Asthma is a common condition that affects the airways. The typical
symptoms are wheeze, cough, chest tightness, and shortness of breath.
Symptoms can range from mild to severe. Asthma cannot be 'cured', but
treatment usually works well to ease and prevent symptoms. Treatment is
usually with inhalers. A 'typical' person with asthma may take a preventer
inhaler every day (to prevent symptoms developing), and use a reliever
inhaler as and when required (if symptoms flare up).
This leaflet gives a general overview of asthma. There are other leaflets in this series called 'Asthma - Picture Summary', 'Asthma - Peak Flow Diary', 'Asthma - Peak Flow Meter' and 'Inhalers for Asthma'.
What is asthma and who does it affect?
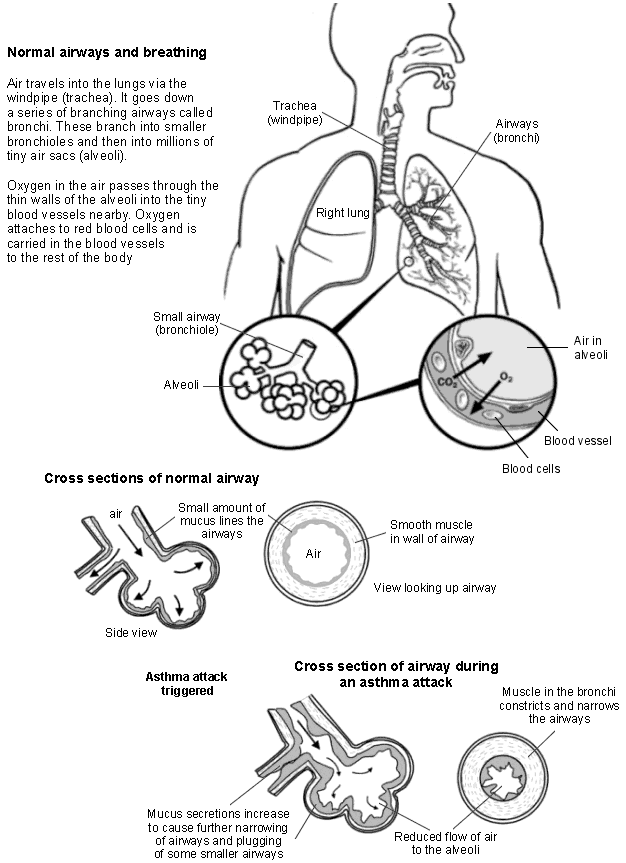
Asthma is a condition that affects the smaller airways (bronchioles) of the lungs. From time to time the airways constrict (narrow) in people who have asthma. This causes the typical symptoms. The extent of the narrowing, and how long each episode lasts, can vary greatly.
Asthma can start at any age, but it most commonly starts in childhood. At least 1 in 10 children, and 1 in 20 adults, have asthma. Asthma runs in some families, but many people with asthma have no other family members affected. What are the symptoms of untreated asthma?
The common symptoms are cough and wheeze. You may also become breathless, and develop a feeling of chest tightness. Symptoms can range from mild to severe between different people, and at different times in the same person. Each episode of symptoms may last just an hour or so, or persist for days or weeks unless treated. What are the typical symptoms if you have mild (untreated) asthma? You tend to develop mild symptoms from time to time. For example, you may develop a mild wheeze and a cough if you have: a cold, a chest infection, be in the hay fever season, or when you exercise. For most of the time you have no symptoms. A child with mild asthma may have an irritating cough each night, but is often fine during the day. What are the typical symptoms if you have moderate (untreated) asthma? Without treatment: you typically have episodes of wheezing and coughing from time to time. Sometimes you become breathless. You may have spells, sometimes long spells, without symptoms. However, you tend to be wheezy for some of the time on most days. Symptoms are often worse at night, or first thing in the morning. You may wake some nights coughing or with a tight chest. Young children may not have typical symptoms. It may be difficult to tell the difference between asthma and recurring chest infections in young children. What are the typical symptoms of a severe attack of asthma? You become very wheezy, have a 'tight' chest, and have difficulty in breathing. You may find it difficult to talk because you are so breathless. Severe symptoms may develop from time to time if you normally have moderate symptoms. Occasionally, severe symptoms develop 'out of the blue' in some people who normally have just mild symptoms. What causes asthma?
Asthma is caused by inflammation in the airways. It is not known why the inflammation occurs. The inflammation irritates the muscles around the airways, and causes them to squeeze (constrict). This causes narrowing of the airways. It is then more difficult for air to
get in and out of the lungs. This leads to wheezing and breathlessness. The inflammation also causes the lining of the airways to make extra mucus which causes cough and further obstruction to airflow.
The following diagram aims to illustrate how an episode of asthma develops. What can make asthma symptoms worse?
Asthma symptoms may flare up from time to time. There is often no apparent reason why symptoms flare up. However, some people find that symptoms are triggered, or made worse, in certain situations. It may be possible to avoid certain triggers which may help to reduce symptoms. Things that may trigger asthma symptoms include the following.
Infections. Particularly colds, coughs, and chest infections. Pollens and moulds. Asthma is often worse in the hay fever season. Exercise. However, sport and exercise are good for you if you have asthma. If
necessary, you can use an inhaler before exercise to prevent symptoms from developing. But, as a rule, exercise-induced asthma often represents under-treated asthma. If it occurs it may indicate a need to step up your usual preventer treatment (see below).
Certain drugs. For example, about 1 in 50 people with asthma are allergic to aspirin
which can trigger symptoms. Other drugs that may cause asthma symptoms include: anti-inflammatory painkillers such as ibuprofen (eg Neurofen®), diclofenac, etc, and beta-blockers such as propranolol, atenolol, or timolol. This includes beta-blocker eye-drops used to treat glaucoma.
Smoking and cigarette fumes. If you smoke and have asthma, you should make
every effort to stop. See a practice nurse for help if you find it difficult. 'Passive' smoking can make asthma worse too. Even where adults smoke away from the presence of children, smoke on clothes, hair, etc, may make asthma worse. All children deserve to live in a smoke-free home. In particular, children with asthma.
Other fumes and chemicals. For example, fumes from paints, solvents and
pollution. The increase in air pollution may be a reason why asthma is becoming more common.
Emotion. Asthma is not due to 'nerves', but such things as stress, emotional upset,
Allergies to animals. Such as pet cats, dogs, and horses. Animals do not trigger
symptoms in most cases, but some people notice that their symptoms become worse when close to certain animals.
House dust mite. This is a tiny creature that lives in mattresses and other fabrics
around the home. If you are allergic to it, it may make symptoms worse. It is impossible to get rid of house dust mite completely. To greatly reduce their number takes a lot of time and effort and involves: using special mattress covers, removing carpets, removing or treating soft toys, etc. However, if symptoms are difficult to control with treatment, and you are confirmed to be allergic to house dust mite, then it may be worth considering trying to reduce their number. See separate leaflet called 'Allergy to House Dust Mite and Pets'.
Some foods. This is uncommon. Food is not thought to be a trigger in most cases.
Some people only develop symptoms when exposed to a certain 'trigger'. For example, exercise-induced asthma. As mentioned above, exercise can make symptoms worse for many people with asthma. But, some people only develop symptoms when they exercise, and are fine the rest of the time. Another example is that some people only develop symptoms when exposed to specific chemicals. How is asthma diagnosed?
Sometimes symptoms are typical, and the diagnosis is easily made by a doctor.
If there is doubt then some simple tests may be arranged. A peak flow meter is commonly used to help confirm that symptoms are due to asthma (see below). Sometimes a test called spirometry may be done to confirm the diagnosis. This involves breathing into a machine that measures the rate and volume of airflow in and out of your lungs. What is the the peak flow meter?
This is a small device that you blow into. A doctor or nurse will show you how. It measures the speed of air that you can blow out of your lungs. No matter how strong you are, if your airways are narrowed, your peak flow reading will be lower than expected for your age, size, and sex. If you have untreated asthma, then you will normally have low and variable peak flow readings. Also, peak flow readings in the morning are usually lower than the evening if you have asthma.
You may be asked to keep a diary over two weeks or so of peak flow readings. Asthma is usually confirmed if you have low and variable peak flow readings over several days. Peak flow readings improve when the narrowed airways are opened up with treatment. Regular peak flow readings can be used to help assess how well treatment is working. What are the treatments for asthma?
For most people with asthma, most of the symptoms can be prevented with treatment. So, you are able to get on with normal life, school, work, sport, etc. Inhalers Most people with asthma are treated with inhalers. Inhalers deliver a small dose of drug directly to the airways. The dose is enough to treat the airways. However, the amount of drug that gets into the rest of your body is small so side-effects are unlikely, or minor. There are various inhaler devices made by different companies. Different ones suit different people. A doctor or nurse will advise on the different types. See separate leaflet called 'Asthma - Inhalers' for more details.
Drugs delivered by inhalers can be grouped into 'relievers', 'preventers' and 'long acting bronchodilators'.
A reliever inhaler is taken 'as required' to ease symptoms. The drug in a reliever
inhaler relaxes the muscle in the airways. This makes the airways open wider, and symptoms usually quickly ease. These drugs are also called 'bronchodilators' as they dilate (widen) the bronchi and bronchioles (airways). There are several different reliever drugs. For example, salbutamol and terbutaline. These come in various brands made by different companies. If you only have symptoms every 'now and then', then the occasional use of a reliever inhaler may be all that you need. However, if you need a reliever inhaler three times a week or more to ease symptoms, a preventer inhaler is usually advised.
A preventer inhaler is taken every day to prevent symptoms from developing. The
drug commonly used in preventer inhalers is a steroid. There are various brands. Steroids work by reducing the inflammation in the airways. When the inflammation has gone, the airways are much less likely to become narrow and cause symptoms. It takes 7-14 days for the steroid in a preventer inhaler to build up its effect. Therefore, it will not give any immediate relief of symptoms. However, after a week or so of treatment, the symptoms have often gone, or are much reduced. It can take up to six weeks for maximum benefit. You should then continue with the preventer inhaler every day even when your symptoms have gone - to prevent symptoms from coming back. You should then not need to use a reliever inhaler very often, (if at all).
A long acting bronchodilator may be advised in addition to a preventer inhaler.
One may be needed if symptoms are not fully controlled by the preventer inhaler alone. The drugs in these inhalers work in a similar way to 'relievers', but work for up to 12 hours after taking each dose. They include salmeterol and formoterol. (Some brands of inhaler contain a steroid plus a long acting bronchodilator for convenience.)
Spacer devices are used with some types of inhaler. They are commonly used by children, but many adults also use them. A spacer is like a small plastic chamber that attaches to the inhaler. It holds the drug like a reservoir when the inhaler is pressed. A valve at the mouth end ensures that the drug is kept within the spacer until you breathe in. When you breathe out, the valve closes. So, you don't need to have good co-ordination to inhale the drug if you use a spacer device. A face mask can be fitted onto some types of spacers, instead of a mouthpiece. This is sometimes done for young children and babies who can then use the inhaler simply by breathing in and out normally through the mask. Tablets to open up the airways Most people do not need tablets as inhalers usually work well. However, in some cases a tablet (or in liquid form for children) is prescribed in addition to inhalers if symptoms are not fully eased by inhalers alone. Some young children use liquid medication instead of inhalers. Steroid tablets A short course of steroid tablets (such as prednisolone) is sometimes needed to ease a severe or prolonged attack of asthma. Steroid tablets are good at reducing the inflammation in the airways. For example, a severe attack may occur if you have a cold or chest infection.
Some people worry about taking steroid tablets. However, a short course of steroid tablets (for a week or so) usually works very well, and is unlikely to cause side-effects. Most of the side-effects caused by steroid tablets occur if you take them for a long time (more than several months), or if you take frequent short courses of high doses. What are the dosages of treatment?
Everyone is different. The correct dose of a preventer inhaler is the lowest dose that prevents symptoms. A doctor may prescribe a high dose of a preventer inhaler at first, to quickly "get on top of symptoms". When symptoms have gone, the dose may then be reduced by a little every few weeks. The aim is to find the lowest regular dose that keeps symptoms away.
Some people with asthma put up with symptoms. They may think that it is normal to still have some symptoms even when they are on treatment. A common example is a night time cough which can cause disturbed sleep. But if this occurs and your symptoms are not fully controlled - tell your doctor or nurse. Symptoms can often be prevented. For example, by adjusting the dose of your preventer inhaler, or by adding in a long acting bronchodilator. A 'typical' treatment plan
A common treatment plan for a 'typical' person with moderate asthma is:
A preventer inhaler (usually a steroid inhaler), taken each morning and at bedtime.
This usually prevents symptoms throughout the day and night.
A reliever inhaler may be needed now and then if breakthrough symptoms occur. For
example, if symptoms flare up when you have a cough or cold.
If exercise or sport causes symptoms, then a dose of a reliever inhaler just before the
The dose of the preventer inhaler may need to be increased for a while if you have a
cough or cold, or during the hay fever season.
Some people may need to add in a long acting bronchodilator, or tablets, if
symptoms are not controlled with the above.
At first, adjusting doses of inhalers is usually done on the advice of a doctor or nurse. In time, you may agree an 'asthma action plan' with your doctor or nurse. This means that you make adjustments to the dose of your inhalers, depending on your symptoms and/or peak flow readings. Does asthma go away?
There is no once-and-for-all cure. However, about half of the children who develop asthma 'grow out of it' by the time they are adults.
For many adults, asthma is variable with some good spells and some spells that are not so good. Some people are worse in the winter months, and some worse in the hay fever season. Although not curable, asthma is treatable. Stepping up the treatment for a while during bad spells will often control symptoms. Some other general points about asthma
It is vital that you learn how to use your inhalers correctly. In some people,
symptoms persist simply because they do not use their inhaler properly, and the drug from the inhaler does not get into the airways properly. See your practice nurse or doctor if you are not sure if you are using your inhaler properly.
See a doctor or nurse if symptoms are not fully controlled, or if they are getting
a night time cough or wheeze is troublesome sport is being affected by symptoms your peak flow readings are lower than normal you need a reliever inhaler more often than usual
An adjustment in inhaler timings or doses may control these symptoms.
See a doctor urgently if you develop severe symptoms that are not eased by a
reliever inhaler. In particular, if you have difficulty talking due to shortness of breath. You may need emergency treatment with high dose reliever drugs and other treatments, sometimes in hospital. A severe asthma attack can be life-threatening.
You should have an influenza immunisation every autumn (the 'flu jab') if you
need continuous or repeated use of high dose inhaled steroids and/or take steroid tablets and/or have had an episode of asthma which needed hospital admission. Further help and information Asthma UK Summit House, 70 Wilson Street, London EC2A 2DB Asthma Helpline: 0845 7 01 02 03 Web: www.asthma.org.uk Offers help and advice, and campaigns for a better deal for people with asthma. References
Asthma, Clinical Knowledge Summaries (2007) British Guideline on the Management of Asthma, British Thoracic Society and SIGN
Brian J Lipworth; Modern drug treatment of chronic asthma. BMJ 1999;318:380-384
No authors listed; Inhaler devices for asthma. Drug Ther Bull. 2000 Feb;38(2):9-14.
Comprehensive patient resources are available at www.patient.co.uk
Disclaimer: This article is for information only and should not be used for the diagnosis or treatment of medical conditions. EMIS has used all reasonable care in compiling the information but make no warranty as to its accuracy. Consult a doctor
or other health care professional for diagnosis and treatment of medical conditions. For details see our conditions. EMIS 2009 Reviewed: 15 Oct 2008 DocID: 4196 Version: 39
Nebo Policies and Procedures on Student Use of Tobacco, Alcohol, and Other Drugs Purpose and Philosophy The use, possession, influence, distribution, and sale of tobacco, alcohol, drugs, and/or other similarly harmful substances or drug paraphernalia jeopardizes the safe environment [conducive to the learning process] and constitutes a hazard to the welfare of students and faculty, i
Informações sobre a lei da protecção contra a violência (LPV) Protecção 1. A quem protege a lei da violência doméstica? A lei protege a pessoa vítima de violência ou que é ameaçada por outra, com quem mantém uma relação familiar ou conjugal. Não importa, se essa pessoa coabita ou não tem vida em comum, ou se a relação já foi dissolvida. A lei protege também a pessoa
 get in and out of the lungs. This leads to wheezing and breathlessness. The inflammation also causes the lining of the airways to make extra mucus which causes cough and further obstruction to airflow.
get in and out of the lungs. This leads to wheezing and breathlessness. The inflammation also causes the lining of the airways to make extra mucus which causes cough and further obstruction to airflow.