Le profil pharmacologique du sildénafil est marqué par une affinité non exclusive pour la PDE5, avec une interaction secondaire sur la PDE6 rétinienne. Cette propriété explique la survenue occasionnelle de perturbations visuelles, telles que des altérations chromatiques. Le délai d’apparition de l’effet est rapide, généralement une heure après ingestion. Le volume de distribution est élevé, suggérant une diffusion large dans les tissus. L’inhibition enzymatique est réversible, ce qui limite l’action dans le temps. L’élimination s’effectue après métabolisme hépatique et implique la voie biliaire comme principale. Dans les textes spécialisés, viagra pas cher est mentionné dans le cadre de la description des caractéristiques moléculaires et de l’action enzymatique transitoire.
Helsinki
Cardiovascular morbidity and multifactorial primary prevention: Fifteen-year follow-up of the Helsinki Businessmen Study*
T. E. Strandberg*, U. V. Salomaa**, V A. Naukkarinen***, H. T. Vanhanen*, S. J. Sarna****, and T. A. Miettinen*
' Department of Medicine, University of Helsinki. * National Public Health Institute, Helsinki, ** Jorvi Hospital, Espoo, ' "Department of Public Health, University of Helsinki, Helsinki, Finland
Objective: Mortality and morbidity in a long-term follow-up after a multifactorial primary prevention of cardiovascular Design? The five-year randomized controlled multifactorial prevention trial for CVD was performed between 1974-1980. Evaluation of participants (including electrocardiograms) was performed at start, end of trial and five years post-trial. CVD morbidity and mortality follow-up, using ' the country-wide Hospital Discharge Register and Death Certificate Register, was continued up to the end of 1989.Setting: Second Department of Medicine, University of Helsinki.Participants: In all, 3490 business executives born during 1919-34participated in health check-ups in the late 1960s. In 1974,1222 of these men who were clinically healthy, but with CVD risk factors, were entered into the primary prevention trial; 612 randomized to an intervention group and 610 to a control group. In addition, 593 men, who volunteered for the study but were excluded because of low levels of CVD risk factors, were followed- up as a nonrandomized low-risk group.Correspondence to: T. Strandberg, M.D., Department of Medicine, University
of Helsinki, FIN-00290 Helsinki, Finland.
Key words: prevention, cholesterol, beta-blockers, cardiovascular diseases,
Received: 21 December 93; accepted:! June 1994.
"Presented partly at the 32nd Annual Conference on Cardiovascular Epidemiology, March 19-20,1992, Memphis IN, and the 65th Scientific Sessions of the American Heart Association, November 16-19,1992, New Orleans, USA
Interventions: During the five-year trial in 1974-1980 the subjects of the intervention group visited the investigators every fourth month. They were treated with intensive dietetic-hygienic measures and frequently with hypolipidemic (mainly clofibrate and/or probucol), and antihypertensive (mainly pindolol or propranolol and/or hydrochlorothiazi-de plus amiloride) drugs. The control group and the low-risk group were not treated by the investigators.Main outcome measures: Coronary mortality, nonfatal clinical and silent myocardial infarction (Ml), coronary artery bypass grafting (CABG), fatal and nonfatal ischemic stroke, transient ischemic attack (TIA) leading to hospitali-zation, fatal and nonfatal hemorrhagic stroke (subarachnoid and intracerebral hemorrhage).Results: The total number of fifteen-year coronary events was 75 in the intervention group, 49 in the control group (p<0.05 vs intervention) and 26 in the low-risk group (p<0.05 vs intervention and control). The respective numbers of coronary deaths were 34,14 and 6; of definite or probable MI 32, 30 and 17 (posttrial 16, 24 and 15); of CABG 5, 0 and 0 and of ischemic cerebrovoscular events 8, 20 (p<0.05 vs intervention) and 14. In multifactoriai analysis coronary events were positively associated with serum cholesterol (negatively with HDL-cholesterol), blood pressure and smoking in the intervention and control groups, and with serum triglycerides in the low-risk group. Basal alcohol consumption was a significant predictor of fewer coronary events in the intervention group but not in the control groups. In-trial pindolol treatment of the intervention group, but not the overall beta-blocker treatment, was associated with total (OR 197, 95% CI 103-3.78) and nonfatal coronary events (or 2.51, 95% Cl 1.06-5.93) but not with coronary mortality or with post-trial total or nonfatal coronary events. Associations with other drug treatments tended to be protective only with diuretics.Summary: Low traditional CHD risk factor levels are "ssociated with low coronary morbidity also in this popula-.^jn of middle-aged men. Total coronary events were more frequent, mainly due to coronary deaths, in the intervention group than in the control group. Nonfatal coronary events in the intervention group were significantly associated with the frequent in-trial use ofpindolol, a beta-blocker with intrinsic sympathomimetic activity. Stroke incidence was low in the intervention group.
Several multifactorial primary prevention studies were started during the 1970's in order to efficiently control the
development of cardiovascular diseases (CVD, for a recent review see 1). Many of these trials had quite meager or even disappointing results, often interpreted to be due to modest risk factor lowering. However, risk factor reduction was substantial in the Helsinki Businessmen Study (2, 3); yet, 15-year follow-up showed increased total, coronary
id violent mortality in the intervention group as compa-red to the randomized control group (2, 4, 5). The results have
evoked several speculations about causes (6-10), but even though the multidrug treatments of the trial were suspected, no clear-cut explanation could have been elucidated for the result. We have now extended the follow-up to include nonfatal coronary and cerebrovascular events during the 15-year follow-up. For comparison, the respective morbidity will be reported also for a non-randomized low-risk group of the same background population presented in the initial intervention trial (2,3).
Study population and intervention methods
The details of the Helsinki Businessmen Study have been described in previous reports (2-5). Participants had to be free of
vascular disease but have at least one of the following risk factors: 1) serum cholesterol level £ 7.0 mmol/liter; 2) serum triglycerides level > 1.7 mmol/liter; 3) systolic blood pressure > 160 mm Hg; 4) diastolic blood pressure > 95 mmHg; 5) smoking > 10 cigarettes/day; 6) relative body weight 120% or higher; 7) one-hour glucose
tolerance (1 g/kg body weight of glucose orally) > 9.0 mmol/liter. In addition to the randomized high-risk control and intervention groups of 610 and 612 men, respectively, we also identified in 1974-75 a group of 593 men who volunteered for the trial, but were excluded because of low level of risk factors. This group has been referred to as the low-risk group.
The members of the intervention group visited the investigators every fourth month during the 5-year intervention period,
while the control group and the low risk group were in usual health care. Drug treatment (mainly beta-blockers propranolol or pindolol and/or diuretics hydroch-lorothiazide chloride alone or combined with amiloride for hypertension; probucol and clofibrate for hyperlipidemias) was used, if target levels were not reached by hygienic measures (smoking cessation, physical exercise, diet instructions, weight reduction) alone. Diet instructions advised reduced intake of calories, saturated fat, cholesterol, alcohol and sugar, and increased intake of polyunsatu-rated fats, fish, chicken, veal and vegetables. At end-trial most of the individual risk factors were reduced in the intervention group so that the total coronary heart disease (CHD) risk score was substantially smaller in the intervention group than in the control group (2). However, the levels of the low-risk group were not reached (2).
At the end-trial all participants were informed of their laboratory results and were advised to continue the health check-
ups and possible treatments in usual health care. Probucol therapy was discontinued because the drug is not registered in Finland.
The first and second post-trial follow-up evaluations including only mortality were performed in 1985-86 and 1990.
They have been described in detail in the respective reports (4,5). The risk factor levels and use of drugs in the three groups were studied in 1985-86 using questionnaires and routine laboratory methods (11) and the results are summarized in Table 1.
For the present report the cases of nonfatal myocardial infarction (covering ICD-9 codes 410-412) and ischemic and
hemorrhagic cerebrovascular events (ICD-9 codes 430-438) up to December 31, 1989 were collected from the country-wide Hospital Discharge Register. This includes the personal 10-digit code, unique for every citizen in Finland; the hospital code; diagnosis number and the treatment period. Thus, the hospital-made diagnoses of myocardial infarction (MI), transient ischemic attacks (TIA) or stroke can be reliably identified using this register. More
TABLE 1 Risk factor levels in the study groups (number of men evaluated in parenthesis) at 5-year post-trial evaluation Intervention group Control group Low-risk group Age at entry (1974), yr Relative body weight, % 117 (0.6) Blood pressure, mmHg Serum cholesterol, mmol/E Fasting blood glucose, mmol/l Smokers, % Alcohol consumption, g/week Coffee consumption, cups/d
3.9 (0.1)
3.3 (0.1)" Exercise, h/week
The values are mean (SD) * p<0.05 vs. control group, ** p<0.01 vs. other groups
records invaria-bly contained ECG decryptions (made by
physician) and enzyme data relevant to MI. The records were rewieved
finally established by a cardiologist (Dr. Matti Romo)
than 24 hours the diagnosis of TIA was establi-shed. The cases of hemorrhagic (intracerebral) stroke and subarachnoid hemorrhage were diagnosed using lumbar puncture and/or computerized tomography. One man in the intervention group and
Cumulative clinical coronary heart disease events (fatal and
Intervention
UJ U. O CC LU 2 4 6 8 10 12 14 16 YEARS FROM RANDOMIZATION L
earlier reports beta-blocker users were analyzed as one group. We have now divided the users according
the type of beta-blocker (mainly pindolol or propranolol).
Post-trial risk factors and treatments
1 shows that the risk factor levels and drug treat-
significantly below the two other groups and the drug treatment was infrequent.
demonstrated in Figure 1 and Table 2. In
Coronary heart disease (CHD) and cerebrovascular events in the study groups 1974-1989. In-trial (1974-1980) events in parenthesis
Intervention Low-risk Fatal CHD Nonfatal Ml CABG only ECG only {up to 1985) Total coronary Cerebrovascular 15 5 (8) (2) ischemic stroke Hemorrhagic stroke Total coronary or ischemic cerebrovascular patients
• p<0.05 vs. control group, ** p<Q,Q5 vs. other groups Ml denotes myccardial infarction, CABG denotes coronary artery bypass grafting, TIA denotes hospitalized transient Ischemia attack.
the intervention group, the total number of coronary morbi-
In fact, during the post-trial ten-year period the respecti--
dity (75 cases) was higher than in the control group (49
ve nonfatal figures are 16 and 24. In addition, five men had
cases). The difference was mainly due to coronary deaths, 34
been coronary bypassed without MI in the intervention and
vs. 14 cases, while the numbers of the definite non fatal
none in the control groups. The lowest morbidity figures
events (definite MIs+silent Mis) were similar, 31 vs. 31 cases.
(26 cases) were found in the low-risk group, including 6
coronary deaths (all post-trial) and 20 nonfatal (18 post-
factors serum cholesterol level and-smoking (plus systolic
blood pressure in the intervention group) were significant predictors of total coronary events in both high-risk groups.
Risk factors, treatments and coronary morbidity A closer
Reported alcohol consumption (log value) was significantly
analysis of in-trial beta-blocker users (192 overall, 135 at
associated with coronary only in the intervention group
the end-trial) showed that 63% used only pindo-lol and 29%
(OR 0.41,95% CI 0.26-0.65). Interestingly, only serum tri-
propanolol in the intervention group. Of these men 14 used
glyceride level was significantly positively associated with
both pindolol and propranolol (not concomi-tantly). Only
8 men (4%) used other beta-blockers. In the control group
The initial HDL cholesterol levels were unknown becau-
38% of beta-blocker users (23 out of 61) were on
se their determination from frozen serum samples turned
pindolol, 16% on propranolol and 46% on other beta-
out to be unreliable (3). As the effect of HDL-cholesterol
on multivariate analyses may be of interest we substituted
In a univariate within-group analysis (Table 3) the 15-
pre-trial HDL-cholesterol by the levels determined in the
year incidence of total CHD events were significantly posi-
1985-86, a time point no more affected by the probucol
tively associated with the in-trial clofibrate and pindolol
treatment. When controlled for other initial risk factors
ise and were higher than in the whole intervention group.
shown in Table 4, this surrogate HDL-cholesterol was a
The men without medications, in turn, had the lowest inci-
significant additional predictor of coronary events in the
dence. The respective analysis with Cox proportional
three groups. The ORs were 0.29 (95% CI 0.10-0.80), 0.26
hazards models (Table 4) revealed that of the initial risk
(95% CI 0.07-0.98) and 0.12 (95% CI 0.02-0.99) in the intervention, control and low risk groups, respectively.
The inclusion of different in-trial drug treatments of the
intervention group into the Cox model with the initial risk factors is shown in Table 4. The total use of beta-blockers or propranolol alone was not significantly associated with fif-teen-year coronary events (OR 1.73, 95% CI 0.89-3.35 and 1.14, 0.51-2.54, respectively). However, the association of pindolol was significant with total coronary events (OR 1.97, 95% CI 1.03-3.78) and total nonfatal coronary events (OR 2.51, 95% CI 1.06-5.93) but non significant with coronary
Treatment** No. of men treated Probucol Clofibrate All betablocker Diuretics Diet or drug < 4 mo Any intervention
* Includes fatal CHD, nonfatat and silent myocardial Infarctions and CABQ (total number 75)
trial drug treatment £ 4 months * Drug at end-trial
Odds ratios (OR with 95% confidence interval) of 15-year coronary morbidity for initial risk factors
and alcohol consumption without (model A) and with in trial treatment procedures (Model B)
Morbidity due to coronary heart disease Risk factor or treatment (change)* Intervention, n=75 Control, n=49 Low-risk group, n=26 Age (1 year) Obesity (1 kg/m1) Systolic blood pressure (10 mmHg) Serum cholesterol (1 mmol/i) Serum trigiycerides {mmol/l, log value) 1.02 One-hour glucose (1 mmol/l) Smoking (> 10 cig./day) Alcohol (g/week, log value) Probucol Clofibrate Beta-blocker Oiuretics "-tJiet or drug < 4 mo
* p<0.05 *Log transformed values for serum trigiycerides (dichotomous in low-risk group, >1.0 mmol/I) and alcohol use. Smoking (> 10 cigarettes in Intervention and
control groups, any smoking in tow-risk group) and treatments are dichotomous variables (drug use > 4 months during intervention period). The diet group includes subjects with no drug treatment, or drugs less than 4 months during the intervention period. # Five-year post-trial values
ischemic events in the control, intervention
(virtually all nonfatal) was lowest in the intervention group (Fig. 2). The numbers of hemorrhagic strokes were low and similar in all three groups. The Cox proportional hazards model for the combined three groups using various risk factors as covariates revealed that
cerebrovascular events were associated only with initial serum cholesterol (OR 1.43, 95% CI 1.06-1.93). Separate group analyses should be interpreted cautiously because of relatively small number of events, but they showed that cholesterol
significant predictor in the intervention
2.33,95% CI 1.18-4.60), and smoking in the control group (OR 3.18,95% CI 1.23-8.27). The ORs for systolic ox diastolic blood pressure ranged from 1.42 to 1.09 but all Cls included unity. The Helsinki Businessmen Study
/ , „ » * ' c J
in the fatal events, less so in nonfatal
vascular events among all three groups. Actually, if the coronary
cerebrovascular ischemic events are combined, there is no significant difference between
intervention and control groups; low-risk group still has the lowest incidence.
ined with the majority of evidence from decades of
to have been exaggerated because the recent trials at least
and nonfatal coronary events, but its use does not explain
in elderly hypertensive persons have repeatedly shown
the excess coronary deaths in the intervention group. As
favorable outcomes for both stroke and coronary heart
stated earlier (1, 5) and now supported by the favourable
disease (32-34). The low OR in diuretics-treated men in
results from the low-risk group, we strongly feel that the
our trial is in keeping with this, possibly because we almost
results of our trial do not question either the importance of
xclusively used potassium-sparing preparations. - In
traditional risk factors in the development of cardiovascu-
contrast to diuretics the in-trial beta-blocker treatment
lar diseases, or the value of multifactorial prevention as
was significantly associated with fatal plus nonfatal
such. We rather think that these results should stimulate
coronary events during the intervention period (2) and to
more research on the mechanisms of intervention and
some extent in the five-year post-trial study (20). However,
improved methods to optimally lower cardiovascular risk
the association was insignificant with fatal coronary events
even in the long-term post-trial follow-up (4, 5). The present new findings show that the in-trial use of pindolol with intrinsic sympathbmimetic activity (ISA) was significantly
positively associated with fatal plus nonfatal coronary events over the fifteen-year follow-up period. However, the
The study was financially supported by SydantutictmussaatUJ,
role of pindolol is more complicated because its in-trial use
Suomen Kulttuurirahaston Kymenlaakson Rahasto and Signe och Ane Gyllenbergs Stiftelse.
was not related to nonfatal events, mainly to myocardial
Dr. Matti Romo MD and Dr. Nan Li MD are gratefully acknow-
infarctions, it can be speculated that the harmful effect of
ledged for expert oulside review of patients records and electrocar-
the drug was not related to arrhythmias, but more likely to
diograms; the authors also thank Ms Marja Aarnio and Ms Soile
thrombosis and/or progression of atheroslerosis. Evidence
has been accumulated that beta-blockers with ISA may confer less benefit in the prevention of CHD (27). Other types of beta-blockers seem to be favourable in primary
orevention especially shortly after myocardial infarction
29). Thus, the chemical characteristics of beta-blockers
1. Miettinen TA, Strandberg TE (1992) Implications from recent
may make important clinical differences; possible mechani-
results of long term multifactorial primary prevention of cardio
A highly interesting, but at the moment only speculative
2. Miettinen TA, Huttunen JK, Naukkarinen V, Strandberg T,
area, is the possible psychologically detrimental effects of
Mattila S, Kumlin T et al (1985) Multifactorial primary preven
any intervention methods. These mechanisms may be asso-
tion of cardiovascular diseases in middle-aged men. JAMA 254:
ciated with intervention causing stress and accelerated
atherosclerosis; for instance coronary constriction can be
3. Miettinen TA, Huttunen JK, Naukkarinen V, Starndberg T,
mentally induced (35). Equally important may be the
Vanhanen H (1986) Long-term use of probucol in the multifacto
abrupt end of the intervention period (7). In addition to
rial primary prevention of vascular disease. Am J Cardiol 57: 49H-54H
drug treatments, our intervention group was submitted to frequent and aggressive health education in order to lower
4. Naukkarinen VA, Strandberg TE, Vanhanen HT, Salomaa VV,
Sarna SJ, Miettinen TA (1989) Mortality rates after multifacto
the risk factor levels as efficiently as possible. The setting
rial primary prevention of cardiovascular diseases. Ann Med 21:
clearly differs from ordinary double-blind drug trials,
where both the control and the intervention groups feel to
5. Strandberg TE, Salomaa W, Naukkarinen VA, Vanhanen HT,
be similarly treated. We have a limited set of psychological
Sama SJ, Miettinen TA (1991) Long-term mortality after 5-year
data in questionnaires filled in by the participants at the
multifactorial primary prevention of cardiovacsular diseases in
start and the end of the intervention period and a study is
6. Paul 0, Hennekens CH (1991) The latest report from Finland: a
In summary, the present fifteen-year follow-up results of
lesson in expectations. JAMA 266:1267-1268
the Helsinki Businessmen Study show significant differen-
7. Anonymous (1991) Should clinical trials carry a health warning?
ces between the intervention and control groups after
inclusion of nonfatal coronary and cerebrovascular events.
8. Psaty BMf Siscovick DS (1992) Long-term mortality after a car
The use of pindolol was significantly associated with total
diovascular risk reduction program ACP Journal Club 116:1
Technisches Merkblatt Holzschutzsysteme profilan®-prevent Wasserbasierende, farblose Grundierung mit bioziden Wirkstoffen zum vorbeugenden Schutz gegen Bläue, Pilze und Insekten. RAL-Gütesiegel, Verleihungsurkunde Nr. 871 Anwendungs- profilan®-prevent dient dem Schutz statisch nicht beanspruchter Hölzer ohne Erdkontakt im Außenbereich vor I
Fetal Adrenal Suppression Due to Maternal Selim Kurto¤lu1, Dilek Sar›c›1, Mustafa Ali Ak›n1, Ghaniya Daar2, Levent Korkmaz1, fieyma Memur11 Erciyes University Faculty of Medicine, Department of Pediatrics Division of Neonatology, Kayseri, Turkey 2 Nevflehir Government Hospital, Deparment of Pediatrics, Nevflehir, Turkey Introduction Corticosteroids administered during pregnancy o
 Cardiovascular morbidity and multifactorial primary prevention: Fifteen-year follow-up of the Helsinki Businessmen Study*
T. E. Strandberg*, U. V. Salomaa**, V A. Naukkarinen***, H. T. Vanhanen*, S. J. Sarna****, and T. A. Miettinen*
' Department of Medicine, University of Helsinki. * National Public Health Institute, Helsinki, ** Jorvi Hospital, Espoo, ' "Department of Public Health, University of Helsinki, Helsinki, Finland
Objective: Mortality and morbidity in a long-term follow-up after a multifactorial primary prevention of cardiovascular
Design? The five-year randomized controlled multifactorial prevention trial for CVD was performed between 1974-1980.
Evaluation of participants (including electrocardiograms) was performed at start, end of trial and five years post-trial. CVD morbidity and mortality follow-up, using ' the country-wide Hospital Discharge Register and Death Certificate Register, was continued up to the end of 1989.
Setting: Second Department of Medicine, University of Helsinki.
Participants: In all, 3490 business executives born during 1919-34participated in health check-ups in the late 1960s. In
1974,1222 of these men who were clinically healthy, but with CVD risk factors, were entered into the primary prevention trial; 612 randomized to an intervention group and 610 to a control group. In addition, 593 men, who volunteered for the study but were excluded because of low levels of CVD risk factors, were followed- up as a nonrandomized low-risk group.
Correspondence to: T. Strandberg, M.D., Department of Medicine, University
of Helsinki, FIN-00290 Helsinki, Finland.
Key words: prevention, cholesterol, beta-blockers, cardiovascular diseases,
Received: 21 December 93; accepted:! June 1994.
"Presented partly at the 32nd Annual Conference on Cardiovascular Epidemiology, March 19-20,1992, Memphis IN, and the 65th Scientific Sessions of the American Heart Association, November 16-19,1992, New Orleans, USA
Interventions: During the five-year trial in 1974-1980 the subjects of the intervention group visited the investigators every
fourth month. They were treated with intensive dietetic-hygienic measures and frequently with hypolipidemic (mainly clofibrate and/or probucol), and antihypertensive (mainly pindolol or propranolol and/or hydrochlorothiazi-de plus amiloride) drugs. The control group and the low-risk group were not treated by the investigators.
Main outcome measures: Coronary mortality, nonfatal clinical and silent myocardial infarction (Ml), coronary artery
bypass grafting (CABG), fatal and nonfatal ischemic stroke, transient ischemic attack (TIA) leading to hospitali-zation, fatal and nonfatal hemorrhagic stroke (subarachnoid and intracerebral hemorrhage).
Results: The total number of fifteen-year coronary events was 75 in the intervention group, 49 in the control group (p<0.05
vs intervention) and 26 in the low-risk group (p<0.05 vs intervention and control). The respective numbers of coronary deaths were 34,14 and 6; of definite or probable MI 32, 30 and 17 (posttrial 16, 24 and 15); of CABG 5, 0 and 0 and of ischemic cerebrovoscular events 8, 20 (p<0.05 vs intervention) and 14. In multifactoriai analysis coronary events were positively associated with serum cholesterol (negatively with HDL-cholesterol), blood pressure and smoking in the intervention and control groups, and with serum triglycerides in the low-risk group. Basal alcohol consumption was a significant predictor of fewer coronary events in the intervention group but not in the control groups. In-trial pindolol treatment of the intervention group, but not the overall beta-blocker treatment, was associated with total (OR 197, 95% CI 103-3.78) and nonfatal coronary events
(or 2.51, 95% Cl 1.06-5.93) but not with coronary mortality or with post-trial total or nonfatal coronary events. Associations with other drug treatments tended to be protective only with diuretics.
Summary: Low traditional CHD risk factor levels are "ssociated with low coronary morbidity also in this popula-.^jn of
middle-aged men. Total coronary events were more frequent, mainly due to coronary deaths, in the intervention group than in the control group. Nonfatal coronary events in the intervention group were significantly associated with the frequent in-trial use ofpindolol, a beta-blocker with intrinsic sympathomimetic activity. Stroke incidence was low in the intervention group.
Several multifactorial primary prevention studies were started during the 1970's in order to efficiently control the
development of cardiovascular diseases (CVD, for a recent review see 1). Many of these trials had quite meager or even disappointing results, often interpreted to be due to modest risk factor lowering. However, risk factor reduction was substantial in the Helsinki Businessmen Study (2, 3); yet, 15-year follow-up showed increased total, coronary
id violent mortality in the intervention group as compa-red to the randomized control group (2, 4, 5). The results have
evoked several speculations about causes (6-10), but even though the multidrug treatments of the trial were suspected, no clear-cut explanation could have been elucidated for the result. We have now extended the follow-up to include nonfatal coronary and cerebrovascular events during the 15-year follow-up. For comparison, the respective morbidity will be reported also for a non-randomized low-risk group of the same background population presented in the initial intervention trial (2,3).
Study population and intervention methods
The details of the Helsinki Businessmen Study have been described in previous reports (2-5). Participants had to be free of
vascular disease but have at least one of the following risk factors: 1) serum cholesterol level £ 7.0 mmol/liter; 2) serum triglycerides level > 1.7 mmol/liter; 3) systolic blood pressure > 160 mm Hg; 4) diastolic blood pressure > 95 mmHg; 5) smoking > 10 cigarettes/day; 6) relative body weight 120% or higher; 7) one-hour glucose
tolerance (1 g/kg body weight of glucose orally) > 9.0 mmol/liter. In addition to the randomized high-risk control and intervention groups of 610 and 612 men, respectively, we also identified in 1974-75 a group of 593 men who volunteered for the trial, but were excluded because of low level of risk factors. This group has been referred to as the low-risk group.
The members of the intervention group visited the investigators every fourth month during the 5-year intervention period,
while the control group and the low risk group were in usual health care. Drug treatment (mainly beta-blockers propranolol or pindolol and/or diuretics hydroch-lorothiazide chloride alone or combined with amiloride for hypertension; probucol and clofibrate for hyperlipidemias) was used, if target levels were not reached by hygienic measures (smoking cessation, physical exercise, diet instructions, weight reduction) alone. Diet instructions advised reduced intake of calories, saturated fat, cholesterol, alcohol and sugar, and increased intake of polyunsatu-rated fats, fish, chicken, veal and vegetables. At end-trial most of the individual risk factors were reduced in the intervention group so that the total coronary heart disease (CHD) risk score was substantially smaller in the intervention group than in the control group (2). However, the levels of the low-risk group were not reached (2).
At the end-trial all participants were informed of their laboratory results and were advised to continue the health check-
ups and possible treatments in usual health care. Probucol therapy was discontinued because the drug is not registered in Finland.
The first and second post-trial follow-up evaluations including only mortality were performed in 1985-86 and 1990.
They have been described in detail in the respective reports (4,5). The risk factor levels and use of drugs in the three groups were studied in 1985-86 using questionnaires and routine laboratory methods (11) and the results are summarized in Table 1.
For the present report the cases of nonfatal myocardial infarction (covering ICD-9 codes 410-412) and ischemic and
hemorrhagic cerebrovascular events (ICD-9 codes 430-438) up to December 31, 1989 were collected from the country-wide Hospital Discharge Register. This includes the personal 10-digit code, unique for every citizen in Finland; the hospital code; diagnosis number and the treatment period. Thus, the hospital-made diagnoses of myocardial infarction (MI), transient ischemic attacks (TIA) or stroke can be reliably identified using this register. More
TABLE 1
Cardiovascular morbidity and multifactorial primary prevention: Fifteen-year follow-up of the Helsinki Businessmen Study*
T. E. Strandberg*, U. V. Salomaa**, V A. Naukkarinen***, H. T. Vanhanen*, S. J. Sarna****, and T. A. Miettinen*
' Department of Medicine, University of Helsinki. * National Public Health Institute, Helsinki, ** Jorvi Hospital, Espoo, ' "Department of Public Health, University of Helsinki, Helsinki, Finland
Objective: Mortality and morbidity in a long-term follow-up after a multifactorial primary prevention of cardiovascular
Design? The five-year randomized controlled multifactorial prevention trial for CVD was performed between 1974-1980.
Evaluation of participants (including electrocardiograms) was performed at start, end of trial and five years post-trial. CVD morbidity and mortality follow-up, using ' the country-wide Hospital Discharge Register and Death Certificate Register, was continued up to the end of 1989.
Setting: Second Department of Medicine, University of Helsinki.
Participants: In all, 3490 business executives born during 1919-34participated in health check-ups in the late 1960s. In
1974,1222 of these men who were clinically healthy, but with CVD risk factors, were entered into the primary prevention trial; 612 randomized to an intervention group and 610 to a control group. In addition, 593 men, who volunteered for the study but were excluded because of low levels of CVD risk factors, were followed- up as a nonrandomized low-risk group.
Correspondence to: T. Strandberg, M.D., Department of Medicine, University
of Helsinki, FIN-00290 Helsinki, Finland.
Key words: prevention, cholesterol, beta-blockers, cardiovascular diseases,
Received: 21 December 93; accepted:! June 1994.
"Presented partly at the 32nd Annual Conference on Cardiovascular Epidemiology, March 19-20,1992, Memphis IN, and the 65th Scientific Sessions of the American Heart Association, November 16-19,1992, New Orleans, USA
Interventions: During the five-year trial in 1974-1980 the subjects of the intervention group visited the investigators every
fourth month. They were treated with intensive dietetic-hygienic measures and frequently with hypolipidemic (mainly clofibrate and/or probucol), and antihypertensive (mainly pindolol or propranolol and/or hydrochlorothiazi-de plus amiloride) drugs. The control group and the low-risk group were not treated by the investigators.
Main outcome measures: Coronary mortality, nonfatal clinical and silent myocardial infarction (Ml), coronary artery
bypass grafting (CABG), fatal and nonfatal ischemic stroke, transient ischemic attack (TIA) leading to hospitali-zation, fatal and nonfatal hemorrhagic stroke (subarachnoid and intracerebral hemorrhage).
Results: The total number of fifteen-year coronary events was 75 in the intervention group, 49 in the control group (p<0.05
vs intervention) and 26 in the low-risk group (p<0.05 vs intervention and control). The respective numbers of coronary deaths were 34,14 and 6; of definite or probable MI 32, 30 and 17 (posttrial 16, 24 and 15); of CABG 5, 0 and 0 and of ischemic cerebrovoscular events 8, 20 (p<0.05 vs intervention) and 14. In multifactoriai analysis coronary events were positively associated with serum cholesterol (negatively with HDL-cholesterol), blood pressure and smoking in the intervention and control groups, and with serum triglycerides in the low-risk group. Basal alcohol consumption was a significant predictor of fewer coronary events in the intervention group but not in the control groups. In-trial pindolol treatment of the intervention group, but not the overall beta-blocker treatment, was associated with total (OR 197, 95% CI 103-3.78) and nonfatal coronary events
(or 2.51, 95% Cl 1.06-5.93) but not with coronary mortality or with post-trial total or nonfatal coronary events. Associations with other drug treatments tended to be protective only with diuretics.
Summary: Low traditional CHD risk factor levels are "ssociated with low coronary morbidity also in this popula-.^jn of
middle-aged men. Total coronary events were more frequent, mainly due to coronary deaths, in the intervention group than in the control group. Nonfatal coronary events in the intervention group were significantly associated with the frequent in-trial use ofpindolol, a beta-blocker with intrinsic sympathomimetic activity. Stroke incidence was low in the intervention group.
Several multifactorial primary prevention studies were started during the 1970's in order to efficiently control the
development of cardiovascular diseases (CVD, for a recent review see 1). Many of these trials had quite meager or even disappointing results, often interpreted to be due to modest risk factor lowering. However, risk factor reduction was substantial in the Helsinki Businessmen Study (2, 3); yet, 15-year follow-up showed increased total, coronary
id violent mortality in the intervention group as compa-red to the randomized control group (2, 4, 5). The results have
evoked several speculations about causes (6-10), but even though the multidrug treatments of the trial were suspected, no clear-cut explanation could have been elucidated for the result. We have now extended the follow-up to include nonfatal coronary and cerebrovascular events during the 15-year follow-up. For comparison, the respective morbidity will be reported also for a non-randomized low-risk group of the same background population presented in the initial intervention trial (2,3).
Study population and intervention methods
The details of the Helsinki Businessmen Study have been described in previous reports (2-5). Participants had to be free of
vascular disease but have at least one of the following risk factors: 1) serum cholesterol level £ 7.0 mmol/liter; 2) serum triglycerides level > 1.7 mmol/liter; 3) systolic blood pressure > 160 mm Hg; 4) diastolic blood pressure > 95 mmHg; 5) smoking > 10 cigarettes/day; 6) relative body weight 120% or higher; 7) one-hour glucose
tolerance (1 g/kg body weight of glucose orally) > 9.0 mmol/liter. In addition to the randomized high-risk control and intervention groups of 610 and 612 men, respectively, we also identified in 1974-75 a group of 593 men who volunteered for the trial, but were excluded because of low level of risk factors. This group has been referred to as the low-risk group.
The members of the intervention group visited the investigators every fourth month during the 5-year intervention period,
while the control group and the low risk group were in usual health care. Drug treatment (mainly beta-blockers propranolol or pindolol and/or diuretics hydroch-lorothiazide chloride alone or combined with amiloride for hypertension; probucol and clofibrate for hyperlipidemias) was used, if target levels were not reached by hygienic measures (smoking cessation, physical exercise, diet instructions, weight reduction) alone. Diet instructions advised reduced intake of calories, saturated fat, cholesterol, alcohol and sugar, and increased intake of polyunsatu-rated fats, fish, chicken, veal and vegetables. At end-trial most of the individual risk factors were reduced in the intervention group so that the total coronary heart disease (CHD) risk score was substantially smaller in the intervention group than in the control group (2). However, the levels of the low-risk group were not reached (2).
At the end-trial all participants were informed of their laboratory results and were advised to continue the health check-
ups and possible treatments in usual health care. Probucol therapy was discontinued because the drug is not registered in Finland.
The first and second post-trial follow-up evaluations including only mortality were performed in 1985-86 and 1990.
They have been described in detail in the respective reports (4,5). The risk factor levels and use of drugs in the three groups were studied in 1985-86 using questionnaires and routine laboratory methods (11) and the results are summarized in Table 1.
For the present report the cases of nonfatal myocardial infarction (covering ICD-9 codes 410-412) and ischemic and
hemorrhagic cerebrovascular events (ICD-9 codes 430-438) up to December 31, 1989 were collected from the country-wide Hospital Discharge Register. This includes the personal 10-digit code, unique for every citizen in Finland; the hospital code; diagnosis number and the treatment period. Thus, the hospital-made diagnoses of myocardial infarction (MI), transient ischemic attacks (TIA) or stroke can be reliably identified using this register. More
TABLE 1 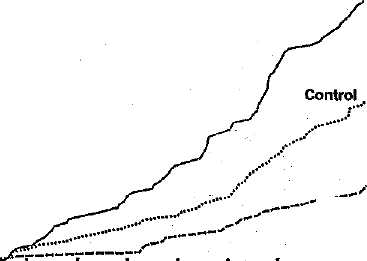 Intervention
Intervention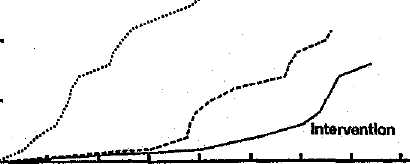 /
/