Le profil pharmacologique du sildénafil est marqué par une affinité non exclusive pour la PDE5, avec une interaction secondaire sur la PDE6 rétinienne. Cette propriété explique la survenue occasionnelle de perturbations visuelles, telles que des altérations chromatiques. Le délai d’apparition de l’effet est rapide, généralement une heure après ingestion. Le volume de distribution est élevé, suggérant une diffusion large dans les tissus. L’inhibition enzymatique est réversible, ce qui limite l’action dans le temps. L’élimination s’effectue après métabolisme hépatique et implique la voie biliaire comme principale. Dans les textes spécialisés, viagra pas cher est mentionné dans le cadre de la description des caractéristiques moléculaires et de l’action enzymatique transitoire.
A general introduction to the subject of depression
A General Introduction to the Subject of Depression
[Chicago Pastoral Conference, September 11-12, 1989]
Introduction
Never have so many people been so unhappy. A poll has shown that one out of two people say that they
Depression is the least understood but one of the most serious emotional problems of our time. From all
indications it is on the increase. According to the National Institute of Mental Health, 8 million people a year may suffer depression severe enough to warrant being treated by a doctor. More than 500,000 Americans were hospitalized in 1980 for depression.
Unfortunately, a frequent outcome of depression is suicide. Of the estimated 20,000 to 50,000 suicides
in the United States each year, as many as three-quarters occur among persons suffering from depression. (Statistics gained through the National Center for Health Statistics, HEW.)
Depression goes beyond anxiety. The symptoms of anxiety are a pounding heart, troubled breathing,
trembling, giddiness, nervousness, and hot and cold spells. The symptoms of depression include all of these plus fatigue, inability to eat, restlessness, boredom, an inability to concentrate on the daily tasks of life, a feeling of “going to pieces,” and physical complaints such as a backache, muscle ache, or skin conditions. Crying spells are common in depression.
Anxiety may be fleeting. Depression may persist for years. Anxiety is highly visible. Depression is
obscure. Anxiety clamors for relief. Depression hides in silence.
Depression can be said to be an emotional state of dejection and sadness. There are all degrees of
depression, ranging from discouragement and downheartedness to feelings of utter hopelessness and despair.
Mild depression is marked by unhappiness and pessimism. A sufferer from mild depression often feels
inadequate and loses interest in the social environment. It is nothing to be alarmed about. Such depression is a normal condition of existence. (Witness even the life of the Christian whose life is marked by peaks and valleys.) However, mild depression may progress to a moderate stage. The same symptoms are seen, but they are severe enough to interfere with the way an individual functions. Conversation is difficult. There is an inability to think. In its most severe form, depression sees a marked change of behavior. Initiative is lost. The individual is overly concerned with feelings of unworthiness and guilt.
The Bible also has something, to say about depression and shows us quite clearly what it is. “Day and night thy hand was heavy upon me,” David cried (Ps. 32:4). The hand of God pressed hard
upon him. He literally felt depressed (pressed down). It was as if God’s hand were crushing him. He believed depression was from God and considered it the merciful punishment of God warning him and leading him to repentance. The sense of guilt crushed him. “My moisture,” he says, “is turned into the drought of summer.” The effects of this anxiety upon his body were evident. The saliva in his mouth dried up (a natural response in an anxiety state).
The 51st Psalm parallels Psalm 32 in many respects. The two Psalms refer to the same event. In Psalm
51 David wrote about his sin against Uriah and Bathsheba. The Psalm is a record of what he said after Nathan accused him of adultery and murder. In Verse 3 he described the anxiety state caused by his guilty conscience prior to repentance. He wrote: “My sin is ever before me.” (Note how the writer of Proverbs vividly pictures the effects of a haunting guilty conscience. Proverbs 28:1—“The wicked flee when no one pursues but the righteous are bold as a lion.”) Jay Adams in his book Competent to Counsel explains that this way:
A guilty conscience leads to fear, and a good conscience leads to boldness. The wicked flee in many ways. Henry was burdened with a guilty conscience. Walking down the street one day, he saw Ron coming his way. Henry knew he had wronged Ron in a business deal. Seeing Ron, Henry was suddenly
afraid and felt as if he had to avoid him at all costs. He turned a corner as quickly as he could and escaped. He felt as if he would do almost anything to avoid meeting Ron. Because Henry had wronged him, Ron had become a stressor to Henry. Unforgiven sinners are vulnerable people. They often become intensely self-conscious. Even innocent words frequently are interpreted as personal attacks. They interpret as personal affronts acts that have no direct relationship to them. A guilty person may claim that a sermon was a personal attack, or lacking the courage to do so, will object to some incidental feature of the sermon or some supposed slight of the minister. To call such a person paranoid is to misinterpret the dynamics of his problem. On the other hand, a person at peace with God and with other men is invulnerable and can be bold as a lion. (Jay Adams, Competent to Counsel, pp. 117-118)
This same kind of conscience was at work in King David accusing him of sin. Constantly, day and night,
it haunted him. He cried out, “Make me to hear joy and gladness that the bones which thou hast broken may rejoice” (Verse 8). The condition which before he had likened to aching bones produced such sharp pain that they felt like they were broken. The same picture is given is Psalm 38:1. Here David describes his condition like that of a wounded soldier, staggering about with God’s arrows in him. In Verses 3 and 4 he enlarges again upon his depressed condition, “There is no soundness in my flesh because of thy anger, nor is there any rest in my bones because of my sin, for my iniquities have gone over my head. Like a heavy burden they are too heavy for me.”
The pressure of the feeling of quilt was overbearing. David loathed his condition. It was so distasteful he
could only cry out: “My wounds stink and are rotten because of my foolishness” (Verse 5). He moaned, “I am greatly troubled, I am bowed down greatly, I go mourning all the day long.” No one figure of speech was adequate to describe his misery. David described himself as a wounded soldier lying helpless on the battlefield. Such agony of soul was as if he were being cursed under a load heavier than he could carry. It was as though he mourned over the death of a loved one. He says, “My loins are filled with a burning. There is no soundness in my flesh.” Pain filled his body. He declared: “I am feeble and painfully broken. I have roared because of the groaning of my heart,” and he prayed, “Lord, all of my desire is before thee, and my groaning is not hidden from thee. My heart pants. My strength fails me.”
David came to the end of his rope; he was in despair. He felt he could endure the pain no longer. He was
about to give up. At that point, he recalled the cause of these sufferings, and resolved to adopt the only solution to the problem: “I am ready to fall, and my pain is always before me. I will declare my iniquity. I will be sorry for my sin” (Verses 17-18).
These passages in Psalms 51 and 38 are parallel to Psalm 32. All three Psalms speak of the same kind of
anxiety, the same sort of depression, the same type of physical distress, and the same class of emotion visceral responses. All three describe the anxiety of a man who is guilty over his sin and who is crushed by that anxiety. To summarize then, David’s first contention was: hiding sin causes distress both of soul and of body (Psalm 32:3, 4). (Jay Adams, Competent to Counsel, pp. 116-119)
This is basically what depression has to do with. Here in the biblical account of David’s sin we explore
one kind of depression, albeit a very common form, the cause of which (guilt) underlies many of the forms depression takes. A diagram which might accurately describe this is:
Depression, in whatever form it takes, is a result of sin. God created man in his own image so that man
would dominate the world. Sin brought the reversal of man’s rule over the earth so that the earth gained dominion over man. Our spiritual enemies, sin, death, and the power of the devil, would destroy us in whatever way they can. Christ reversed that trend by defeating our enemies. In Christ we can now perform all things. With that in mind, let’s take a brief look at how psychologists view depression.
Depression has been called by mental health professionals “the common cold of psychopathology.”
Depressions come in all sizes, shapes, kinds and degrees, however. They, can range from very mild, transient episodes that might be labeled the “blues” to very severe forms of depression in which one’s bodily processes may actually be slowed down to a life-threatening degree.
There are numerous technical distinctions among the various types and kinds of depression: psychotic
depression, neurotic depression, manic depression, involutional melancholia (change of life depression), post-partum depression, endogenous or exogenous depression. Though these distinctions and labels may be important to the therapist working with depression, they are not very meaningful to the depressed person. People may tend to impute more “craziness” to themselves than most of these labels imply. They are then convinced they really do have a problem. They feel, once they have a label, that they really are a “Mental case” or “crazy” (whatever that means) or “psychologically disabled” or “emotionally disturbed.” Most of these technical labels are merely a shorthand system for communication between professionals and are not disease categories as most people tend to think of them.
Let’s go through some of these different kinds of depression just so we get a feel for what we’re talking
about. We will follow here the brief definitions as set down by Roger Barrett in his book entitled “Depression” What It Is and What to Do About It. Psychotic depression: This is a very severe kind of depression. There is usually some loss of contact
with reality. Delusions (irrational false beliefs) or hallucinations (sensing things not there) are usually present. There may be something called “psychomotor retardation.” This refers to a slowing down of bodily processes. The person may move so slowly or talk so quietly and slowly that it’s hard to follow him.
Another severe depression is termed manic depressive. This originally referred to cases of mood or
feeling excess that usually involved an alternation of moods from depression to euphoria and excitement and then back to a depressed mood again, etc. However, persons who don’t necessarily show alternation of moods have also been classified here. This label usually implies that the person has no obvious reason for his extremes in moods. There is supposedly no outside reason to explain or account for his extremes of feeling.
The neurotic depression is a more mild form of depression. The person experiences no loss of contact
with reality. He usually continues to function in his life tasks, but only with great difficulty. He suffers from an acute loss of self-esteem and has problems motivating himself.
Involutional melancholia refers to the stage of life for both men and women when they go through
physiological changes that make it less likely that they will be able to reproduce. This is frequently an agitated depression, i.e., rather than being slowed down, the person is highly agitated and anxious. He is likely to be very restless and tense. Hypochondriacal preoccupation is very frequent. (That simply means that the person has aches and pains that they focus on and are highly concerned about.) They frequently doubt their competency. They feel worthless.
Post-partum depression refers to a continuing depressed mood experienced by a woman following
childbirth. It usually doesn’t last long, but the problem is that at this very time she is much needed by the newborn child.
One very interesting depression has been called “success depression.” This is not a technical category,
but happens frequently enough to be viewed as a syndrome of its own. It is interesting because it appears to be a paradox. It appears to occur following the successful accomplishment of a long-term goal when the individual has put in long periods of time and disciplined effort. Earning a degree in a long-term program like an M.D. or Ph.D. is an example of this. Once achieved, you’d expect absolute euphoria and utter bliss rather than
depression, but for some people the period immediately following the accomplishment of this long sought after goal is followed by a down period of emptiness and depression.
It all seems so baffling. Why would anyone feel blue for “arriving”? Actually it can be explained in part
by the old proverb, “the grass is always greener on the other side of the fence.” Once we get to the other side of the fence, it seems the grass is never quite as different as it had appeared from our previous perspective. And the weeds -- they are always there. (But you frequently have to get up close to see them clearly.) Nietzsche of the nihilistic philosophical vain spoke of the “melancholia of everything completed.” I think this suggests that the attaining of goals always leaves us with a loss of some kind, a vacuum that needs to be filled. That may also account to some degree for this so called “success depression.”
Sometimes a distinction is made between endogenous or exogenous depression. Endogenous means
internally caused or originating within the body, and exogenous means externally or environmentally caused or originating outside the body. Sometimes the word reactive is used with similar meaning to exogenous. Since it is often difficult to determine whether a depression is directly attributable to outside events or inside factors, this distinction can be somewhat arbitrary. As a result, the terms endogenous and exogenous are used by some practitioners to refer to different patterns of symptoms in depression.
It may be that problems such as alcoholism and some forms of obesity are actually forms of depression.
Mental health professionals sometimes speak of “masked depression,” which means that the usual symptoms of depressions may be covered up by other kinds of behaviors. Excessive drinking is a good example. The individual may resort to drinking to cope with his bad feelings. An outsider may not see the depressed symptoms, but only the excessive drinking behavior. Or, someone else may resort to eating excessively when down or blue. When these ways of coping with bad feelings become habitual, we may not see the depression so much as the habitual behavior. These, of course, will only temporarily mask the depression, and in the long run they become part of a vicious cycle that will only make the depression worse.
These are some of the most common types of depression. But here are a couple of things to watch for so
that you do not confuse depression with other mental and physical characteristics.
Depression is to be distinguished from “the blues.” Many of us feel down in the dumps at times. It is
only normal to have low points, which can occur under all sorts of circumstances. Christmas, holidays, parties, reunions, etc. may trigger such a period of “the blues” which is really loneliness.
Weekend blues arise from a guilt feeling on the part of those who seem to be saying, “I don’t deserve to
enjoy myself.” Men or women working for five straight days with their time fully occupied, doing something useful and doing it well, reach the weekend, when they are supposed to relax and enjoy themselves. Many people do not know how to do that. They either sink into lethargy or over-react in more activity or drinking.
The weekend is also the time when a husband and wife who do not see a great deal of each other during
weekdays are with one another under conditions in which maladjustments and problems surface.
A Sunday blues occurs in some people who have been raised in a religious environment in which going
to church was a regular part of their lives. If these individuals have stopped their church practices, they find themselves depressed. They know that something is not right. They see no reason to go to church, yet at the same time they feel an emotional vacuum.
Another kind of “blues” is the “post-vacation blues.” Many people come back from a vacation with a
tired, turned-off, slack and sluggish feeling. They find it difficult to get back to the “pressure cooker” and the responsibilities of the job after having lived the “good life.” Fortunately, this “blah” feeling wears off in a couple of days.
A more serious form of post-vacation blues occurs in the individual who begrudges the time he took off.
He is a “work freak.” Work is his whole life, and he cannot seem to enjoy anything else. His blues come on before, during, and after vacation. Before he leaves he gets gangplank fever. He worries about who will work while he is away, and the volume that will be there when he returns. A work addict can get away from his job no easier than-a heavy drinker can get away from alcohol.
One last note along this line deals with the difference between depression and grief. Grief is a realistic
reaction to an actual loss about which there is full awareness. There are few psychosomatic symptoms, rarely any fear of an incurable disease, no fears of going insane. The grief-stricken person can concentrate and make decisions and manage his affairs.
In grief the loss is personal, objective, and readily understandable. The bereavement is realistic and in
proportion to what has been lost. It is self-limited and gradually subsides. In depression, on the other hand, the loss is much more complex. It is loss of self, the feeling of self-doubt, or self-contempt, even of self-loathing.
In summary, we can see that depressed people and depressed experiences vary both in quantity and
quality. Two persons, both of whom are experiencing depression, may have as many things different about their experience as similar. Not only are there multiple forms of expression of depression, but there are also many different causes of depression (as we will look at briefly next). Therefore, be careful how you apply what you read and learn concerning depression. Depression is much too complex to make easy individual application. What may be true for one depressed person may not in any way apply to another equally depressed person. (A. J. Snider and I. J. Adatto, M.D.’s, Learning How to Live with Nervous Tension, pp.62-79.)
In the next section of this paper, common causes of depression will be discussed. Since there is such a
wide range of opinions on this matter, we will try and describe just a few causes as simply and briefly as possible. This section, therefore, will not be exhaustive or inclusive.
First of all, we need to get the idea out of our heads that just because someone is depressed or has a
breakdown that he is emotionally weak. We all experience many of the same precipitating occurrences that bring on depression. The difference may be in our levels of tolerance and in the load. Dr. Roger Barrett points to “the straw that broke the camel’s back.” The camel’s broken back can be explained by a number of factors. Maybe we don’t have a very strong camel in the first place. He has a weak back. Or maybe he hasn’t worked with heavy loads enough. (Many people haven’t experienced enough stress in appropriate amounts in younger years to have learned how to cope with it.) The camel’s back is strong enough all right, but he just hasn’t worked out enough to build up supporting muscles. Or maybe it was the suddenness of the additional weight being added --too much all at once. He could have handled it had the load been added more gradually. Or maybe he’s carrying around such a heavy load all the time that he is constantly exhausted. (Many people constantly carry heavy loads of adverse past experiences around with them, which in turn keeps them emotionally run down.) (Roger Barrett, Depression, pp.26-27.)
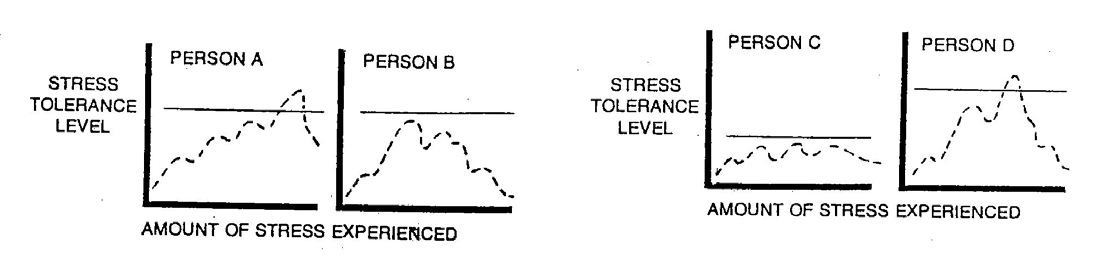
There is in clinical psychology something which is called frustration or stress tolerance level.
Individuals do not have the same tolerance level in coping with stress. The same adverse event may be a precipitating or triggering event for emotional problems or depression for one individual and no problem at all to another person whose stress tolerance level is higher. Our ability to tolerate stress relates to what we call the “predisposing” factors. A person who has experienced an emotional breakdown may be healthier than either you or I who haven’t had such an experience. It’s just that he has experienced more stress than we have. Here Dr. Barrett has a helpful diagram to help us get a clear picture.
A and B show two similar stress levels. As you can see, Person A has experienced more stress at one
point in time than has Person B. Unfortunately, and with some pharisaical disdain, someone will point to Person A and say, “He’s emotionally weak” or “He has mental problems.” They won’t say the same about Person B, even though A and B are really of equal emotional stability.
It is even possible that someone with a lower stress tolerance level (“weak emotionally”) may not
experience emotional disorder or breakdown when a much stronger person may because he has experienced much more stress.
Person C has less good mental health or emotional stability than Person D. But he never experiences
more stress than he can cope with. Person D has considerable more ability to cope with stress by comparison to person C, but he has also far more severe and stressful events and problems, and they have, on one occasion, exceeded his ability to handle them.
Here are some of the characteristic stress factors in depression. The triggering factor in depression is
known as a stress factor. Psychologists have identified certain of these stress factors.
For men stress factors are most often events like financial reversals, failures in vocational identity
(failure to get job or promotion, etc.) and failing physical powers.
For women the stress factors are somewhat different. The major factors appear to be such events as an
attack on her femininity (e.g., a mastectomy or hysterectomy). Also a stress factor for women is the feeling of being abandoned by important men in her life such as her father or husband. The loss of children or trouble at home are stress factors in females which trigger depression.
Dr. Barrett reminds the student of depression that most of the precipitating factors involved in bringing
on depression involve the sense of worth an individual has of himself. Apparently the female’s sense of worth is tied very closely to her appearance and her relationship to her family members, whereas a man’s sense of worth is more closely tied to his work and his physical prowess. We might question whether this should be true for the Christian especially. Should these identities mean so much to us that their loss can have devastating effect on our emotional well-being? The loss or removal of anything we overvalue in terms of our security can trigger depression. A pertinent question here is: Are these the areas of life in which the Christian is to place his security? I doubt it!
So then, loss of loved ones, things in general, physical appearance or ability may all be precipitators to
depression. But on occasion there may not be a critical event or loss that will trigger depression. Instead, a long series of stresses or simply chronic stress finally topples the person’s emotional well-being and depression enters.
Constant fear and anxieties if not checked can, use up energy and exhaust oneself. If such stress is
severe enough and applied long enough, the hormonal reserves of the body become depleted. This results in fatigue and eventually exhaustion. The feeling side of this physical experience is depression. Pastors!—Here is a strong argument against allowing ourselves to be uptight, tense, nervous, and anxious all of the time. Eventually it catches up with us, and we leave ourselves open to the risk of depression.
What are the symptoms of depression? According to Dr. Adatto, who writes in a book called Learning How to Live with Nervous Tension, a depressed person can be picked out if he has three main symptoms. “First, he is less interested in things than he used to be, whether these are work, hobbies, pets, friends, or people he loves. The second symptom is the fact that he cannot enjoy things as much as he-used to, whether it is a good dinner, a beautiful landscape, a theater performance, or some personal pleasure. Whatever it is, the enjoyment has gone out of it. The third symptom is that he cannot produce as much and as well as he did. a few months before. He gets fatigued much earlier and he cannot finish things” (p.66).
The seriously depressed person sees himself in a very negative way. He is convinced that he is “alone”
and helpless. He blames himself for ordinary faults and exaggerates his shortcomings. He is pessimistic not only about himself but about the world and the future. He wants to sleep for longer than usual. He may lose his appetite and lose weight, or eat more than normally and gain weight. Another characteristic, particularly evident in women, is crying spells, whether or not there is something to cry about. A severely depressed person often will say, “I’m scared I’m going out of my mind. I’ve been staring at the wall for three months. My children give
me no pleasure. I feel nothing for them. My husband has been forced to do the shopping and housework. I can’t move myself. I just can’t seem to do anything.”
Such people have lost confidence in themselves to carry out even the simple tasks of life. They describe
their depression as a wall between them and others. Many simply sleep all the time to avoid life’s troubles.
Some women express a sense of loss. They have gone through school, married, and raised children who
have grown up and left home and do not need them any more. The women sense a loss of purpose. Commonly, depressed people are more bothered by the body symptoms than by their sad feelings. They blame their mood on physical troubles. (“You’d be depressed too if you felt the pains I do.”) One study of 500 depressed patients showed that 74 percent had consulted a physician because of headaches, chest pains and the like. They believed that their mood change was the result, not the cause, of their body symptoms. Depression may masquerade as a skin condition, muscle aches and pains, urinary problems, stomach distress -- almost any bodily complaint.
There is no mistaking depression when the patient says that he has “no interest in living,” has feelings of
futility and hopelessness, and talks of wrist-slashing or jumping from a window or in front of a car. This is a red flare and calls for immediate steps to be taken.
The risk of suicide is great if the patient has an overwhelming sense of guilt and unworthiness, if he
talks of suicide or seems preoccupied with arranging his affairs.
At what point can a person tell if he should be seeking outside help for his depression? Here are some
general guidelines. He would be well advised to seek professional guidance if:
he finds himself continually unhappy with the way his life is going, he finds a marked drop in his ability to function at work, socially, and in his relationship
the condition persists for a month or two and he finds no specific reason for it and cannot
What kind of guidance should an individual seek? One would hope that Christians would first of all seek the
help and advice of their pastor. If indeed deep rooted feelings of inadequacy and guilt are at the heart of the depression, who better than God’s servant, the pastor, is able to apply Law and Gospel. Certainly the knowledgeable pastor will know his limits. He may first seek to find out if the problem is a medical or mental one. An easy way to help determine this is simply to send the patient to a physician as a matter of course for a routine physical. This will generally uncover any medical irregularities. If the problem is mental in nature, the pastor will seek to find the cause.
We have already noted somewhat how a pastor may be of help to the depressed. Let’s take a brief look also
at how the doctor or psychologist would deal with the depressed. Some doctors think drugs are very helpful. They claim that the introduction of antidepressant drugs has made the treatment of depression easier. Here are just a few samples. One type of antidepressant works by blocking the action of an enzyme in the brain that breaks down the chemical norepinephrine. In this way, it is believed, the drugs ensure adequate levels of the chemical. These include Marplan, Parnate, Nardil, and Eutonyl. A new class of antidepressant drugs, called tricyclics, prevent the breakdown of serotonin, the other major chemical believed to be involved in depression. These drugs include Tofranil and Sinequan.
When there is little of the chemicals norepinephrine and serotonin the emotional circuit is sluggish and a
person feels depressed. Just why there is a chemical drop in a depressed person is unknown. Drugs help restore the chemicals, but even if no drugs are used, nature eventually cures the bio-chemical illness. Drugs shorten the time and help a patient avoid needless suffering.
Sometimes drugs used in treatment have unpleasant side effects. Addiction is just one thing both doctor and
patient need to keep in mind. Here the doctor needs to monitor his patient carefully. There are many cases which have come to light in recent years where the doctor has not been responsible in this area.
Because the drugs are sometimes referred to as psychic energizers, a person might think they boost energies
to superhuman levels, like a missile fuel lifting a rocket into space. That is not the case. They are more like psychic restoratives, or psychic normalizers. They will act to lift the depressed energies of the patient up to his
best normal, but not beyond. There is no improvement in drive, character, or other attributes beyond those that were present before the depressive illness.
The drugs are convenient to take and enable family doctors to treat many depressions, and patients to
continue working while under medication. Clinical statistics show that drugs are effective in restoring patients to function in 50 to 80 percent of cases. Before there was a chemical treatment an average depression lasted two years. With chemical treatment, an average of 60 days will turn depressions around. These statistics are valid, I suppose, depending upon who you read. An article in Reader’s Digest (Dec. 1980, pp. 124-128) argues the method of “thinking one’s way out of depression.” According to their statistics, of 19 cognitive-therapy patients, 15 showed complete recovery. Only 5 of the 25 drug-therapy patients did as well, and 8 others dropped out because of side effects from the drug. A year later, 11 cognitive-therapy patients were still symptom-free—a significant finding since depression tends to become chronic.
Edward Ziegler, the author of “Think Your Way out of Depression,” states “that in cognitive therapy,
the doctor challenges the patient to listen to his own negative thoughts—trains him to identify these inner saboteurs and silence them. Results come quickly, usually within a few weeks.”
Dr. Burns offers these techniques to get the upper hand over your depression:
1. “Write down your negative thoughts. Don’t let them buzz in your head; snare them on
2. “Read over the list of cognitive distortions.”
3. “Substitute more objective thoughts that put the lie to the ones that made you depressed.”
Here is a sampling of the types of positive insights Burns offers to replace negative thoughts.
1. Your feelings are not facts! “Your feelings don’t even count, except to mirror your thinking. If
your thoughts make no sense, feelings they create will be just as absurd.”
2. You can cope. Even with genuine sadness due to real loss or disappointment, a substantial
portion of the suffering comes from thought distortion. “When you eliminate these distortions, coping with the real problem will become less painful.”
3. Don’t base your opinion of yourself on your achievements. “Self-worth based on
accomplishments is ‘pseudo-esteem’; not the genuine thing,” Burns says. You can’t base your self worth on looks, talent, fame or fortune. Marilyn Monroe, Freddie Prinze and other famous suicides attest to this grim truth. “Nor can love or approval add one iota to your inherent worth. Most depressed individuals are in fact much loved, but it doesn’t help. At the bottom line, only your own sense of self-worth determines how you feel.”
According to Ziegler, the main lesson of cognitive therapy is self-esteem. “Like yourself better and
“Self-esteem can be viewed as your decision to treat yourself like a beloved friend,” Burns says. He
asks: If a famous visitor came to stay with you, would you insult him? Would you peck away at his weaknesses and imperfections? Of course not. You would do everything you could to make your guest feel comfortable. “Now--why not treat yourself like that? Do it all the time!” (“Think you Way out of Depression,” Reader’s Digest, Dec. 1980, pp. 124-128.)
Obviously we cannot as Christians buy this kind of approach to depression. Rather we seek to let God’s
law point out our sins, we look at our disgusting state by nature and trust not in our own self-worth and esteem but in the active and passive righteousness of the God-man Jesus Christ who offered Himself as a sacrifice for us. This new status that we have as God’s children should go a long way in helping rid ourselves of depression. As blood-bought children of God, we have everything to live for; we really have hope—not only for this life but also for the life to come. It is indeed sad how many people will see secular counselors seeking to help them in their depression when only the Word of God will suffice. Here we see the need of mission work to solve man’s most basic need with the Gospel of the forgiveness of sins.
Guidelines on the use of Transdermal Fentanyl Patch Indications Fentanyl is a strong opioid which may be used in the management of cancer pain. Fentanyl patches may be suitable in patients who have: Intolerable side effects with oral morphine e.g. intractable constipation and vomiting (despite appropriate antiemetics) and hallucinations (despite haloperidol). Renal impairment as mor
http://www.medscape.com/viewarticle/811716_print'Heart Failure Is Killing Your Diabetes Patients,' Experts WarnBARCELONA, SPAIN — Cardiologists speaking here at the European Association for the Study of Diabetes (EASD) 2013 Meeting are urging diabetologists to sit up and take notice: heart failure is kil ing their patients and is not getting the attention it deserves. Not only is heart fail
 afraid and felt as if he had to avoid him at all costs. He turned a corner as quickly as he could and escaped. He felt as if he would do almost anything to avoid meeting Ron. Because Henry had wronged him, Ron had become a stressor to Henry. Unforgiven sinners are vulnerable people. They often become intensely self-conscious. Even innocent words frequently are interpreted as personal attacks. They interpret as personal affronts acts that have no direct relationship to them. A guilty person may claim that a sermon was a personal attack, or lacking the courage to do so, will object to some incidental feature of the sermon or some supposed slight of the minister. To call such a person paranoid is to misinterpret the dynamics of his problem. On the other hand, a person at peace with God and with other men is invulnerable and can be bold as a lion. (Jay Adams, Competent to Counsel, pp. 117-118)
This same kind of conscience was at work in King David accusing him of sin. Constantly, day and night,
it haunted him. He cried out, “Make me to hear joy and gladness that the bones which thou hast broken may rejoice” (Verse 8). The condition which before he had likened to aching bones produced such sharp pain that they felt like they were broken. The same picture is given is Psalm 38:1. Here David describes his condition like that of a wounded soldier, staggering about with God’s arrows in him. In Verses 3 and 4 he enlarges again upon his depressed condition, “There is no soundness in my flesh because of thy anger, nor is there any rest in my bones because of my sin, for my iniquities have gone over my head. Like a heavy burden they are too heavy for me.”
The pressure of the feeling of quilt was overbearing. David loathed his condition. It was so distasteful he
could only cry out: “My wounds stink and are rotten because of my foolishness” (Verse 5). He moaned, “I am greatly troubled, I am bowed down greatly, I go mourning all the day long.” No one figure of speech was adequate to describe his misery. David described himself as a wounded soldier lying helpless on the battlefield. Such agony of soul was as if he were being cursed under a load heavier than he could carry. It was as though he mourned over the death of a loved one. He says, “My loins are filled with a burning. There is no soundness in my flesh.” Pain filled his body. He declared: “I am feeble and painfully broken. I have roared because of the groaning of my heart,” and he prayed, “Lord, all of my desire is before thee, and my groaning is not hidden from thee. My heart pants. My strength fails me.”
David came to the end of his rope; he was in despair. He felt he could endure the pain no longer. He was
about to give up. At that point, he recalled the cause of these sufferings, and resolved to adopt the only solution to the problem: “I am ready to fall, and my pain is always before me. I will declare my iniquity. I will be sorry for my sin” (Verses 17-18).
These passages in Psalms 51 and 38 are parallel to Psalm 32. All three Psalms speak of the same kind of
anxiety, the same sort of depression, the same type of physical distress, and the same class of emotion visceral responses. All three describe the anxiety of a man who is guilty over his sin and who is crushed by that anxiety. To summarize then, David’s first contention was: hiding sin causes distress both of soul and of body (Psalm 32:3, 4). (Jay Adams, Competent to Counsel, pp. 116-119)
This is basically what depression has to do with. Here in the biblical account of David’s sin we explore
one kind of depression, albeit a very common form, the cause of which (guilt) underlies many of the forms depression takes. A diagram which might accurately describe this is:
Depression, in whatever form it takes, is a result of sin. God created man in his own image so that man
would dominate the world. Sin brought the reversal of man’s rule over the earth so that the earth gained dominion over man. Our spiritual enemies, sin, death, and the power of the devil, would destroy us in whatever way they can. Christ reversed that trend by defeating our enemies. In Christ we can now perform all things. With that in mind, let’s take a brief look at how psychologists view depression.
Depression has been called by mental health professionals “the common cold of psychopathology.”
Depressions come in all sizes, shapes, kinds and degrees, however. They, can range from very mild, transient episodes that might be labeled the “blues” to very severe forms of depression in which one’s bodily processes may actually be slowed down to a life-threatening degree.
There are numerous technical distinctions among the various types and kinds of depression: psychotic
depression, neurotic depression, manic depression, involutional melancholia (change of life depression), post-partum depression, endogenous or exogenous depression. Though these distinctions and labels may be important to the therapist working with depression, they are not very meaningful to the depressed person. People may tend to impute more “craziness” to themselves than most of these labels imply. They are then convinced they really do have a problem. They feel, once they have a label, that they really are a “Mental case” or “crazy” (whatever that means) or “psychologically disabled” or “emotionally disturbed.” Most of these technical labels are merely a shorthand system for communication between professionals and are not disease categories as most people tend to think of them.
Let’s go through some of these different kinds of depression just so we get a feel for what we’re talking
about. We will follow here the brief definitions as set down by Roger Barrett in his book entitled “Depression” What It Is and What to Do About It.
Psychotic depression: This is a very severe kind of depression. There is usually some loss of contact
with reality. Delusions (irrational false beliefs) or hallucinations (sensing things not there) are usually present. There may be something called “psychomotor retardation.” This refers to a slowing down of bodily processes. The person may move so slowly or talk so quietly and slowly that it’s hard to follow him.
Another severe depression is termed manic depressive. This originally referred to cases of mood or
feeling excess that usually involved an alternation of moods from depression to euphoria and excitement and then back to a depressed mood again, etc. However, persons who don’t necessarily show alternation of moods have also been classified here. This label usually implies that the person has no obvious reason for his extremes in moods. There is supposedly no outside reason to explain or account for his extremes of feeling.
The neurotic depression is a more mild form of depression. The person experiences no loss of contact
with reality. He usually continues to function in his life tasks, but only with great difficulty. He suffers from an acute loss of self-esteem and has problems motivating himself.
Involutional melancholia refers to the stage of life for both men and women when they go through
physiological changes that make it less likely that they will be able to reproduce. This is frequently an agitated depression, i.e., rather than being slowed down, the person is highly agitated and anxious. He is likely to be very restless and tense. Hypochondriacal preoccupation is very frequent. (That simply means that the person has aches and pains that they focus on and are highly concerned about.) They frequently doubt their competency. They feel worthless.
Post-partum depression refers to a continuing depressed mood experienced by a woman following
childbirth. It usually doesn’t last long, but the problem is that at this very time she is much needed by the newborn child.
One very interesting depression has been called “success depression.” This is not a technical category,
but happens frequently enough to be viewed as a syndrome of its own. It is interesting because it appears to be a paradox. It appears to occur following the successful accomplishment of a long-term goal when the individual has put in long periods of time and disciplined effort. Earning a degree in a long-term program like an M.D. or Ph.D. is an example of this. Once achieved, you’d expect absolute euphoria and utter bliss rather than
depression, but for some people the period immediately following the accomplishment of this long sought after goal is followed by a down period of emptiness and depression.
It all seems so baffling. Why would anyone feel blue for “arriving”? Actually it can be explained in part
by the old proverb, “the grass is always greener on the other side of the fence.” Once we get to the other side of the fence, it seems the grass is never quite as different as it had appeared from our previous perspective. And the weeds -- they are always there. (But you frequently have to get up close to see them clearly.) Nietzsche of the nihilistic philosophical vain spoke of the “melancholia of everything completed.” I think this suggests that the attaining of goals always leaves us with a loss of some kind, a vacuum that needs to be filled. That may also account to some degree for this so called “success depression.”
Sometimes a distinction is made between endogenous or exogenous depression. Endogenous means
internally caused or originating within the body, and exogenous means externally or environmentally caused or originating outside the body. Sometimes the word reactive is used with similar meaning to exogenous. Since it is often difficult to determine whether a depression is directly attributable to outside events or inside factors, this distinction can be somewhat arbitrary. As a result, the terms endogenous and exogenous are used by some practitioners to refer to different patterns of symptoms in depression.
It may be that problems such as alcoholism and some forms of obesity are actually forms of depression.
Mental health professionals sometimes speak of “masked depression,” which means that the usual symptoms of depressions may be covered up by other kinds of behaviors. Excessive drinking is a good example. The individual may resort to drinking to cope with his bad feelings. An outsider may not see the depressed symptoms, but only the excessive drinking behavior. Or, someone else may resort to eating excessively when down or blue. When these ways of coping with bad feelings become habitual, we may not see the depression so much as the habitual behavior. These, of course, will only temporarily mask the depression, and in the long run they become part of a vicious cycle that will only make the depression worse.
These are some of the most common types of depression. But here are a couple of things to watch for so
that you do not confuse depression with other mental and physical characteristics.
Depression is to be distinguished from “the blues.” Many of us feel down in the dumps at times. It is
only normal to have low points, which can occur under all sorts of circumstances. Christmas, holidays, parties, reunions, etc. may trigger such a period of “the blues” which is really loneliness.
Weekend blues arise from a guilt feeling on the part of those who seem to be saying, “I don’t deserve to
enjoy myself.” Men or women working for five straight days with their time fully occupied, doing something useful and doing it well, reach the weekend, when they are supposed to relax and enjoy themselves. Many people do not know how to do that. They either sink into lethargy or over-react in more activity or drinking.
The weekend is also the time when a husband and wife who do not see a great deal of each other during
weekdays are with one another under conditions in which maladjustments and problems surface.
A Sunday blues occurs in some people who have been raised in a religious environment in which going
to church was a regular part of their lives. If these individuals have stopped their church practices, they find themselves depressed. They know that something is not right. They see no reason to go to church, yet at the same time they feel an emotional vacuum.
Another kind of “blues” is the “post-vacation blues.” Many people come back from a vacation with a
tired, turned-off, slack and sluggish feeling. They find it difficult to get back to the “pressure cooker” and the responsibilities of the job after having lived the “good life.” Fortunately, this “blah” feeling wears off in a couple of days.
A more serious form of post-vacation blues occurs in the individual who begrudges the time he took off.
He is a “work freak.” Work is his whole life, and he cannot seem to enjoy anything else. His blues come on before, during, and after vacation. Before he leaves he gets gangplank fever. He worries about who will work while he is away, and the volume that will be there when he returns. A work addict can get away from his job no easier than-a heavy drinker can get away from alcohol.
afraid and felt as if he had to avoid him at all costs. He turned a corner as quickly as he could and escaped. He felt as if he would do almost anything to avoid meeting Ron. Because Henry had wronged him, Ron had become a stressor to Henry. Unforgiven sinners are vulnerable people. They often become intensely self-conscious. Even innocent words frequently are interpreted as personal attacks. They interpret as personal affronts acts that have no direct relationship to them. A guilty person may claim that a sermon was a personal attack, or lacking the courage to do so, will object to some incidental feature of the sermon or some supposed slight of the minister. To call such a person paranoid is to misinterpret the dynamics of his problem. On the other hand, a person at peace with God and with other men is invulnerable and can be bold as a lion. (Jay Adams, Competent to Counsel, pp. 117-118)
This same kind of conscience was at work in King David accusing him of sin. Constantly, day and night,
it haunted him. He cried out, “Make me to hear joy and gladness that the bones which thou hast broken may rejoice” (Verse 8). The condition which before he had likened to aching bones produced such sharp pain that they felt like they were broken. The same picture is given is Psalm 38:1. Here David describes his condition like that of a wounded soldier, staggering about with God’s arrows in him. In Verses 3 and 4 he enlarges again upon his depressed condition, “There is no soundness in my flesh because of thy anger, nor is there any rest in my bones because of my sin, for my iniquities have gone over my head. Like a heavy burden they are too heavy for me.”
The pressure of the feeling of quilt was overbearing. David loathed his condition. It was so distasteful he
could only cry out: “My wounds stink and are rotten because of my foolishness” (Verse 5). He moaned, “I am greatly troubled, I am bowed down greatly, I go mourning all the day long.” No one figure of speech was adequate to describe his misery. David described himself as a wounded soldier lying helpless on the battlefield. Such agony of soul was as if he were being cursed under a load heavier than he could carry. It was as though he mourned over the death of a loved one. He says, “My loins are filled with a burning. There is no soundness in my flesh.” Pain filled his body. He declared: “I am feeble and painfully broken. I have roared because of the groaning of my heart,” and he prayed, “Lord, all of my desire is before thee, and my groaning is not hidden from thee. My heart pants. My strength fails me.”
David came to the end of his rope; he was in despair. He felt he could endure the pain no longer. He was
about to give up. At that point, he recalled the cause of these sufferings, and resolved to adopt the only solution to the problem: “I am ready to fall, and my pain is always before me. I will declare my iniquity. I will be sorry for my sin” (Verses 17-18).
These passages in Psalms 51 and 38 are parallel to Psalm 32. All three Psalms speak of the same kind of
anxiety, the same sort of depression, the same type of physical distress, and the same class of emotion visceral responses. All three describe the anxiety of a man who is guilty over his sin and who is crushed by that anxiety. To summarize then, David’s first contention was: hiding sin causes distress both of soul and of body (Psalm 32:3, 4). (Jay Adams, Competent to Counsel, pp. 116-119)
This is basically what depression has to do with. Here in the biblical account of David’s sin we explore
one kind of depression, albeit a very common form, the cause of which (guilt) underlies many of the forms depression takes. A diagram which might accurately describe this is:
Depression, in whatever form it takes, is a result of sin. God created man in his own image so that man
would dominate the world. Sin brought the reversal of man’s rule over the earth so that the earth gained dominion over man. Our spiritual enemies, sin, death, and the power of the devil, would destroy us in whatever way they can. Christ reversed that trend by defeating our enemies. In Christ we can now perform all things. With that in mind, let’s take a brief look at how psychologists view depression.
Depression has been called by mental health professionals “the common cold of psychopathology.”
Depressions come in all sizes, shapes, kinds and degrees, however. They, can range from very mild, transient episodes that might be labeled the “blues” to very severe forms of depression in which one’s bodily processes may actually be slowed down to a life-threatening degree.
There are numerous technical distinctions among the various types and kinds of depression: psychotic
depression, neurotic depression, manic depression, involutional melancholia (change of life depression), post-partum depression, endogenous or exogenous depression. Though these distinctions and labels may be important to the therapist working with depression, they are not very meaningful to the depressed person. People may tend to impute more “craziness” to themselves than most of these labels imply. They are then convinced they really do have a problem. They feel, once they have a label, that they really are a “Mental case” or “crazy” (whatever that means) or “psychologically disabled” or “emotionally disturbed.” Most of these technical labels are merely a shorthand system for communication between professionals and are not disease categories as most people tend to think of them.
Let’s go through some of these different kinds of depression just so we get a feel for what we’re talking
about. We will follow here the brief definitions as set down by Roger Barrett in his book entitled “Depression” What It Is and What to Do About It.
Psychotic depression: This is a very severe kind of depression. There is usually some loss of contact
with reality. Delusions (irrational false beliefs) or hallucinations (sensing things not there) are usually present. There may be something called “psychomotor retardation.” This refers to a slowing down of bodily processes. The person may move so slowly or talk so quietly and slowly that it’s hard to follow him.
Another severe depression is termed manic depressive. This originally referred to cases of mood or
feeling excess that usually involved an alternation of moods from depression to euphoria and excitement and then back to a depressed mood again, etc. However, persons who don’t necessarily show alternation of moods have also been classified here. This label usually implies that the person has no obvious reason for his extremes in moods. There is supposedly no outside reason to explain or account for his extremes of feeling.
The neurotic depression is a more mild form of depression. The person experiences no loss of contact
with reality. He usually continues to function in his life tasks, but only with great difficulty. He suffers from an acute loss of self-esteem and has problems motivating himself.
Involutional melancholia refers to the stage of life for both men and women when they go through
physiological changes that make it less likely that they will be able to reproduce. This is frequently an agitated depression, i.e., rather than being slowed down, the person is highly agitated and anxious. He is likely to be very restless and tense. Hypochondriacal preoccupation is very frequent. (That simply means that the person has aches and pains that they focus on and are highly concerned about.) They frequently doubt their competency. They feel worthless.
Post-partum depression refers to a continuing depressed mood experienced by a woman following
childbirth. It usually doesn’t last long, but the problem is that at this very time she is much needed by the newborn child.
One very interesting depression has been called “success depression.” This is not a technical category,
but happens frequently enough to be viewed as a syndrome of its own. It is interesting because it appears to be a paradox. It appears to occur following the successful accomplishment of a long-term goal when the individual has put in long periods of time and disciplined effort. Earning a degree in a long-term program like an M.D. or Ph.D. is an example of this. Once achieved, you’d expect absolute euphoria and utter bliss rather than
depression, but for some people the period immediately following the accomplishment of this long sought after goal is followed by a down period of emptiness and depression.
It all seems so baffling. Why would anyone feel blue for “arriving”? Actually it can be explained in part
by the old proverb, “the grass is always greener on the other side of the fence.” Once we get to the other side of the fence, it seems the grass is never quite as different as it had appeared from our previous perspective. And the weeds -- they are always there. (But you frequently have to get up close to see them clearly.) Nietzsche of the nihilistic philosophical vain spoke of the “melancholia of everything completed.” I think this suggests that the attaining of goals always leaves us with a loss of some kind, a vacuum that needs to be filled. That may also account to some degree for this so called “success depression.”
Sometimes a distinction is made between endogenous or exogenous depression. Endogenous means
internally caused or originating within the body, and exogenous means externally or environmentally caused or originating outside the body. Sometimes the word reactive is used with similar meaning to exogenous. Since it is often difficult to determine whether a depression is directly attributable to outside events or inside factors, this distinction can be somewhat arbitrary. As a result, the terms endogenous and exogenous are used by some practitioners to refer to different patterns of symptoms in depression.
It may be that problems such as alcoholism and some forms of obesity are actually forms of depression.
Mental health professionals sometimes speak of “masked depression,” which means that the usual symptoms of depressions may be covered up by other kinds of behaviors. Excessive drinking is a good example. The individual may resort to drinking to cope with his bad feelings. An outsider may not see the depressed symptoms, but only the excessive drinking behavior. Or, someone else may resort to eating excessively when down or blue. When these ways of coping with bad feelings become habitual, we may not see the depression so much as the habitual behavior. These, of course, will only temporarily mask the depression, and in the long run they become part of a vicious cycle that will only make the depression worse.
These are some of the most common types of depression. But here are a couple of things to watch for so
that you do not confuse depression with other mental and physical characteristics.
Depression is to be distinguished from “the blues.” Many of us feel down in the dumps at times. It is
only normal to have low points, which can occur under all sorts of circumstances. Christmas, holidays, parties, reunions, etc. may trigger such a period of “the blues” which is really loneliness.
Weekend blues arise from a guilt feeling on the part of those who seem to be saying, “I don’t deserve to
enjoy myself.” Men or women working for five straight days with their time fully occupied, doing something useful and doing it well, reach the weekend, when they are supposed to relax and enjoy themselves. Many people do not know how to do that. They either sink into lethargy or over-react in more activity or drinking.
The weekend is also the time when a husband and wife who do not see a great deal of each other during
weekdays are with one another under conditions in which maladjustments and problems surface.
A Sunday blues occurs in some people who have been raised in a religious environment in which going
to church was a regular part of their lives. If these individuals have stopped their church practices, they find themselves depressed. They know that something is not right. They see no reason to go to church, yet at the same time they feel an emotional vacuum.
Another kind of “blues” is the “post-vacation blues.” Many people come back from a vacation with a
tired, turned-off, slack and sluggish feeling. They find it difficult to get back to the “pressure cooker” and the responsibilities of the job after having lived the “good life.” Fortunately, this “blah” feeling wears off in a couple of days.
A more serious form of post-vacation blues occurs in the individual who begrudges the time he took off.
He is a “work freak.” Work is his whole life, and he cannot seem to enjoy anything else. His blues come on before, during, and after vacation. Before he leaves he gets gangplank fever. He worries about who will work while he is away, and the volume that will be there when he returns. A work addict can get away from his job no easier than-a heavy drinker can get away from alcohol.
 One last note along this line deals with the difference between depression and grief. Grief is a realistic
reaction to an actual loss about which there is full awareness. There are few psychosomatic symptoms, rarely any fear of an incurable disease, no fears of going insane. The grief-stricken person can concentrate and make decisions and manage his affairs.
In grief the loss is personal, objective, and readily understandable. The bereavement is realistic and in
proportion to what has been lost. It is self-limited and gradually subsides. In depression, on the other hand, the loss is much more complex. It is loss of self, the feeling of self-doubt, or self-contempt, even of self-loathing.
In summary, we can see that depressed people and depressed experiences vary both in quantity and
quality. Two persons, both of whom are experiencing depression, may have as many things different about their experience as similar. Not only are there multiple forms of expression of depression, but there are also many different causes of depression (as we will look at briefly next). Therefore, be careful how you apply what you read and learn concerning depression. Depression is much too complex to make easy individual application. What may be true for one depressed person may not in any way apply to another equally depressed person. (A. J. Snider and I. J. Adatto, M.D.’s, Learning How to Live with Nervous Tension, pp.62-79.)
In the next section of this paper, common causes of depression will be discussed. Since there is such a
wide range of opinions on this matter, we will try and describe just a few causes as simply and briefly as possible. This section, therefore, will not be exhaustive or inclusive.
First of all, we need to get the idea out of our heads that just because someone is depressed or has a
breakdown that he is emotionally weak. We all experience many of the same precipitating occurrences that bring on depression. The difference may be in our levels of tolerance and in the load. Dr. Roger Barrett points to “the straw that broke the camel’s back.” The camel’s broken back can be explained by a number of factors. Maybe we don’t have a very strong camel in the first place. He has a weak back. Or maybe he hasn’t worked with heavy loads enough. (Many people haven’t experienced enough stress in appropriate amounts in younger years to have learned how to cope with it.) The camel’s back is strong enough all right, but he just hasn’t worked out enough to build up supporting muscles. Or maybe it was the suddenness of the additional weight being added --too much all at once. He could have handled it had the load been added more gradually. Or maybe he’s carrying around such a heavy load all the time that he is constantly exhausted. (Many people constantly carry heavy loads of adverse past experiences around with them, which in turn keeps them emotionally run down.) (Roger Barrett, Depression, pp.26-27.)
There is in clinical psychology something which is called frustration or stress tolerance level.
Individuals do not have the same tolerance level in coping with stress. The same adverse event may be a precipitating or triggering event for emotional problems or depression for one individual and no problem at all to another person whose stress tolerance level is higher. Our ability to tolerate stress relates to what we call the “predisposing” factors. A person who has experienced an emotional breakdown may be healthier than either you or I who haven’t had such an experience. It’s just that he has experienced more stress than we have. Here Dr. Barrett has a helpful diagram to help us get a clear picture.
A and B show two similar stress levels. As you can see, Person A has experienced more stress at one
point in time than has Person B. Unfortunately, and with some pharisaical disdain, someone will point to Person A and say, “He’s emotionally weak” or “He has mental problems.” They won’t say the same about Person B, even though A and B are really of equal emotional stability.
It is even possible that someone with a lower stress tolerance level (“weak emotionally”) may not
experience emotional disorder or breakdown when a much stronger person may because he has experienced much more stress.
Person C has less good mental health or emotional stability than Person D. But he never experiences
more stress than he can cope with. Person D has considerable more ability to cope with stress by comparison to person C, but he has also far more severe and stressful events and problems, and they have, on one occasion, exceeded his ability to handle them.
Here are some of the characteristic stress factors in depression. The triggering factor in depression is
known as a stress factor. Psychologists have identified certain of these stress factors.
For men stress factors are most often events like financial reversals, failures in vocational identity
(failure to get job or promotion, etc.) and failing physical powers.
For women the stress factors are somewhat different. The major factors appear to be such events as an
attack on her femininity (e.g., a mastectomy or hysterectomy). Also a stress factor for women is the feeling of being abandoned by important men in her life such as her father or husband. The loss of children or trouble at home are stress factors in females which trigger depression.
Dr. Barrett reminds the student of depression that most of the precipitating factors involved in bringing
on depression involve the sense of worth an individual has of himself. Apparently the female’s sense of worth is tied very closely to her appearance and her relationship to her family members, whereas a man’s sense of worth is more closely tied to his work and his physical prowess. We might question whether this should be true for the Christian especially. Should these identities mean so much to us that their loss can have devastating effect on our emotional well-being? The loss or removal of anything we overvalue in terms of our security can trigger depression. A pertinent question here is: Are these the areas of life in which the Christian is to place his security? I doubt it!
So then, loss of loved ones, things in general, physical appearance or ability may all be precipitators to
depression. But on occasion there may not be a critical event or loss that will trigger depression. Instead, a long series of stresses or simply chronic stress finally topples the person’s emotional well-being and depression enters.
Constant fear and anxieties if not checked can, use up energy and exhaust oneself. If such stress is
severe enough and applied long enough, the hormonal reserves of the body become depleted. This results in fatigue and eventually exhaustion. The feeling side of this physical experience is depression. Pastors!—Here is a strong argument against allowing ourselves to be uptight, tense, nervous, and anxious all of the time. Eventually it catches up with us, and we leave ourselves open to the risk of depression.
What are the symptoms of depression? According to Dr. Adatto, who writes in a book called Learning
How to Live with Nervous Tension, a depressed person can be picked out if he has three main symptoms. “First, he is less interested in things than he used to be, whether these are work, hobbies, pets, friends, or people he loves. The second symptom is the fact that he cannot enjoy things as much as he-used to, whether it is a good dinner, a beautiful landscape, a theater performance, or some personal pleasure. Whatever it is, the enjoyment has gone out of it. The third symptom is that he cannot produce as much and as well as he did. a few months before. He gets fatigued much earlier and he cannot finish things” (p.66).
The seriously depressed person sees himself in a very negative way. He is convinced that he is “alone”
and helpless. He blames himself for ordinary faults and exaggerates his shortcomings. He is pessimistic not only about himself but about the world and the future. He wants to sleep for longer than usual. He may lose his appetite and lose weight, or eat more than normally and gain weight. Another characteristic, particularly evident in women, is crying spells, whether or not there is something to cry about. A severely depressed person often will say, “I’m scared I’m going out of my mind. I’ve been staring at the wall for three months. My children give
me no pleasure. I feel nothing for them. My husband has been forced to do the shopping and housework. I can’t move myself. I just can’t seem to do anything.”
Such people have lost confidence in themselves to carry out even the simple tasks of life. They describe
their depression as a wall between them and others. Many simply sleep all the time to avoid life’s troubles.
Some women express a sense of loss. They have gone through school, married, and raised children who
have grown up and left home and do not need them any more. The women sense a loss of purpose. Commonly, depressed people are more bothered by the body symptoms than by their sad feelings. They blame their mood on physical troubles. (“You’d be depressed too if you felt the pains I do.”) One study of 500 depressed patients showed that 74 percent had consulted a physician because of headaches, chest pains and the like. They believed that their mood change was the result, not the cause, of their body symptoms. Depression may masquerade as a skin condition, muscle aches and pains, urinary problems, stomach distress -- almost any bodily complaint.
There is no mistaking depression when the patient says that he has “no interest in living,” has feelings of
futility and hopelessness, and talks of wrist-slashing or jumping from a window or in front of a car. This is a red flare and calls for immediate steps to be taken.
The risk of suicide is great if the patient has an overwhelming sense of guilt and unworthiness, if he
talks of suicide or seems preoccupied with arranging his affairs.
At what point can a person tell if he should be seeking outside help for his depression? Here are some
general guidelines. He would be well advised to seek professional guidance if:
he finds himself continually unhappy with the way his life is going, he finds a marked drop in his ability to function at work, socially, and in his relationship
the condition persists for a month or two and he finds no specific reason for it and cannot
What kind of guidance should an individual seek? One would hope that Christians would first of all seek the
help and advice of their pastor. If indeed deep rooted feelings of inadequacy and guilt are at the heart of the depression, who better than God’s servant, the pastor, is able to apply Law and Gospel. Certainly the knowledgeable pastor will know his limits. He may first seek to find out if the problem is a medical or mental one. An easy way to help determine this is simply to send the patient to a physician as a matter of course for a routine physical. This will generally uncover any medical irregularities. If the problem is mental in nature, the pastor will seek to find the cause.
We have already noted somewhat how a pastor may be of help to the depressed. Let’s take a brief look also
at how the doctor or psychologist would deal with the depressed. Some doctors think drugs are very helpful. They claim that the introduction of antidepressant drugs has made the treatment of depression easier. Here are just a few samples. One type of antidepressant works by blocking the action of an enzyme in the brain that breaks down the chemical norepinephrine. In this way, it is believed, the drugs ensure adequate levels of the chemical. These include Marplan, Parnate, Nardil, and Eutonyl. A new class of antidepressant drugs, called tricyclics, prevent the breakdown of serotonin, the other major chemical believed to be involved in depression. These drugs include Tofranil and Sinequan.
When there is little of the chemicals norepinephrine and serotonin the emotional circuit is sluggish and a
person feels depressed. Just why there is a chemical drop in a depressed person is unknown. Drugs help restore the chemicals, but even if no drugs are used, nature eventually cures the bio-chemical illness. Drugs shorten the time and help a patient avoid needless suffering.
Sometimes drugs used in treatment have unpleasant side effects. Addiction is just one thing both doctor and
patient need to keep in mind. Here the doctor needs to monitor his patient carefully. There are many cases which have come to light in recent years where the doctor has not been responsible in this area.
Because the drugs are sometimes referred to as psychic energizers, a person might think they boost energies
to superhuman levels, like a missile fuel lifting a rocket into space. That is not the case. They are more like psychic restoratives, or psychic normalizers. They will act to lift the depressed energies of the patient up to his
best normal, but not beyond. There is no improvement in drive, character, or other attributes beyond those that were present before the depressive illness.
The drugs are convenient to take and enable family doctors to treat many depressions, and patients to
continue working while under medication. Clinical statistics show that drugs are effective in restoring patients to function in 50 to 80 percent of cases. Before there was a chemical treatment an average depression lasted two years. With chemical treatment, an average of 60 days will turn depressions around. These statistics are valid, I suppose, depending upon who you read. An article in Reader’s Digest (Dec. 1980, pp. 124-128) argues the method of “thinking one’s way out of depression.” According to their statistics, of 19 cognitive-therapy patients, 15 showed complete recovery. Only 5 of the 25 drug-therapy patients did as well, and 8 others dropped out because of side effects from the drug. A year later, 11 cognitive-therapy patients were still symptom-free—a significant finding since depression tends to become chronic.
Edward Ziegler, the author of “Think Your Way out of Depression,” states “that in cognitive therapy,
the doctor challenges the patient to listen to his own negative thoughts—trains him to identify these inner saboteurs and silence them. Results come quickly, usually within a few weeks.”
Dr. Burns offers these techniques to get the upper hand over your depression:
1. “Write down your negative thoughts. Don’t let them buzz in your head; snare them on
2. “Read over the list of cognitive distortions.”
3. “Substitute more objective thoughts that put the lie to the ones that made you depressed.”
Here is a sampling of the types of positive insights Burns offers to replace negative thoughts.
1. Your feelings are not facts! “Your feelings don’t even count, except to mirror your thinking. If
your thoughts make no sense, feelings they create will be just as absurd.”
2. You can cope. Even with genuine sadness due to real loss or disappointment, a substantial
portion of the suffering comes from thought distortion. “When you eliminate these distortions, coping with the real problem will become less painful.”
3. Don’t base your opinion of yourself on your achievements. “Self-worth based on
accomplishments is ‘pseudo-esteem’; not the genuine thing,” Burns says. You can’t base your self worth on looks, talent, fame or fortune. Marilyn Monroe, Freddie Prinze and other famous suicides attest to this grim truth. “Nor can love or approval add one iota to your inherent worth. Most depressed individuals are in fact much loved, but it doesn’t help. At the bottom line, only your own sense of self-worth determines how you feel.”
According to Ziegler, the main lesson of cognitive therapy is self-esteem. “Like yourself better and
“Self-esteem can be viewed as your decision to treat yourself like a beloved friend,” Burns says. He
asks: If a famous visitor came to stay with you, would you insult him? Would you peck away at his weaknesses and imperfections? Of course not. You would do everything you could to make your guest feel comfortable. “Now--why not treat yourself like that? Do it all the time!” (“Think you Way out of Depression,” Reader’s Digest, Dec. 1980, pp. 124-128.)
Obviously we cannot as Christians buy this kind of approach to depression. Rather we seek to let God’s
law point out our sins, we look at our disgusting state by nature and trust not in our own self-worth and esteem but in the active and passive righteousness of the God-man Jesus Christ who offered Himself as a sacrifice for us. This new status that we have as God’s children should go a long way in helping rid ourselves of depression. As blood-bought children of God, we have everything to live for; we really have hope—not only for this life but also for the life to come. It is indeed sad how many people will see secular counselors seeking to help them in their depression when only the Word of God will suffice. Here we see the need of mission work to solve man’s most basic need with the Gospel of the forgiveness of sins.
One last note along this line deals with the difference between depression and grief. Grief is a realistic
reaction to an actual loss about which there is full awareness. There are few psychosomatic symptoms, rarely any fear of an incurable disease, no fears of going insane. The grief-stricken person can concentrate and make decisions and manage his affairs.
In grief the loss is personal, objective, and readily understandable. The bereavement is realistic and in
proportion to what has been lost. It is self-limited and gradually subsides. In depression, on the other hand, the loss is much more complex. It is loss of self, the feeling of self-doubt, or self-contempt, even of self-loathing.
In summary, we can see that depressed people and depressed experiences vary both in quantity and
quality. Two persons, both of whom are experiencing depression, may have as many things different about their experience as similar. Not only are there multiple forms of expression of depression, but there are also many different causes of depression (as we will look at briefly next). Therefore, be careful how you apply what you read and learn concerning depression. Depression is much too complex to make easy individual application. What may be true for one depressed person may not in any way apply to another equally depressed person. (A. J. Snider and I. J. Adatto, M.D.’s, Learning How to Live with Nervous Tension, pp.62-79.)
In the next section of this paper, common causes of depression will be discussed. Since there is such a
wide range of opinions on this matter, we will try and describe just a few causes as simply and briefly as possible. This section, therefore, will not be exhaustive or inclusive.
First of all, we need to get the idea out of our heads that just because someone is depressed or has a
breakdown that he is emotionally weak. We all experience many of the same precipitating occurrences that bring on depression. The difference may be in our levels of tolerance and in the load. Dr. Roger Barrett points to “the straw that broke the camel’s back.” The camel’s broken back can be explained by a number of factors. Maybe we don’t have a very strong camel in the first place. He has a weak back. Or maybe he hasn’t worked with heavy loads enough. (Many people haven’t experienced enough stress in appropriate amounts in younger years to have learned how to cope with it.) The camel’s back is strong enough all right, but he just hasn’t worked out enough to build up supporting muscles. Or maybe it was the suddenness of the additional weight being added --too much all at once. He could have handled it had the load been added more gradually. Or maybe he’s carrying around such a heavy load all the time that he is constantly exhausted. (Many people constantly carry heavy loads of adverse past experiences around with them, which in turn keeps them emotionally run down.) (Roger Barrett, Depression, pp.26-27.)
There is in clinical psychology something which is called frustration or stress tolerance level.
Individuals do not have the same tolerance level in coping with stress. The same adverse event may be a precipitating or triggering event for emotional problems or depression for one individual and no problem at all to another person whose stress tolerance level is higher. Our ability to tolerate stress relates to what we call the “predisposing” factors. A person who has experienced an emotional breakdown may be healthier than either you or I who haven’t had such an experience. It’s just that he has experienced more stress than we have. Here Dr. Barrett has a helpful diagram to help us get a clear picture.
A and B show two similar stress levels. As you can see, Person A has experienced more stress at one
point in time than has Person B. Unfortunately, and with some pharisaical disdain, someone will point to Person A and say, “He’s emotionally weak” or “He has mental problems.” They won’t say the same about Person B, even though A and B are really of equal emotional stability.
It is even possible that someone with a lower stress tolerance level (“weak emotionally”) may not
experience emotional disorder or breakdown when a much stronger person may because he has experienced much more stress.
Person C has less good mental health or emotional stability than Person D. But he never experiences
more stress than he can cope with. Person D has considerable more ability to cope with stress by comparison to person C, but he has also far more severe and stressful events and problems, and they have, on one occasion, exceeded his ability to handle them.
Here are some of the characteristic stress factors in depression. The triggering factor in depression is
known as a stress factor. Psychologists have identified certain of these stress factors.
For men stress factors are most often events like financial reversals, failures in vocational identity
(failure to get job or promotion, etc.) and failing physical powers.
For women the stress factors are somewhat different. The major factors appear to be such events as an
attack on her femininity (e.g., a mastectomy or hysterectomy). Also a stress factor for women is the feeling of being abandoned by important men in her life such as her father or husband. The loss of children or trouble at home are stress factors in females which trigger depression.
Dr. Barrett reminds the student of depression that most of the precipitating factors involved in bringing
on depression involve the sense of worth an individual has of himself. Apparently the female’s sense of worth is tied very closely to her appearance and her relationship to her family members, whereas a man’s sense of worth is more closely tied to his work and his physical prowess. We might question whether this should be true for the Christian especially. Should these identities mean so much to us that their loss can have devastating effect on our emotional well-being? The loss or removal of anything we overvalue in terms of our security can trigger depression. A pertinent question here is: Are these the areas of life in which the Christian is to place his security? I doubt it!
So then, loss of loved ones, things in general, physical appearance or ability may all be precipitators to
depression. But on occasion there may not be a critical event or loss that will trigger depression. Instead, a long series of stresses or simply chronic stress finally topples the person’s emotional well-being and depression enters.
Constant fear and anxieties if not checked can, use up energy and exhaust oneself. If such stress is
severe enough and applied long enough, the hormonal reserves of the body become depleted. This results in fatigue and eventually exhaustion. The feeling side of this physical experience is depression. Pastors!—Here is a strong argument against allowing ourselves to be uptight, tense, nervous, and anxious all of the time. Eventually it catches up with us, and we leave ourselves open to the risk of depression.
What are the symptoms of depression? According to Dr. Adatto, who writes in a book called Learning
How to Live with Nervous Tension, a depressed person can be picked out if he has three main symptoms. “First, he is less interested in things than he used to be, whether these are work, hobbies, pets, friends, or people he loves. The second symptom is the fact that he cannot enjoy things as much as he-used to, whether it is a good dinner, a beautiful landscape, a theater performance, or some personal pleasure. Whatever it is, the enjoyment has gone out of it. The third symptom is that he cannot produce as much and as well as he did. a few months before. He gets fatigued much earlier and he cannot finish things” (p.66).
The seriously depressed person sees himself in a very negative way. He is convinced that he is “alone”
and helpless. He blames himself for ordinary faults and exaggerates his shortcomings. He is pessimistic not only about himself but about the world and the future. He wants to sleep for longer than usual. He may lose his appetite and lose weight, or eat more than normally and gain weight. Another characteristic, particularly evident in women, is crying spells, whether or not there is something to cry about. A severely depressed person often will say, “I’m scared I’m going out of my mind. I’ve been staring at the wall for three months. My children give
me no pleasure. I feel nothing for them. My husband has been forced to do the shopping and housework. I can’t move myself. I just can’t seem to do anything.”
Such people have lost confidence in themselves to carry out even the simple tasks of life. They describe
their depression as a wall between them and others. Many simply sleep all the time to avoid life’s troubles.
Some women express a sense of loss. They have gone through school, married, and raised children who
have grown up and left home and do not need them any more. The women sense a loss of purpose. Commonly, depressed people are more bothered by the body symptoms than by their sad feelings. They blame their mood on physical troubles. (“You’d be depressed too if you felt the pains I do.”) One study of 500 depressed patients showed that 74 percent had consulted a physician because of headaches, chest pains and the like. They believed that their mood change was the result, not the cause, of their body symptoms. Depression may masquerade as a skin condition, muscle aches and pains, urinary problems, stomach distress -- almost any bodily complaint.
There is no mistaking depression when the patient says that he has “no interest in living,” has feelings of
futility and hopelessness, and talks of wrist-slashing or jumping from a window or in front of a car. This is a red flare and calls for immediate steps to be taken.
The risk of suicide is great if the patient has an overwhelming sense of guilt and unworthiness, if he
talks of suicide or seems preoccupied with arranging his affairs.
At what point can a person tell if he should be seeking outside help for his depression? Here are some
general guidelines. He would be well advised to seek professional guidance if:
he finds himself continually unhappy with the way his life is going, he finds a marked drop in his ability to function at work, socially, and in his relationship
the condition persists for a month or two and he finds no specific reason for it and cannot
What kind of guidance should an individual seek? One would hope that Christians would first of all seek the
help and advice of their pastor. If indeed deep rooted feelings of inadequacy and guilt are at the heart of the depression, who better than God’s servant, the pastor, is able to apply Law and Gospel. Certainly the knowledgeable pastor will know his limits. He may first seek to find out if the problem is a medical or mental one. An easy way to help determine this is simply to send the patient to a physician as a matter of course for a routine physical. This will generally uncover any medical irregularities. If the problem is mental in nature, the pastor will seek to find the cause.
We have already noted somewhat how a pastor may be of help to the depressed. Let’s take a brief look also
at how the doctor or psychologist would deal with the depressed. Some doctors think drugs are very helpful. They claim that the introduction of antidepressant drugs has made the treatment of depression easier. Here are just a few samples. One type of antidepressant works by blocking the action of an enzyme in the brain that breaks down the chemical norepinephrine. In this way, it is believed, the drugs ensure adequate levels of the chemical. These include Marplan, Parnate, Nardil, and Eutonyl. A new class of antidepressant drugs, called tricyclics, prevent the breakdown of serotonin, the other major chemical believed to be involved in depression. These drugs include Tofranil and Sinequan.
When there is little of the chemicals norepinephrine and serotonin the emotional circuit is sluggish and a
person feels depressed. Just why there is a chemical drop in a depressed person is unknown. Drugs help restore the chemicals, but even if no drugs are used, nature eventually cures the bio-chemical illness. Drugs shorten the time and help a patient avoid needless suffering.
Sometimes drugs used in treatment have unpleasant side effects. Addiction is just one thing both doctor and
patient need to keep in mind. Here the doctor needs to monitor his patient carefully. There are many cases which have come to light in recent years where the doctor has not been responsible in this area.
Because the drugs are sometimes referred to as psychic energizers, a person might think they boost energies
to superhuman levels, like a missile fuel lifting a rocket into space. That is not the case. They are more like psychic restoratives, or psychic normalizers. They will act to lift the depressed energies of the patient up to his
best normal, but not beyond. There is no improvement in drive, character, or other attributes beyond those that were present before the depressive illness.
The drugs are convenient to take and enable family doctors to treat many depressions, and patients to
continue working while under medication. Clinical statistics show that drugs are effective in restoring patients to function in 50 to 80 percent of cases. Before there was a chemical treatment an average depression lasted two years. With chemical treatment, an average of 60 days will turn depressions around. These statistics are valid, I suppose, depending upon who you read. An article in Reader’s Digest (Dec. 1980, pp. 124-128) argues the method of “thinking one’s way out of depression.” According to their statistics, of 19 cognitive-therapy patients, 15 showed complete recovery. Only 5 of the 25 drug-therapy patients did as well, and 8 others dropped out because of side effects from the drug. A year later, 11 cognitive-therapy patients were still symptom-free—a significant finding since depression tends to become chronic.
Edward Ziegler, the author of “Think Your Way out of Depression,” states “that in cognitive therapy,
the doctor challenges the patient to listen to his own negative thoughts—trains him to identify these inner saboteurs and silence them. Results come quickly, usually within a few weeks.”
Dr. Burns offers these techniques to get the upper hand over your depression:
1. “Write down your negative thoughts. Don’t let them buzz in your head; snare them on
2. “Read over the list of cognitive distortions.”
3. “Substitute more objective thoughts that put the lie to the ones that made you depressed.”
Here is a sampling of the types of positive insights Burns offers to replace negative thoughts.
1. Your feelings are not facts! “Your feelings don’t even count, except to mirror your thinking. If
your thoughts make no sense, feelings they create will be just as absurd.”
2. You can cope. Even with genuine sadness due to real loss or disappointment, a substantial
portion of the suffering comes from thought distortion. “When you eliminate these distortions, coping with the real problem will become less painful.”
3. Don’t base your opinion of yourself on your achievements. “Self-worth based on
accomplishments is ‘pseudo-esteem’; not the genuine thing,” Burns says. You can’t base your self worth on looks, talent, fame or fortune. Marilyn Monroe, Freddie Prinze and other famous suicides attest to this grim truth. “Nor can love or approval add one iota to your inherent worth. Most depressed individuals are in fact much loved, but it doesn’t help. At the bottom line, only your own sense of self-worth determines how you feel.”
According to Ziegler, the main lesson of cognitive therapy is self-esteem. “Like yourself better and
“Self-esteem can be viewed as your decision to treat yourself like a beloved friend,” Burns says. He
asks: If a famous visitor came to stay with you, would you insult him? Would you peck away at his weaknesses and imperfections? Of course not. You would do everything you could to make your guest feel comfortable. “Now--why not treat yourself like that? Do it all the time!” (“Think you Way out of Depression,” Reader’s Digest, Dec. 1980, pp. 124-128.)
Obviously we cannot as Christians buy this kind of approach to depression. Rather we seek to let God’s
law point out our sins, we look at our disgusting state by nature and trust not in our own self-worth and esteem but in the active and passive righteousness of the God-man Jesus Christ who offered Himself as a sacrifice for us. This new status that we have as God’s children should go a long way in helping rid ourselves of depression. As blood-bought children of God, we have everything to live for; we really have hope—not only for this life but also for the life to come. It is indeed sad how many people will see secular counselors seeking to help them in their depression when only the Word of God will suffice. Here we see the need of mission work to solve man’s most basic need with the Gospel of the forgiveness of sins.