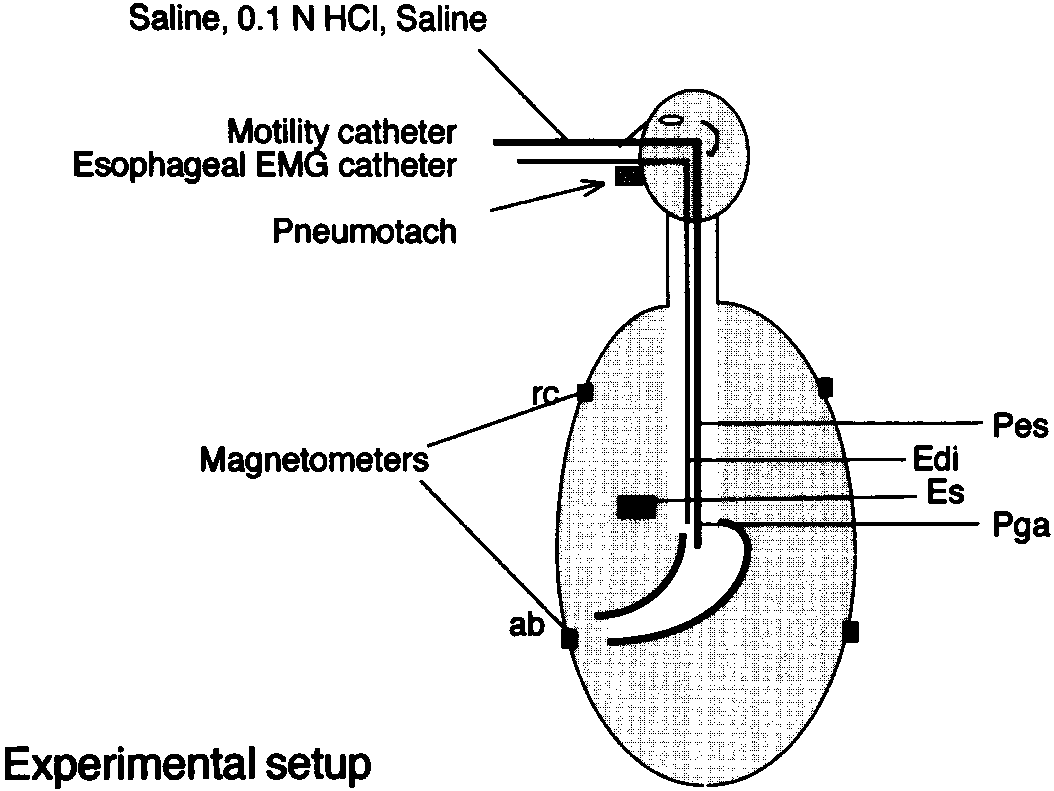
Figure 1. Experimental setup. Diagram shows leads and catheters
Hewlett-Packard Inc., Waltham, MA). The Borg scale was used as the
in place. Saline and 0.1 N HCl were infused into the lower esopha-
psychophysical measure of breathlessness (14). Patients also used it to
gus through the motility catheter. Two of the other ports in the
describe the severity of their throat, swallowing, chest, and stomach
motility catheter were used to measure esophageal and gastric
discomfort during each perfusion period.
pressure. Abbreviations: rc ϭ rib cage magnetometer coil; ab ϭabdominal magnetometer coil; Pes, Pga ϭ locations of ports in
ExperimentaI ProtocoI
motility catheter used for measurement of esophageal and gastric
The motility studies were done early in the morning, after an over-
pressures, respectively; Es ϭ surface EMG electrode; Edi ϭ esoph-
night fast. Patients receiving prokinetic agents, omeprazole, or H
receptor blockers were asked to discontinue these medications at leastone 1 wk before the study began. Antacids were withheld on the day
of the study. Gastrointestinal and respiratory functional inquires were
relationship between changes in symptoms and V E was explored with
conducted prior to the study. Patients were weighed, measured, and
linear regression analysis. Two-sample t tests were used to compare
changes from baseline in the BP versus the BN patients. Data were
The magnetometry discs and surface EMG electrodes were then
expressed as mean SD. The minimum level of statistical significance
attached. The four-channel pressure catheter was then inserted, fol-
lowed by the esophageal EMG catheter. These catheters were in-serted transnasally, with the aid of lubricant but without topical anes-
thetic. The patients were then placed in the supine position and
All but one of the 25 patients in the study were referred for
remained in that position through the motility and Bernstein tests
evaluation of suspected esophageal disease. Presenting symp-
(15). The experimental setup is shown in Figure 1.
The motility study took 30 to 45 min. Once it was completed, the
toms included dysphagia, atypical chest pain, poorly con-
pressure catheter was placed across the lower esophageal sphincter
trolled pyrosis despite intensive medical antireflux therapy, or
(LES), so that the distal port recorded gastric pressure and the third
motility testing was ordered as part of the preoperative evalu-
port (11 cm from the catheter tip) recorded Pes. The most proximal
ation for esophageal surgery. One patient was referred for
port of the pressure catheter was used to perfuse the esophagus with
evaluation of intractable chronic cough. This patient had nor-
normal saline or 0.1 N HCl at a rate of 5 ml/min. The esophageal
mal pulmonary function and methacholine challenge tests.
EMG catheter was then positioned to optimize the inspiratory dia-
The characteristics of the study patients are given in Table 1.
phragm EMG signal. This position was usually within 5 cm of the mid-
The BP and BN groups were similar with regard to age, gen-
point of the LES. The motility study allowed accurate determination
der ratio, and body mass index (BMI). Spirometry gave nor-
of the location of the LES. The signals were then recalibrated and the
To provide a stable baseline, the patients breathed through the
Respiratory Symptom and Discomfort Scores
mouthpiece attached to the pneumotachometer, with the noseclip inplace, for a minimum of 5 min before the beginning of the motility
Eleven of the Bernstein tests were negative and 14 were posi-
study. In sequence, saline, acid, and saline were perfused for 5-min pe-
tive. The numeric scores of throat, swallowing, chest, and
riods each. The patients were neither told when the infusions were be-gun nor which solution they were receiving. The signals were recordedcontinuously. At the end of each infusion period, the patients were
asked to rate their throat, swallowing, chest, and stomach discomfort,
ANTHROPOMETRIC DATA FOR THE 25 STUDY SUBJECTS
as well as respiratory sensation with the Borg scale. The motility nursequestioned the patients separately about their symptoms during acid
perfusion of the esophagus, and determined whether the Bernstein
test was positive (BP) or negative (BN) according to whether acid re-
produced their typical heartburn pain. Statistics
Two-way analysis of variance (ANOVA) was used to compare the re-
sults of different continuous variables in the three infusion periods. As
Definition of abbreviation: BMI ϭ body mass index.
a follow-up to the two-way ANOVA, Tukey’s studentized range test
was used to compare the different parameters between periods. The
No significant difference was seen between the groups for any variable.
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
RESPIRATORY SYMPTOM (BORG) AND THROAT, SWALLOWING, CHEST, AND STOMACH DISCOMFORT SCORES
1.3 Ϯ 1.7 0.8 Ϯ 1.0 1.0 Ϯ 1.3 0.9 Ϯ 1.1
1.4 Ϯ 1.4 1.4 Ϯ 1.4 1.3 Ϯ 1.4 1.1 Ϯ 1.2
0.6 Ϯ 0.8 3.0 Ϯ 2.3* 1.7 Ϯ 1.4 0.8 Ϯ 1.0 0.7 Ϯ 0.8 0.9 Ϯ 1.1
1.6 Ϯ 1.4 1.1 Ϯ 1.0 1.5 Ϯ 1.5 0.7 Ϯ 0.8
0.7 Ϯ 1.1 0.2 Ϯ 0.5 0.8 Ϯ 1.2 0.8 Ϯ 1.5
Definition of abbreviations: Saline 1 ϭ first saline perfusion period; Saline 2 ϭ second
* The change in chest discomfort (D) was greater in the Bernstein-positive than in the
Bernstein-negative patients (p Ͻ 0.05).
stomach discomfort ratings and respiratory symptoms areshown in Table 2. The changes in discomfort ratings duringacid perfusion (AP) were all greater in the BP group, but the
Figure 2. V E of individual patients during saline and acid perfusion
difference only reached statistical significance for chest dis-
periods. Patients are grouped according to whether they had a
comfort (D). The patients felt that throat discomfort was pri-
positive or negative Bernstein test result (see text). V E for the Bern-
marily related to the presence of the catheters. Most of the
stein-positive patients was 7.0 Ϯ 1.6, 9.4 Ϯ 2.6, and 7.8 Ϯ 2.5 L/
symptomatic patients described the other discomforts as pres-
min in the first saline perfusion, acid perfusion, and second perfu-
sure or burning sensations resembling their heartburn pains.
sion periods, respectively. The V E for the Bernstein-negative pa-
The average change in breathing sensation during AP was
tients was 7.2 Ϯ 1.5, 7.4 Ϯ 1.5, and 6.6 Ϯ 1.2 L/min in the first sa-
greater in the BP patients, but the difference was not statisti-
line perfusion, acid perfusion, and second saline perfusion periods,
cally significant (Table 2). Most of the symptomatic patients
described the sensation as an awareness of their breathingbeing greater but not unpleasant. The two patients whose ven-
tilation increased to the greatest extent described the un-
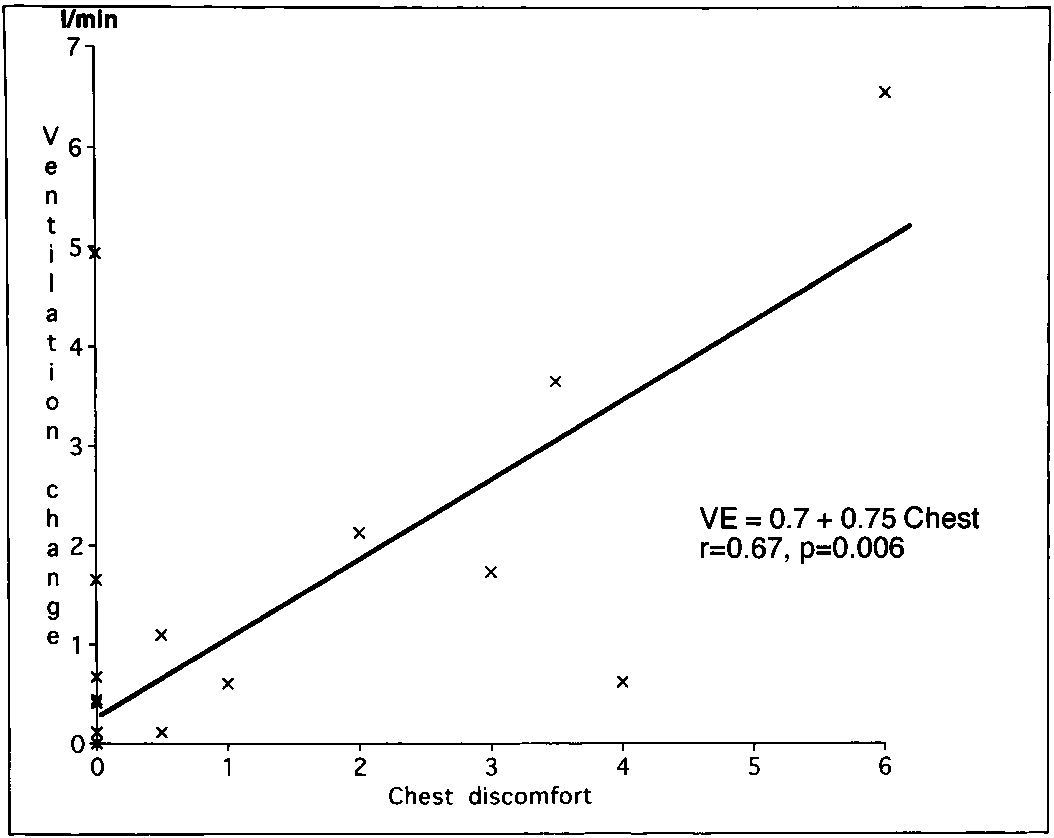
There was a linear correlation between the increase in VE
pleasant sensation of shortness of breath or an inability to get
and the change in chest discomfort (D) score during AP
(VE ϭ 0.7 ϩ 0.8 D; r ϭ 0.67; p Ͻ 0.01) (Figure 3). The in-creased swallowing discomfort also correlated with the change
Ventilation
in VE (VE ϭ 1.1 ϩ 0.8 swallowing discomfort; r ϭ 0.50; p Ͻ
The VE of the entire group was greater during AP than at
0.05). The change in VE and the increases in chest and swal-
baseline (Table 3). The increase in VE was due to an increase
lowing discomfort correlated with the change in respiratory
in respiratory rate (RR). Neither tidal volume (VT) nor its rib
sensation (B) (B ϭ 0.2 ϩ 0.4 VE; r ϭ 0.70; p Ͻ 0.001; B ϭ
cage (Vrc) or abdominal (Vab) components changed during
0.1 ϩ 0.4 D; r ϭ 0.62; p ϭ 0.01; B ϭ 0.3 ϩ 0.5 swallowing dis-
AP (Table 3). Comparison of the BP with the BN patients
comfort; r ϭ 0.55; p ϭ 0.03).
demonstrated that the change in VE was greater in the BP pa-tients (7.0 Ϯ 1.6 to 9.4 Ϯ 2.6 L/min, versus 7.2 Ϯ 1.5 to 7.4 Ϯ1.5 L/min, p ϭ 0.002) (Figure 2). VENTILATION, PRESSURE, AND EMG DATA Definition of abbreviations: VE ϭ minute ventilation; RR ϭ respiratory rate; Vrc ϭ rib
cage tidal volume; Vab ϭ abdominal tidal volume; rc/ab ϭ ratio of rib cage to abdom-inal tidal volumes; Pes ϭ tidal esophageal pressure swing; Pga ϭ tidal gastric pressureswing; Pes/Pga ϭ ratio of esophageal to gastric tidal pressure swing; Es ϭ surface elec-
tromyographic signal; Edi ϭ esophageal electromyographic signal. Figure 3. Relationship between the change in V E and change in
chest discomfort (D) rating during acid perfusion of the esophagus.
Field, Evans, and Price: Effects of Acid Perfusion of the Esophagus
Pressure and Electromyographic Signals
Undoubtedly, the mouthpiece and noseclip adversely af-
Tidal swings in Pes and gastric pressure (Pga) did not change
fected patient comfort and ventilation. Milic-Emili and cowork-
during AP (Table 3). Neither did the ratio of esophageal to
ers showed that wearing a noseclip and breathing through a
gastric tidal pressure swings (Pes/Pga). There was a correla-
mouthpiece, even one with a small dead space, increased E
tion between the product of Pes and RR and the change in
(20). However, we felt it important to accurately measure ven-
respiratory sensation (r ϭ 0.53, p Ͻ 0.01). Neither the surface
tilation in this study. The greater VE caused by the mouth-
(Es) nor the esophageal (Edi) electromyographic signal mag-
piece may have increased the patients’ breathlessness scores.
However, the effect should have been similar in the acid andsaline periods.
Some patients had hiatal hernias, which made placement
DISCUSSION
and maintenance of the esophageal catheters, especially the
To avoid the controversy surrounding the effects of GER on
airway tone in asthmatic individuals, nonasthmatic subjects
The subjects were patients referred for evaluation of sus-
with normal lung function were chosen for this study. The
pected esophageal disease, and had a high prevalence of esoph-
agitis. Patients with esophagitis may be more symptomatic dur-
ing AP than normal individuals. Their ventilatory response to
E was greater in the BP patients, and the severity
of chest discomfort correlated with the increase in V
chest discomfort might not accurately reflect that in normal or
though the literature on the subject is not extensive, several
reports have addressed the relationship between pain andventilation. Sarton and colleagues (16) found that pain in-
Effect of Gastroesophageal Reflux on Pulmonary Function
creased VE in normal volunteers. Both Bourke (17) and Borg-bjerg and associates (18) found that painful stimuli enhanced
Studies of the effects of GER on asthma present an interesting
paradox. Despite the strong association between the two con-
increased in response to pain during AP of the esophagus is
ditions, GER has not been shown to worsen lung function or
consistent with these findings (16–18).
bronchial reactivity consistently (8). Either GER affects only
The changes in breathing sensation correlated with the in-
some asthmatics (21), or its effects are minor and unlikely to
be clinically significant (7). The small reductions in peak expi-
E during AP. The BP patients reported an increase
in respiratory sensation even though the changes in V
ratory flow rate (PEFR) reported during AP can be explained
relatively small. Most of the BP patients described the respira-
by other mechanisms than a change in lung function or airway
tory sensation during AP as a greater awareness of breathing
tone (7, 22). The PEF maneuver is effort dependent, and chest
effort that was not unpleasant. Despite having normal lung
discomfort during AP may limit the ability of a patient to
function, two patients were breathless during AP. Adams and
make a maximal effort (23). This may account for some of the
conflicting reports on the effects of GER in the literature. De-
normal subjects breathless (19). Even though the magnitude
spite the inability to consistently demonstrate that spontane-
of the ventilation increase was consistent for each individual,
ous GER or AP increases airway tone, asthmatic individuals
they found a wide range between subjects. An increase of only
complain of RARS. Cough, dyspnea, wheezing, and -agonist
12 L/min caused breathlessness in some of their normal subjects.
use occur in asthmatic individuals in association with GER (1,
Two of the 14 BP patients in our study described the respira-
3). The present study demonstrates how GER may cause dys-
tory sensation during AP as breathlessness, and felt that it was
pnea without worsening airway obstruction. Increased ventila-
tion during episodes of GER may cause even more breathless-
proximately 6.5 L/min. This increase was proportionately sim-
ness in patients with airway obstruction. The correlation
ilar to that described by Adams and coworkers since our breath-
between the severity of GER and asthma symptoms reported
less subjects were relatively small women and most of their
by Goodall and colleagues (6) is consistent with our findings.
patients were average-sized males (19). Our subjects were na-
Two other groups have reported dyspnea caused by GER
ive patients, relatively obese, and were studied while supine.
in patients with normal lung function and bronchial reactivity.
Anxiety and the factors mentioned previously may have con-
Both Pratter and Depaso showed that GER was the cause of
tributed to their symptoms. Discomfort related to the esoph-
otherwise unexplained dyspnea in patients referred to their
ageal catheters and monitoring equipment was similar in the
clinics for evaluation (24, 25). Ambulatory pH monitoring con-
saline and AP periods, and should not have contributed to the
firmed the temporal association between GER and dyspnea
differences in respiratory sensation.
(25). Moreover, dyspnea resolved with successful antirefluxtherapy (25). Limitations of the Study
Ideally, pH would have been measured continuously to ensure
Diaphragm Function During AP of the Esophagus
that esophageal pH was neutral during the saline perfusion
The diaphragm contributes to maintenance of LES tone, and
periods and low during AP. Some subjects may have experi-
relaxation of the crural fibers facilitates the entry of a food bo-
enced spontaneous GER during the control saline period. In
lus into the stomach (26). Stimulation of mechanoreceptors by
some, VE and discomfort scores were higher during the sec-
esophageal distension causes reflex relaxation of the crural di-
ond saline period than during the first, suggesting the possibil-
aphragm (27). It also causes diaphragm inhibition in humans
ity of incomplete esophageal clearing of acid after AP. In oth-
(28). Acid has been reported to stimulate these esophageal
ers, VE was lower in the second saline period, possibly to
mechanoreceptors (29). Therefore, it is reasonable to specu-
compensate for the greater ventilation during AP. We decided
late that AP of the esophagus might cause diaphragm inhibi-
not to monitor pH, since it would have required a third probe,
tion and, in turn, breathlessness. However, neither the Edi nor
adding both to the patients’ discomfort and the time needed to
Es decreased during AP in the present study. Moreover, nei-
complete the study. Moreover, pH monitoring would have
ther Vrc/Vab nor Pes/Pga changed during AP, suggesting that
added substantially to the cost of the study.
clinically significant diaphragm inhibition did not occur.
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
Reflux as a Cause of Breathlessness in
tor. The Thorax, 2nd ed: Lung Biology in Health and Disease. Marcel
Other ClinicaI Conditions
11. Field, S. K., S. G. Bell, D. F. Cenaiko, and W. A. Whitelaw. 1991. Rela-
This study raises questions about the etiology of dyspnea in
tionship between respiratory effort and breathlessness in pregnancy.
other clinical conditions associated with GER. Although there
J. Appl. Physiol. 71:1897–1902.
is not as much data as with asthma, the reported prevalence of
12. Konno, K., and J. Mead. 1967. Measurement of the separate volume
GER and hiatal hernia in other respiratory conditions, including
changes of the rib cage and abdomen to ventilation during exercise. J.
pulmonary fibrosis and cystic fibrosis, is high (30, 31). GER may
contribute to breathlessness in these conditions. Patients with
13. Bellemare, F., and A. Grassino. 1982. Evaluation of human diaphragm
fatigue. J. Appl. Physiol. (Respir. Environ. Exerc. Physiol.) 53:1196–
heart disease take a variety of medications that are smooth-mus-
cle relaxants. By facilitating GER, these medications may con-
14. Borg, G. 1982. Psychophysical bases of perceived exertion. Med. Sci.
tribute to dyspnea in cardiac patients. Reflux-induced changes
in VE may be responsible for unexplained dyspnea in other-
15. Wu, W. C. 1990. Ancillary tests in the diagnosis of gastroesophageal re-
flux disease. Gastroenterol. Clin. North Am. 19:671–682.
In summary, AP of the esophagus increases V
16. Sarton, E., A. Dahan, L. Teppema, M. van den Eisen, E. Olofsen, A.
Berkenbosch, and J. van Kleef. 1996. Acute pain and central nervous
ratory sensation. The increase in VE correlates with the sever-
system arousal do not restore impaired hypoxic ventilatory response
ity of chest discomfort during AP. There was no evidence in
during sevoflurane sedation. Anesthesiology 85:295–303.
the present study that AP inhibits diaphragm function. Dis-
17. Bourke, D. L. 1993. Respiratory effects of regional anesthesia during
comfort-induced changes in VE offer a logical explanation for
acute pain. Regional Anesth. 18:361–365.
the paradox of GER causing asthma symptoms without chang-
18. Borgbjerg, F. M., K. Nielsen, and J. Franks. 1996. Experimental pain
ing lung function, and explain how GER may cause dyspnea in
stimulates respiration and attenuates morphine-induced respiratorydepression: a controlled study in human volunteers. Pain 64:123–128.
patients with normal lung function and bronchial reactivity
19. Adams, L., N. Chronos, R. Lane, and A. Guz. 1985. The measurement of
(24, 25). One would expect that GER and the associated in-
breathlessness induced in normal subjects: validity of two scaling tech-
crease in VE would have a greater effect in patients with respi-
niques. Clin. Sci. 69:7–16.
ratory disease. In asthmatic individuals dyspnea associated with
20. Askanazi, J., P. A. Silverberg, R. J. Foster, A. I. Hyman, J. Milic-Emili,
and J. M. Kinney. 1980. Effects of breathing apparatus on breathing
of worsening bronchospasm. Our results also explain the appar-
pattern. J. Appl. Physiol. (Respir. Environ. Exerc. Physiol.) 48:577–580.
21. Harding, S. M., J. E. Richter, M. R. Guzzo, C. A. Schan, R. W. Alex-
ent paradox that medical and surgical antireflux therapy im-
ander, and L. A. Bradley. 1996. Asthma and gastroesophageal reflux:
prove asthma symptoms and reduce medication requirements
acid suppressive therapy improves asthma outcome. Am. J. Med. 100:
without improving lung function or bronchial reactivity (32).
22. Schan, C. A., S. M. Harding, J. M. Haile, L. A. Bradley, and J. E. Rich-
Acknowledgment : The authors wish to thank Deb Erickson and Joyce
ter. 1994. Gastroesophageal reflux-induced bronchoconstriction: an
Haworth, motility nurse clinicians, for their skill, patience, help, and good
intraesophageal acid infusion study using state-of-the-art technology.
nature. They would also like to thank Drs. R. L. Cowie, G. T. Ford, K. Mac-
Cannell, J. Remmers, and W. A. Whitelaw for their insightful comments,
23. Miller, A. 1986. Spirometry and maximum expiratory flow-volume
and Dr. R. Brant and V. Shragg for their help with the statistical analysis.
curves. In A. Miller, editor. Pulmonary Function Tests in Clinical andOccupational Lung Disease. Grune & Stratton, Orlando, FL. 15–52.
24. Pratter, M. R., F. J. Curley, J. Dubois, and R. S. Irwin. 1989. Cause and
References
evaluation of chronic dyspnea in a pulmonary disease clinic. Arch. In-
1. Field, S. K., M. Underwood, R. Brant, and R. L. Cowie. 1996. Prevalence
of gastroesophageal reflux symptoms in asthma. Chest 109:316–322.
25. DePaso, W. J., R. H. Winterbauer, J. A. Lusk, D. F. Dreis, and S. C.
2. Sontag, S. J., S. O’Connel, S. Khandelwal, T. Miller, B. Nemschausky,
Springmeyer. 1991. Chronic dyspnea unexplained by history, chest
T. G. Schnell, and R. Serblosky. 1990. Most asthmatics have GER
roentgenogram, and spirometry: analysis of a seven-year experience.
with or without bronchodilator therapy. Gastroenterology 99:613–620.
3. Ekstrom, T., B. R. Lindgren, and L. Tibbling. 1989. Effects of ranitidine
26. Boyle, J. T., S. M. Altschuler, T. E. Nixon, D. N. Tuchman, A. I. Pack,
treatment on patients with asthma and a history of gastroesophageal
and S. Cohen. 1985. Role of the diaphragm in the genesis of the lower
reflux: a double blind crossover study. Thorax 44:19–23.
esophageal pressure in the cat. Gastroenterology 88:723–730.
4. Irwin, R. S., F. J. Curley, and C. L. French. 1993. Difficult-to-control
27. Monges, H., J. Salducci, and B. Naudy. 1978. Dissociation between the
asthma: contributing factors and outcome of a systematic manage-
electrical activity of the diaphragmic dome and crura muscular fibres
ment protocol. Chest 103:1662–1669.
during esophageal distension, vomiting and eructation. J. Physiol.
5. Castell, D. O., and P. F. Schnatz. 1995. Gastroesophageal reflux disease
and asthma: reflux or reflex? Chest 108:1186–1187.
28. Rimmer, K. P., W. A. Whitelaw, K. Graham, and S. K. Field. 1989.
6. Goodall, R. J. R., J. E. Earis, D. N. Cooper, A. Bernstein, and J. G. Tem-
Mechanisms of hypoxemia during panendoscopy. J. Clin. Gastroen-
ple. 1981. Relationship between asthma and gastroesophageal reflux.
29. Harding, R., and D. A. Titchen. 1975. Chemosensitive vagal endings in
7. Herve, P., A. Denjean, R. Jian, G. Simonneau, and P. Duroux. 1986. In-
the oesophagus of the cat. J. Physiol. (London) 247:52P–53P.
traesophageal perfusion of acid increases the bronchomotor response
30. Mays, E. E., J. J. Dubois, and G. B. Hamilton. 1976. Pulmonary fibrosis
to methacholine and isocapnic hyperventilation in asthmatic subjects.
associated with tracheobronchial aspiration: a study of the frequency
Am. Rev. Respir. Dis. 134:986–989.
of hiatal hernia and gastroesophageal reflux in interstitial pulmonary
8. Tan, W. C., R. J. Martin, R. Pandey, and R. D. Ballard. 1990. Effects of
fibrosis of obscure etiology. Chest 69:512–515.
spontaneous and simulated gastroesophageal reflux on sleeping asth-
31. Scott, R. B., E. V. O’Loughlin, and D. G. Gall. 1985. Gastroesophageal
matics. Am. Rev. Respir. Dis. 141:1394–1397.
reflux in patients with cystic fibrosis. J. Pediatr. 106:223–227.
9. Pack, A. I. 1990. Acid: a nocturnal bronchoconstrictor? Am. Rev. Respir.
32. Larrain, A., E. Carrasco, F. Galleguillos, R. Sepulveda, and C. E. Pope.
1991. Medical and surgical treatment of nonallergic asthma associated
10. Killian, K. J., and E. J. M. Campbell. 1995. Dyspnea. In C. Roussos, edi-
with gastroesophageal reflux. Chest 99:1330–1335.
Tetracycline MayoClinic.com Tetracycline (Class) (Oral Route, Parenteral Route) Description Tetracyclines are used to treat infections and to help control acne. Demeclocycline, doxycycline, and minocycline also may be used for other problems as determined by your doctor. Tetracyclines will not work for colds, flu, or other virus infections. Tetracyclines are available only with y
Monday, February 22, 1999 Bob Beck is a physicist, holding a Ph.D in physics from the University of Southern California. He also was previously a Professor at the University of California. He began his professional life as a photo-journalist and owned a photography studio in Hol ywood. He is a researcher and inventor who likes to improve upon other people's inventions. His version of the Brain
 Field, Evans, and Price: Effects of Acid Perfusion of the Esophagus
entific, Burlington, MA) placed at the levels of the middle of the body ofthe sternum and just above the umbilicus, respectively. The magnetome-ters were calibrated for volume by the isovolume method (12).
Field, Evans, and Price: Effects of Acid Perfusion of the Esophagus
entific, Burlington, MA) placed at the levels of the middle of the body ofthe sternum and just above the umbilicus, respectively. The magnetome-ters were calibrated for volume by the isovolume method (12).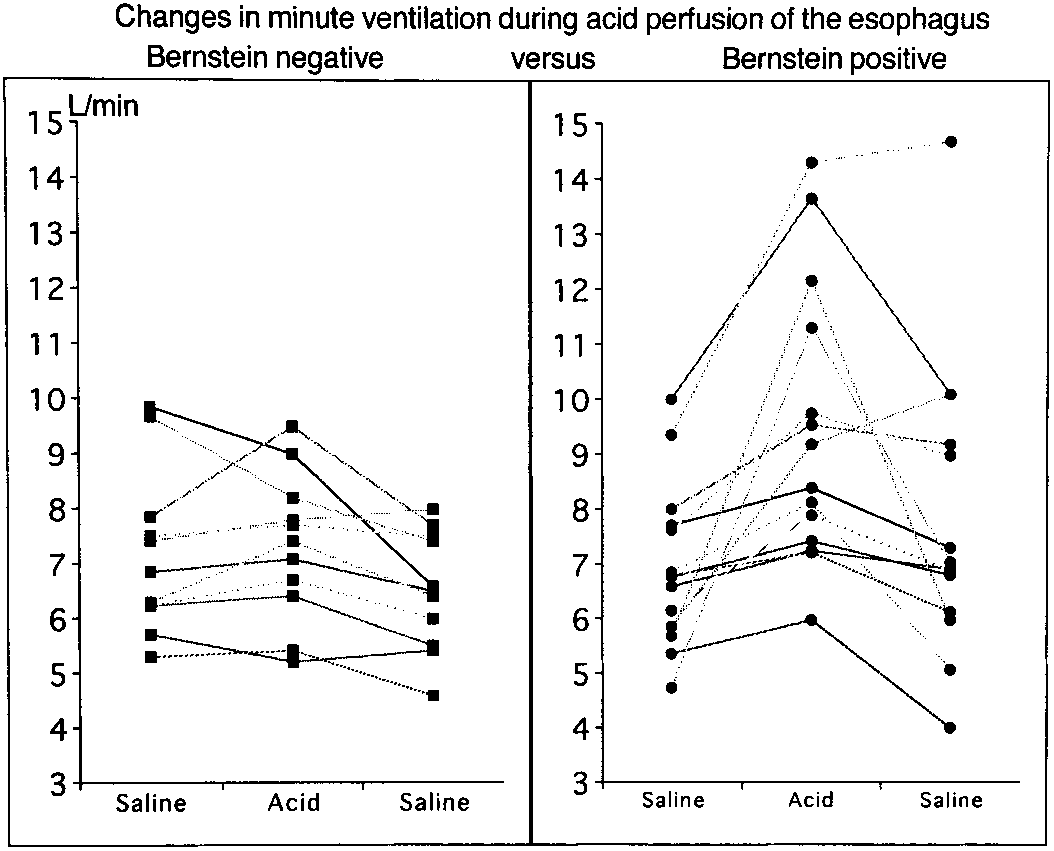
 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
RESPIRATORY SYMPTOM (BORG) AND THROAT, SWALLOWING,
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
RESPIRATORY SYMPTOM (BORG) AND THROAT, SWALLOWING,