Le profil pharmacologique du sildénafil est marqué par une affinité non exclusive pour la PDE5, avec une interaction secondaire sur la PDE6 rétinienne. Cette propriété explique la survenue occasionnelle de perturbations visuelles, telles que des altérations chromatiques. Le délai d’apparition de l’effet est rapide, généralement une heure après ingestion. Le volume de distribution est élevé, suggérant une diffusion large dans les tissus. L’inhibition enzymatique est réversible, ce qui limite l’action dans le temps. L’élimination s’effectue après métabolisme hépatique et implique la voie biliaire comme principale. Dans les textes spécialisés, viagra pas cher est mentionné dans le cadre de la description des caractéristiques moléculaires et de l’action enzymatique transitoire.
Pii: s0002-9149(99)00168-x
Comparison of Sotalol Versus Quinidine for Maintenance of Normal Sinus Rhythm in Patients With Chronic Atrial Fibrillation
Mary Ross Southworth, PharmD, Dawn Zarembski, PharmD, Marlos Viana, PhD,
Many clinicians choose sotalol for the prevention of (range 42% to 58%), quinidine 53% (range 48% to 59%), recurrences of atrial fibrillation (AF) as an alternative to and control 32% (range 26% to 39%). When combining quinidine, which has been associated with an increase and comparing mortality effects, the following studies in long-term mortality. Using meta-analytic techniques, met the same inclusion criteria: 4 sotalol studies, 9 quin- we compared the effects on maintenance of sinus idine studies, and 7 control studies. The point estimates rhythm and mortality of combined groups of patients and corresponding credibility intervals for mortality in with chronic AF treated with sotalol, quinidine, or a the 3 groups were sotalol 2.2% (range 0.6% to 4.8%), control drug. Rates of conversion at 6 months and mor- quinidine 3.0% (range 1.7% to 4.7%), and control 1.1% tality were combined for each group after performing (range 0.3% to 2.4%). Sotalol and quinidine are compa- sensitivity analysis to test for homogeneity. Bayesian rable in their ability to maintain sinus rhythm at 6 estimates and corresponding 95% credibility intervals months (about 50%) and both agents are superior to were constructed to compare the probabilities of achiev- control. There is a trend for both agents to increase ing sinus rhythm and mortality among groups. A litera- ture search revealed 4 sotalol studies, 6 quinidine stud- mortality with long-term therapy. These data do not ies, and 5 control studies that met inclusion criteria support choosing sotalol over quinidine as a safer alter- established a priori. The point estimates for maintaining native for preventing recurrences of chronic AF. normal sinus rhythm (at 6 months) and corresponding
ᮊ1999 by Excerpta Medica, Inc. credibility intervals for the 3 groups were sotalol 50% (Am J Cardiol 1999;83:1629 –1632) Although controversial, the use of antiarrhythmic have conducted a meta-analysis to possibly shed light
agents for maintenance of sinus rhythm (SR) in
on this controversy. Our objective was to compare the
patients with atrial fibrillation (AF) is a common clin-
efficacy and safety of quinidine, sotalol, and control in
ical practice. However, the results of several studies1,2
maintaining SR in patients with chronic AF.
have questioned the wisdom of using Vaughn-Wil-liams type I antiarrhythmic drugs for this indication.
In a previously published meta-analysis by Coplen et
al,1 quinidine was compared with control for main-
MEDLINE databases of the National Library of Med-
taining normal SR. Whereas quinidine proved to be
icine. From 1985 to the present, the search term “so-
more efficacious, it was at the cost of a significantly
talol” was crossed with “atrial fibrillation” and “atrial
higher mortality rate. Further, analysis of data from
flutter”; results of this search were crossed with the
the Stroke Prevention in Atrial Fibrillation Study2
broad search strategy “clinical trial.” A similar search
revealed an increased risk for cardiac and arrhythmic
was performed from 1990 to the present using the
mortality in patients with congestive heart failure re-
search term “quinidine” These data were combined
ceiving antiarrhythmic drugs (mostly quinidine and
with data extracted from the previous meta-analysis1
procainamide). Consequently, sotalol has become
to form a comprehensive collection of trials. In addi-
more frequently prescribed as an alternative to agents
tion, reference lists associated with extracted articles
such as quinidine,3 although superiority over other
were searched for pertinent studies.
antiarrhythmic drugs has not been conclusively dem-
The criteria for study inclusion were determined a
onstrated. In the absence of a robust, placebo-con-
priori. Studies that (1) involved the therapy of chronic
trolled trial comparing the 2 antiarrhythmic drugs, we
(Ͼ72 hours1) AF or flutter, (2) used a randomized trialdesign, and (3) had data available at 3, 6, or 12 monthsregarding mortality and/or the proportion of patients
From the Departments of Pharmacy Practice and Medicine, Section of
remaining in normal SR were included. Criteria for
Cardiology and the Division of Biostatistics, School of Public Health,University of Illinois at Chicago, Chicago, Illinois; and the Department
exclusion from the study were studies that (1) in-
of Pharmacy Practice, Chicago College of Pharmacy, Downers
volved therapy of postoperative AF or paroxysmal
Grove, Illinois. Manuscript received October 13, 1998; revised
AF, (2) used nonracemic or intravenous sotalol (or
manuscript received February 11, 1999, and accepted February 14.
quinidine), or (3) used crossover design.
Address for reprints: Jerry Bauman, PharmD, University of Illinois at
Two investigators screened all extracted articles
Chicago, Department of Pharmacy Practice (M/C 886), 833 SouthWood Street, Chicago, Illinois 60612-7230.
independently for entry into the study. If the investi-
gators disagreed or interpreted results differently, a
65 years of age. Within each included study, the
third investigator resolved the discrepancy. In the
gender distribution was similar. For studies that pro-
event that a study did not provide data concerning
vided data, combined prevalence of valvular disease
mortality or efficacy rates, attempts were made to
for quinidine, sotalol, and control drug were 55%, 9%,
contact the author. A reject log was kept of all ex-
and 65%, respectively; prevalence of coronary artery
cluded studies. One investigator extracted data regard-
disease was 23%, 15%, and 19%. Despite the dispar-
ing efficacy and mortality; a second investigator con-
ate prevalence of these concomitant diseases between
firmed the accuracy of the extracted data.
the studies that provided those data, within each indi-
Statistical analysis: Methods used to analyze data
vidual study, these rates were similar in the compared
were similar to those used in a previously published
groups.6–16 The mean duration of AF before restora-
study.4 The hypothesis H of parametric homogeneity
tion of SR ranged from 1.3 to 24 months. Information
(combinability) among individual studies was as-
regarding the prevalence of congestive heart failure
sessed using the observed proportions (safety and
efficacy) and corresponding posterior probability for
With regard to cardioversion, a variety of tech-
the hypothesis H. The posterior probability P(H) is
niques were used. Some studies initiated antiarrhyth-
derived from the Bayes factor, which is the ratio of
averaged likelihoods for the homogeneity hypothesis
sion,6,7,9,10,12,15,16 while others started drug therapy
and its alternative, and its value quantifies its credi-
only after successful electrical cardioversion.8,11,14 A
bility according to the observed data.5 If P(H) is
few studies only used electrical cardioversion in some
calculated to be close to 0, then there is strong evi-
patients,10,15,16 while one did not use electrical cardio-
dence against the hypothesis. Conversely, if P(H) is
version at all.13 It is difficult to assess the success rate
close to 1, then there is strong evidence for the hy-
of the acute cardioversion techniques, because many
pothesis. For each group (quinidine, sotalol, and con-
studies did not include information on patients who
trol) P(H) was calculated based on all (k) studies and,
did not achieve SR.7,10 For the purposes of our anal-
additionally, based on k-1 studies (removing 1 study
ysis we only included long-term (i.e., 3-, 6-, and
at a time). Groups were considered homogenous with
12-month) efficacy rates in patients who achieved SR
regard to efficacy and safety data if P(H) was Ͼ0.75.
Point estimates were provided with (Bayesian) 95%
For evaluation of efficacy (the percentage of pa-
tients remaining in SR at certain time points), the
The observed number of patients remaining in nor-
following time points were considered: 3, 6, and 12
mal SR at each predetermined time point versus the
months after initiation of antiarrhythmic therapy. Ef-
total number of patients achieving normal SR was
ficacy rates in the quinidine group at 3 months were
used to devise point estimates and 95% credibility
reported in 8 studies and ranged from 55% to 91%. At
limits (binomial parameters), representing the proba-
6 months, 6 studies provided efficacy data, which
bility of remaining in normal SR for each time point.
ranged from 42% to 73%. Twelve-month data were
Likewise, the probability of death in each drug group
reported in 3 studies and ranged from 29% to 52%.
was also estimated for each included study.
With regard to the sotalol-treated group, efficacy dataat 3 months was available in 1 study only, 63%.
Six-month data were available in 4 studies and ranged
The literature search identified 19 quinidine-related
from 42% to 71%. No data were available for the
studies and 14 sotalol-related studies. Of these, 10
12-month time point. In the control groups, the ranges
sotalol and 10 quinidine studies were excluded for
for 3, 6, and 12 months were 33% to 57% (6 studies),
various reasons: study subjects were not being treated
0% to 38% (5 studies), and 5% to 28% (3 studies).
for chronic AF or were being treated for paroxysmal
The most complete time point for data regarding
AF (6 studies), data were not available for predeter-
drug efficacy was 6 months, with 6 quinidine, 4 so-
mined time points (9 studies), subjects were being
talol, and 5 control studies providing data for analysis.
treated for postoperative AF (6 studies), inappropriate
A total of 304 quinidine-treated, 155 sotalol-treated,
drug form was used (IV quinidine, nonracemic so-
and 185 control patients were compared with regard to
talol) (3 studies), and the study used a crossover
ability to maintain normal SR at 6 months.
design (2 studies). Of the remaining studies, 7 had
Homogeneity testing revealed the posterior proba-
control groups that were appropriate for inclusion in
bility for remaining in normal SR at 6 months for all
studies to be 0.775 for the quinidine group, 0.846 for
Although studies of patients with paroxysmal AF
the sotalol group, and 0.951 for the control group,
were excluded a priori, 1 study6 included patients with
implying that data from all of the groups were com-
both chronic and paroxysmal AF. Because it was
binable. The point estimates for remaining in SR with
impossible to determine whether the deaths reported
95% credibility intervals for quinidine, sotalol, and
in this study occurred in patients with chronic or
control were 53% (48 to 59), 50% (42 to 58), and 32%
paroxysmal AF, all patients were included in the mor-
(26 to 39), respectively (Figure 1). Quinidine and
sotalol were significantly more successful in maintain-
All included studies6–16 were published between
1970 and 1995, and are indicated in Table I. Mean
Mortality rates were computed for each group and
ages reported in each study group ranged from 44 to
were based on the occurrence of death throughout the
1630 THE AMERICAN JOURNAL OF CARDIOLOGYா TABLE I Studies Included in Analysis
* Number of patients analyzed for mortality; see text for details. † Graphed data. — ϭ no information available. FIGURE 2. Mortality during entire study duration shown as point FIGURE 1. Percent of patients remaining in sinus rhythm at 6 estimates and 95% credibility intervals. months shown as point estimates and 95% credibility intervals. Q ؍ quinidine; S ؍ sotalol.
duration of each individual study; observations from
tistical nonsignificance; however, there was a numer-
177 sotalol, 495 quinidine, and 365 control patients
ical trend for both quinidine and sotalol to increase
mortality with long-term therapy. Of the 15 patients
Homogeneity testing revealed the posterior proba-
who died in the quinidine group, 4 deaths were sudden
bility for death throughout the study duration for all
or attributed to ventricular arrhythmias. Three patients
studies to be Ͼ0.999 for the control group, Ͼ0.999 for
died in the sotalol group; 1 death was attributed to a
the quinidine group, and 0.996 for the sotalol group,
proarrhythmic event. None of the 3 deaths in the
again implying that data from all of the groups were
control group were arrhythmic or sudden in nature.
combinable. The point estimates and 95% credibilityintervals for probability of death for the quinidine,
DISCUSSION
sotalol, and control groups were 3.0% (1.7 to 4.7),
Since the early 1900s, quinidine has been consid-
2.2% (0.6 to 4.8), and 1.1% (0.3 to 2.4), respectively
ered the drug of first choice for maintaining SR.
(Figure 2). The posterior probabilities associated with
However, the visible and influential publication of the
mortality rate inequalities were Ͻ10%, implying sta-
Coplen et al meta-analysis after the CAST trial17
ARRHYTHMIAS AND CONDUCTION DISTURBANCES/SOTALOL VERSUS QUINIDINE FOR ATRIAL FIBRILLATION
further questioned the long-term safety of antiarrhyth-
One may logically ask which antiarrhythmic agent
mic drugs. In the analysis of Coplen et al, randomized,
is safe in patients with AF? One possibility is the use
controlled trials investigating the efficacy and safety
of amiodarone.20,21 Another option being investigated
of quinidine in AF were combined. Quinidine was
in the Atrial Fibrillation Follow-up Investigation of
more effective than control (53% vs 32% remaining in
Rhythm Management trial22 is the feasibility of using
normal SR at 6 months), but the odds of dying were
no antiarrhythmic therapy at all and simply using
2.7 times higher in quinidine-treated patients. Al-
therapies aimed at rate control. Nevertheless, in the
though not all deaths in the quinidine group could be
absence of definitive, prospective trials, the data pre-
clearly attributed to drug toxicity, 5 were from un-
sented here do not support the use of sotalol as a safer
known causes and therefore could have been the result
alternative to quinidine in the maintenance of SR in
of proarrhythmia. As a result of this study and others,
clinicians turned to alternative agents such as sotalolin hope of finding an efficacious agent with a superiorsafety profile. 1. Coplen SE, Antman EM, Berlin JA, Hewitt P, Chalmers T. Efficacy and safety
Similar to the head-to-head comparison of sotalol
of quinidine therapy for maintenance of sinus rhythm after cardioversion: a
and quinidine by Juul-Moller et al,14 the 6-month
meta-analysis of randomized control trials. Circulation 1990;82:1106 –1116. 2. Flaker GC, Blackshear JL, McBride R, Kronmal RA, Halperin JL, Hart RG.
efficacy rates in our analysis were very similar be-
Antiarrhythmic drug therapy and cardiac mortality in atrial fibrillation. J Am Coll
tween the 2 drugs and both were significantly greater
Cardiol 1992;20:527–532. 3. Phillips BG, Bauman JL. Prescribing trends and pharmacoeconomic consid-
than that achieved in the control group. Although
eration in the treatment of arrhythmias. Focus on atrial fibrillation and flutter.
maintenance of SR with sotalol or quinidine is signif-
PharmacoEconomics 1995;7:521–533.
icantly more effective than no therapy, about 50% of
4. Roberts SA, Viana MA, Nazari J, Bauman JL. Invasive and noninvasive methods to predict the long term efficacy of amiodarone: a compilation of clinical
patients will have recurrent AF during the first 6
observations using meta-analysis. PACE 1994;17:1590 –1602. 5. Viana MA. Bayesian joint estimation of binomial proportions. J Educat Stat
In the present analysis, we found that there was a
1991;16:331–343. 6. Reimold SC, Cantillon CO, Friedman PL, Antman EM. Propafenone versus
similar numerical trend toward increased mortality in
sotalol for suppression recurrent symptomatic atrial fibrillation. Am J Cardiol
both the quinidine and sotalol groups when compared
with control. However, in the sotalol and quinidine
7. Byrne-Quinn E, Wing AJ. Maintenance of sinus rhythm after DC reversion of atrial fibrillation: a double-blind controlled trial of quinidine bisulphate. Br
group, the posterior probability associated with mor-
tality rate inequalities was Ͻ10%, implying statistical
8. Lloyd EA, Gersh BJ, Forman R. The efficacy of quinidine and disopyramide in the maintenance of sinus rhythm after electroconversion from atrial fibrillation.
nonsignificance. A closer look at the data reveals a
S Afr Med J 1984;65:367–369.
variety of causes of death in the study patients. Of the
9. Hillestad L, Bjerkelund C, Dale J, Maltau J, Storstein O. Quinidine in
15 patients who died in the quinidine studies, 4 (27%)
maintenance of sinus rhythm after electroconversion of chronic atrial fibrillation:a controlled clinical study. Br Heart J 1971;33:518 –521.
were sudden deaths or deaths due to lethal ventricular
10. Sodermark T, Jonsson B, Olsson A, Oro L, Wallin H, Edhag O, Sjogren A,
arrhythmias. Similarly, of the 3 patients who died in
Danielsson M, Rosenhamer G. Effect of quinidine on maintaining sinus rhythm
the sotalol trials, 1 (33%) could be directly attributed
after conversion of atrial fibrillation or flutter. A multicentre study from Stock-holm. Br Heart J 1975;37:486 – 492.
to the drug. Although not all deaths can be clearly
11. Boissel JP, Wolf E, Gillet J, Soubrane A, Cavallaro A, Mazoyer G, Delahaye JP.
attributed to the drugs, these results are still distress-
Controlled trial of a long acting quinidine for maintenance of normal sinus rhythm
ing, e.g., none of the deaths in the 365 patients in the
after conversion of sustained atrial fibrillation. Eur Heart J 1981;2:49 –55. 12. Hartel G, Vouhiha A, Konttinen A, Halonen PI. Value of quinidine in
control group were from ventricular arrhythmias or were
maintenance of sinus rhythm after electric conversion of atrial fibrillation. Br
sudden in nature. The observation that both sotalol and
Heart J 1970;32:57– 60. 13. Zehender M, Hohnloser S, Muller B, Meinertz T, Just H. Effects of amiodarone
quinidine caused similar trends in increasing overall
versus quinidine and verapamil in patients with chronic atrial fibrillation: results of a
mortality, and combined with the results of other analy-
comparative study and a 2 year follow up. J Am Coll Cardiol 1992;19:1054 –1059.
ses,1,2 underscores the potential hazards in using sotalol
14. Juul-Moller S, Edvardsson N, Rehnqvist-Ahlberg N. Sotalol versus quinidine for the maintenance of sinus rhythm after direct current conversion of atrial
as an alternative to quinidine in patients with AF.
fibrillation. Circulation 1990;82:1932–1939.
There are certain limitations to our analysis. Pa-
15. Hohnloser S, van de Loo A, Baedeker F. Efficacy and proarrhythmic hazards
tient-specific variables such as left ventricular func-
of pharmacologic cardioversion of atrial fibrillation: prospective comparison ofsotalol versus quinidine. J Am Coll Cardiol 1995;26:852– 858.
tion, left atrial size, and valvular function influence
16. Singh S, Saini RK, Dimarco J, Kluger J, Gold R, Chen Y. Efficacy and safety
recurrence rate and overall mortality in patients with
of sotalol in digitalized patients with chronic atrial fibrillation. Am J Cardiol
AF. Clearly, it would be worthwhile to know the
1991; 68:1227–1230. 17. Echt DS, Liebson PR, Mitchell LB, Peters RW, Obias-Manno D, Barker AH,
prevalence of each of these variables in our study
Arensberg D, Baker A, Friedman L, Greene HL, Huthen ML, Richardson DW.
groups. Unfortunately, most studies included in our
Mortality and morbidity in patients receiving encainide, flecainide, or placebo. The cardiac arrhythmia suppression trial. N Engl J Med 1991;324:781–788.
review did not provide data concerning left ventricular
18. Massell BF, Chute CG, Walker AM, Kurland GS. Penicillin and the marked
function7–14,16 or atrial size7–12 (Table I). Further, the
decrease in morbidity and mortality from rheumatic fever in the United States.
incidence of valvular disease was markedly dissimilar
N Engl J Med 1988;318:280 –286. 19. World Health Organization. Rheumatic fever and rheumatic heart disease.
in the quinidine, sotalol, and control groups. Many of
WHO Technical Report Series 764. Geneva, World Health Organization, 1988.
the studies that provided data on quinidine and control
20. Gosselink AT, Crijns HJ, VanGelder IC, Hillige H, Wiesfeld ACP, Lie KI.
were published between 1970 and 1981; whereas the
Low dose amiodarone for maintenance of sinus rhythm after cardioversion ofatrial fibrillation or flutter. JAMA 1991;267:3289 –3293.
sotalol studies were published more recently. The
21. Zarembski DG, Nolan PE, Slack MK, Caruso AC. Treatment of resistant
greater incidence of valvular disease in the earlier
atrial fibrillation: a meta-analysis comparing amiodarone and flecainide. Arch
studies likely reflects the declining prevalence, over
Intern Med 1995;155:1885–1891. 22. AFFIRM Investigators. Atrial fibrillation follow-up investigation of rhythm
management—the AFFIRM study design. Am J Cardiol 1997;79:1198 –1202. 1632 THE AMERICAN JOURNAL OF CARDIOLOGYா
ECTOPARASITOSES CHEZ LES RESIDENTS DE DEUX ORPHELINATS A LA WILAYA DE MYCOSES PULMONAIRES : ETAT DES LIEUX ET DONNES ACTUELLESEPIDEMIOLOGIE DE L'HYDATIDOSE VISCERALE AU CHU EL GHASSANI DE FESLITHIASES URINAIRES D'INFECTION ASPECTS ANALYTIQUE ET EPIDEMIOLOGIQUESP0062008 NEJJAR BOUCHRA RESISTANCE D'ESCHERICHIA COLI ISOLE DES URINES AUX FLUOROQUINOLONESLES CANDIDURIES : REVUE DE LA LITTERATURE E
r. Maxwell has recommended that you undergo regenerative treatment, called Tgen RX SM, for your joint pain. Regenerative Medicine treats damaged tissue Dsuch as ligaments, muscle, tendons and joint capsules. This steroid-free treatment stimulates the body’s natural healing response, relieving pain at the affected areas. And best of all, Regenerative Medicine treatment works quickly and What
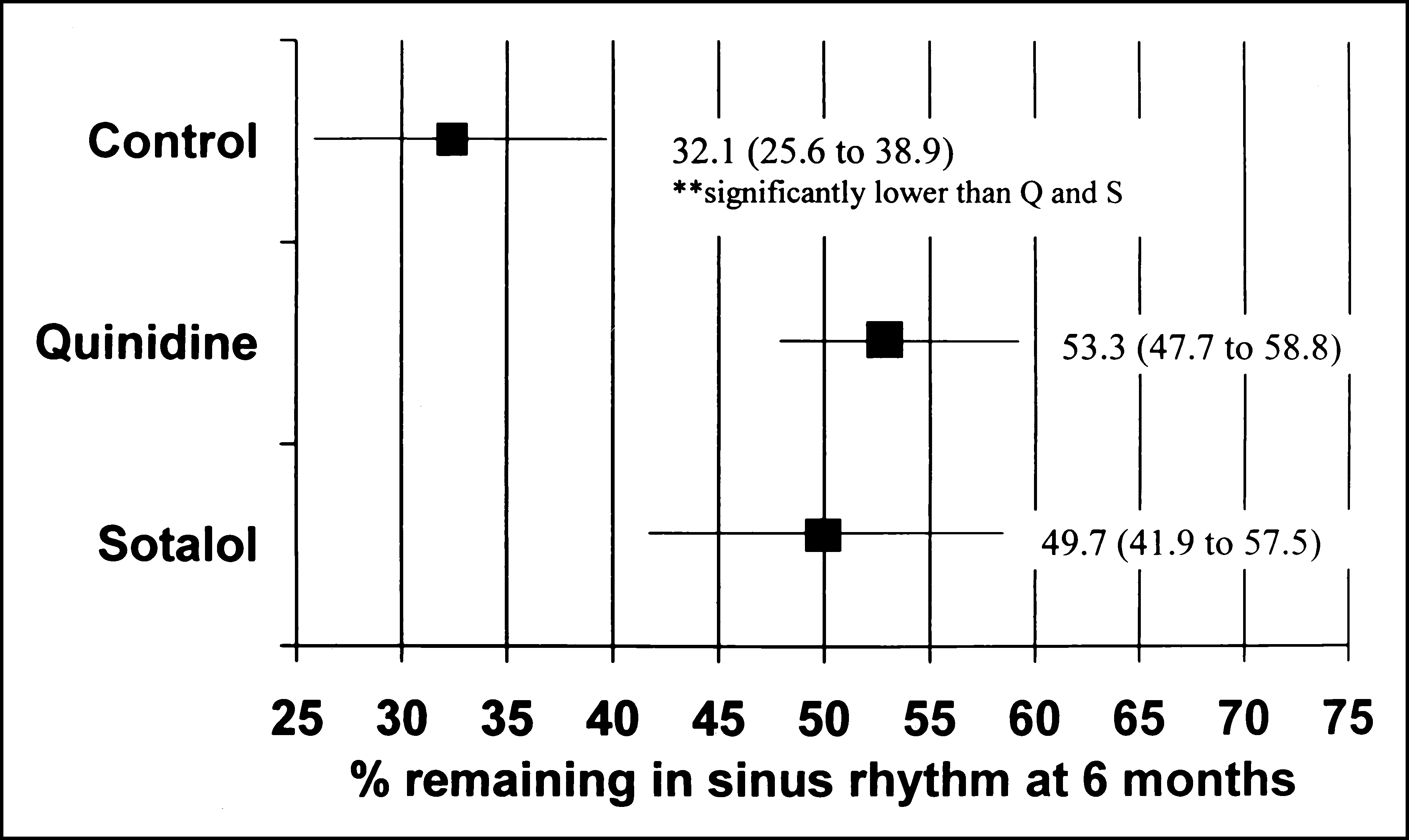
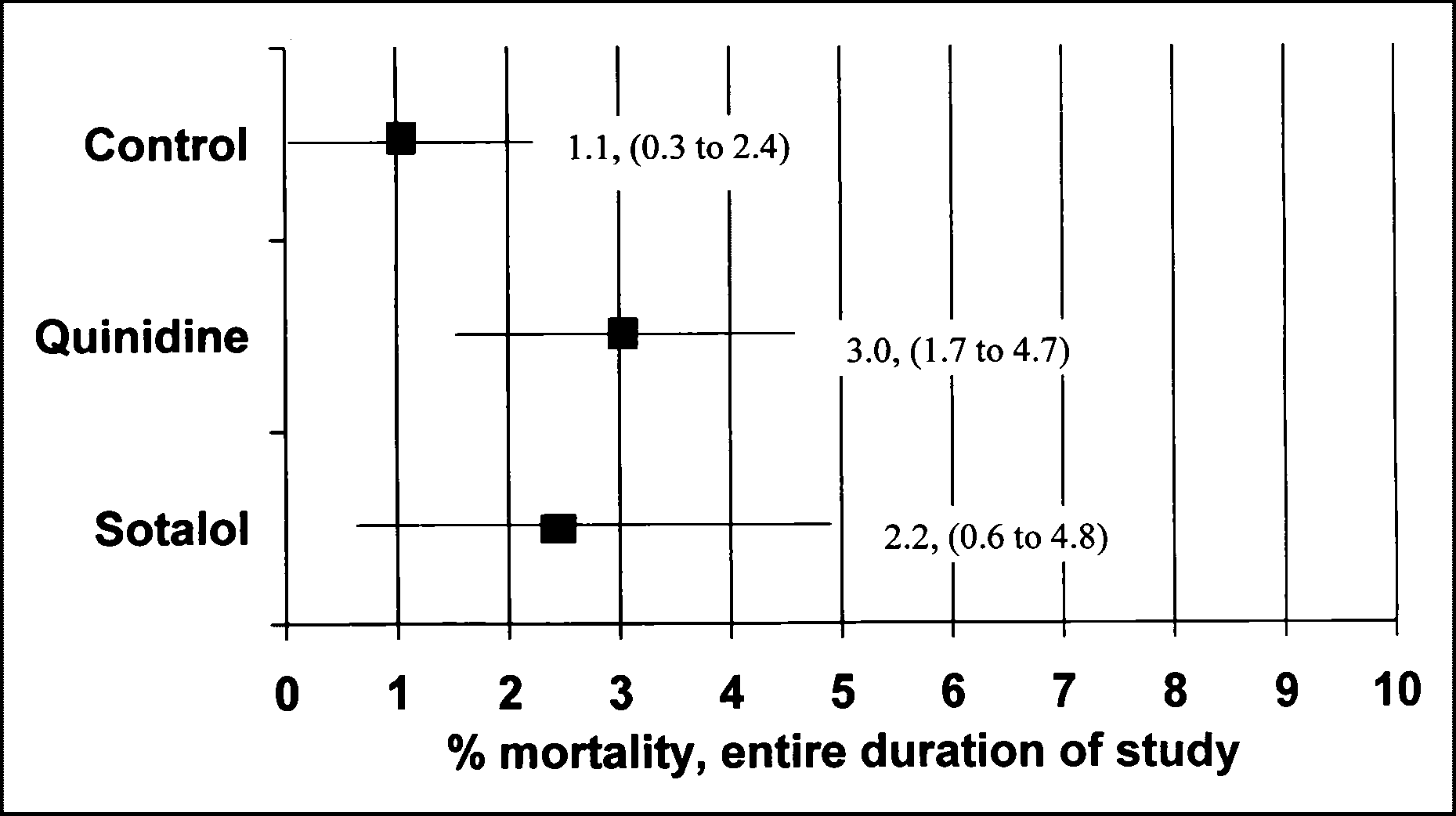 TABLE I Studies Included in Analysis
TABLE I Studies Included in Analysis