Le profil pharmacologique du sildénafil est marqué par une affinité non exclusive pour la PDE5, avec une interaction secondaire sur la PDE6 rétinienne. Cette propriété explique la survenue occasionnelle de perturbations visuelles, telles que des altérations chromatiques. Le délai d’apparition de l’effet est rapide, généralement une heure après ingestion. Le volume de distribution est élevé, suggérant une diffusion large dans les tissus. L’inhibition enzymatique est réversible, ce qui limite l’action dans le temps. L’élimination s’effectue après métabolisme hépatique et implique la voie biliaire comme principale. Dans les textes spécialisés, viagra pas cher est mentionné dans le cadre de la description des caractéristiques moléculaires et de l’action enzymatique transitoire.
Kamje.or.kr
S a lv a g e T h er a py w it h T h a lidom ide in P a t ien t s w it h
Re la ps e d or Re f r a ct or y M u lt iple M y e lom a
Do Yeun Kim, M.D.1, Seock- Ah Im, M.D.1, Chu- Myong Seong, M.D.1, Soon Nam Lee, M.D.1,
Soo- Mee Bang, M.D.2, Jae Hoon Lee, M.D.2, Sung- Soo Yoon, M.D.3, Byoung Kook Kim, M.D.3,
Seon Yang Park, M.D.3 and Myung- Ju Ahn, M.D.4
D e p ar t m e nt of I n t e rn al M e d icine 1, E w ha W om ans U niv e r s it y C olle g e of M e d icine ,D e p ar t m e nt of I n t e rn al M e d icine 2, Gachon M e d ical C e nt e r ,D e p art m e nt of I nt e rn al M e d icine 3, S e ou l N at ional U niv e r s it y C olle g e of M e d icin e , andD e p ar t m e n t of I nt e r nal M e d icine 4, H any an g U n iv e rs it y C olle g e of M e d icine , S e ou l, K ore aB a c k g ro un d : The re are few therape utic op- Re s u lts : The se rum or urine levels of pa -
tions for patie nts with multiple mye loma who
raprotein were reduced by a t le ast 90 pe rcent
relapse after autologous or a llogeneic ste m cell
in two patients , a t lea st 50 perce nt in three
patients , and at lea st 25 perce nt in two pa-
fractory to conventiona l chemothe rapy a nd not
tients; for a total res ponse rate of 25 pe rcent.
e ligible for s alvage high- dos e the rapy. Tha lido-
13 patients had sta ble dis eas e and 8 patients
mide, a potent antiangiogenic agent, has bee n
had progres se d. At lea st ha lf of the patie nts
s ugge ste d as an effective sa lva ge thera py in
refra ctory multiple myeloma. The aim of this
tigue . More severe advers e effects were in-
Co nc lus io n : This study confirms that tha-
lidomide is an effective and safe agent in pa-
Me t h o d : From February 2001 to September
tients with relapsed or refractory multiple mye-
loma. (Korean J Hematol 2002;38:259
included. At sta rt of treatment, all patie nts ha d
Ke y Words : Thalidomide, Multiple myeloma
a ctive dise as e and 17 (61%) had received at
le as t one autologous trans pla ntation.
r elaps e r ate r emains hig h in all patient s , s o the dis eas e
Recently, it has been r eport ed t hat ang iog enes is is
v as cular endothelial g row t h fact or (VEGF ) and bas ic
chem other apy to hig h- dos e chemotherapy follow ed by
peripheral s tem cell or bone m arrow t rans plantation.1)
ant i- ang iog enic dr ug plays the treat ment for my eloma.
T halidom ide is a glutam ic acid deriva tive that
dis appoint ing . M elphalan bas ed high dos e chemot herapy
s how s a potent a ntiangiogenic activity.7,8) Als o, this
drug has been found as im munom odulatory proper-
ties and an effective inhibitor of T NF - alpha.9) Re-
cognition of its a nti- a ngiog enic effect led to its
evalua tion in the treatm ent of various m alignancies ,
Correspondence : Soon Nam Lee M.D., Department of Interna
w here angiogenes is has been s how n to play an
Do Ye un Kim : Thalidomide in Multiple Mye loma
In 1999, Singhal et al. reported the overall respons e
lines). T he previous therapy included either single (N=
rate of 32% of thalidomide in 84 heavily pre- treated
15) or double (N=2) autologous trans plantation. T here
w as 1 patient who received autologous transplant and
after then allogeneic trans plant due to diseas e progres-
confirmed by numerous studies.11 13) We report the
sion. Disease status at study entry w as evaluated w ith
res ults of a retrospective study of the 28 Korean
res pect to the last line of treatment the patient had
patients from 4 centers with refractory or relaps ed
received before thalidomide therapy; 23 patients (82%)
w ere class ified as relapsed and 5 patients (8%) as re-
Complete respons e was defined as lack of detectabl
M- component in serum and/ or urine. Partial and minor
Between February 2001 and September 2002, 28
res ponses w ere defined as 50% and 25% M- component
patients from 4 centers w ere enrolled. Patients' charac
reduction in serum and/or urine, respectively. Patients
teristics at the onset of thalidomide treatment ar
w ith a reduction of les s than 25 percent without ev
presented in table 1. T he median age was 54 years
dence of additional myeloma- related complications w er
considered to no res ponse. Patients w ere cons idered in
93% w ere s tage III. T he median time from diagnosis to
thalidomide therapy w as 31 months. Prior to thalido
res ponse or stable disease. In patients with a res ponse,
mide therapy, 10 patients had been treated with con-
an increase in serum or urine paraprotein levels b
ventional chemotherapy alone (1 4 lines, median 2
more than 25 percent above the nadir value w as con
Participating centers were asked to provide detaile
information about the occurrence of side effect, their
onset date, duration and intensity and about the tha
lidomide dose modifications which w ere due to thes
side effect. We confirmed these contents by telephone
Overall survival (OS) w as defined as the time elapse
form onset of thalidomide to death whatever the caus
Dis ea se s tatus at the ons et of thalidomide
of death. Event free survival (EFS) was defined as th
time elaps ed from the onset of thalidomide to pro
gres sion, s top medication of thalidomide for any rea
son, death from any cause, or the last follow - up visit,
w hichever occurred first. Dis tributions over time w er
estimated by Kaplan- Meier analysis.
months (range; 3.6 15.4). T hirteen patients had sta-
ble disease. Eight patients progressed.
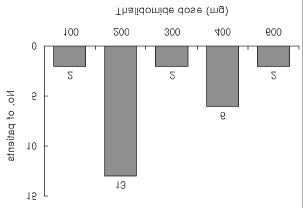
Distribution of the maximum tolerated dose of tha
summarized in T able 2. T w o patients(7%) achieved a
lidomide is show n in Fig. 1. T hree patients w ho stop-
complete response. Partial response was observed in 3
ped thalidomide medication due to WHO grade
patients (11%) and there w as minimal response in 2
toxic effects w ere not cons idered. T hirteen patient
patients (7%). T hus, the overall response rate was
(52%) took the 200mg dose. No patients did not take
25%. T he hemoglobin levels and platelet count were
dose of thalidomide up to 800mg. WHO grade
improved in 2 patients among responders.
effects such as skin ras h, paresthes ia and constipation
One patient of complete responder w as relapsed afte
prompted dose reduction in 3 patients. As shown in
w ithdraw al of thalidomide due to grade 3 skin rash
T able 3, constipation (68%) and lethargy (54%) w ere
One patient who show ed minimal response w as relapse
the most frequent adverse events . No thalidomide-
after self w ithdraw al of thalidomide. T he median inter
related mortality w as noted and most of toxicities we
val betw een ons et of thalidomide and the firs t decreas
grade 1 or 2. Neurologic toxicity such as dizziness,
of M- protein by at least 25% w as 1.7 months (range;
tingling sensation was obs erved in 4 patients . Nin
1.9). T he median response duration w as 7.7
patients experienced skin rash, in three cases treatmen
3. Event free survival and overall survival
T he median follow- up duration from the start o
thalidomide treatment w as 5.8 months . T w enty tw
patients are still alive and followed up as outpatien
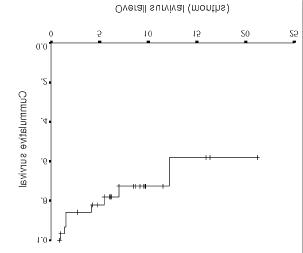
T he median EFS was 4 months (Fig. 2). T he median
time to OS had not been reached. After 12 months
follow- up, 58 percent of patients w ere alive (Fig. 3). Fig. 1. Dis tribution of the ma ximum tole ra te d dose of tha-
Do Ye un Kim : Thalidomide in Multiple Mye loma
anti- multiple myeloma cells effect. T he median time to
res ponse w as rapid similar to other study. Even
though we did not observe bone marrow angiogenesis
after thalidomide, there were no statistically significant
in pos ttreatment microvessel dens ity.10)
From these tw o points of observations, possible other
mechanis ms of thalidomide except angiogenesis are
immunomodulary agents such as potent inhibitor of
T - cell proliferation15) and secretion of interferon-
In addition, it may modulates the expression of cell
surface adhesion molecules16) that allow myeloma cells
Fig. 2. Kaplan- Meier es timate of event fre e s urviva l.
to interact with the bone marrow microenvironment.
So it may be action of mechanis m to myeloma cells
w hich complex effects on tumor angiogenesis, the
immune system, and various cytokines and adhesion
molecules. By searching the more detailed mechanis ms
of action of thalidomide to plas ma cells , it w ill
contribute to new insight into tumor biology and
T he optimal dose of thalidomide remains to be
determined. Barlogie et al. concluded that there is a
dose- response relationship betw een tumor cell reduc
tion and a cumulative dose of thalidomide.17) In con-
trast, other studies achieved comparable results using
much low er dose of the drug.18,19) Also, in our study,
median dos e betw een responder and nonresponder w as
not different. T his means for some subset of patients
Fig. 3. Kaplan- Meier es timate of overall survival.
dose de- es calation may be necessary w ithout sufferin
toxicities. T his iss ue must be solved w ith the detaile
mechanis m of action of thalidomide to myeloma.
T he overall response rate in most studies so fa
While conventional therapies have become inef
reported averages approximately 30%.11 13) T he re-
fective in patients w ith refractory myeloma, thalidomid
sponse rate with 25% of this s tudy is s lightly belo
given substantial respons e. We observed tha
compared to other studies. We can' t assure that rel-
angiogenesis is increased in myeloma.6) Antiangiogenic
atively low dose of thalidomide in our patients ma
therapy represents a novel and pos sibly less tox
contribute, though the dose- response relation is not
T his study confirms an antitumor activity of thalid
T he predictive factors which indicators are associate
mide to advanced multiple myeloma. Since almost al
response of thalidomide to myeloma patient
available therapy for relapse had failed in most of thes
remains to be unsolved. Barlogie et al have reported
patients, the respons es observed are impres sive.
that normal cytogenetic, low plasma cell labeling index
thalidomide.17) Dose res ponse effect w as apparent in
labeling index. Meanwhile, intergroupe francophone du
myeloma (IFM) defined poor risk features s uch as IgA
level < 3g/ dL for myeloma patients with treatment of
thalidomide.20) We had limitation for analyze about this
As many other reports, constipation was the mos
common side effect. Almost of the toxicities were mil
and eas ily manageable w ithout drug- related mortality
T he incidence of skin rash w as slightly more commo
compared to other study. T he s ide effect was dos e
dependent. Reducing the dose of thalidomide alleviated
the effects in 3 patients. One patient, who developed
grade 3 skin rash during dose up to 600mg, stopped
taking thalidomide for 1 month, and then restarted
1) Alex anian R, Dim opoulos M : T he tre at m e nt of m ul-
w ithout skin rash. Side effect such as deep vein
tiple m y elom a. N E ng l J M ed 330:484- 489, 1994
thrombosis w as not noted. Hematologic toxicity w as no
2) Bar log ie B : A d vances in the rapy of m ultiple m ye -
remarkable. Recent report about the adverse effect o
thalidomide in advanced myeloma concluded that safet
of higher dose (800 mg/ day) of thalidomide given over
F uzibet JG, Ros s i JF , Cas as s us P, Mais onneuve H,
a long period(> 15 months).21) All the adverse effects
s pectiv e , random iz e d trial of autolog ous bone m ar-
did not warrant decreas e or termination of therapy, and
row t rans plantation and che m othe rapy in m ult iple
then tolerance developed to sedation, cons tipation, and
m y elom a. N E ng l J M e d 335:91- 99, 1996
skin les ion later. But the patients in our study tolerated
4) Vacca A, Ribatti D, Roncali L, S erio G, S ilves t ris
poorly to dose escalation schedule. We ass ume that
prog re ss ion in m ultiple m ye lom a. B r J H ae m atol
there are possible pharmacodynamic differencies o
Overally thalidomide w as an effective and s afe drug
Recently, thalidomide in combination with other drugs
is investigated actively.22,23) Also the role as remission
6) P ark SY, Im S A, Nam EM, Kim DY, Choi YA, Lee
induction or maintenance therapy still need to be deter
and inte rle uk in- 6 in m ultiple m ye lom a. K orean J
7) D' Amato RJ, Loughnan MS , F ly nn E, F olkaman J :
T halidom ide is an inhibitor of ang iog enes is . P rocN atl A cad S ci U S A 91:4082- 4085, 1994
8) Bauer KS, Dix on S C, F ig g W D : I nhibitor of ang io-g e ne sis by thalidom ide re quires m e tabolic act iva-
Do Ye un Kim : Thalidomide in Multiple Mye loma
s pe cie s - de pend ent . B ioche mnopharm acolog y 31:213- 221, 1996
17) Bar log ie B, Des ikan R, Eddlem on P , Spencer T ,
Zeldis J, Muns hi N, Badr os A, Zang ari M, Anais s ie
E, Eps tein J, Shaug hnes s y J, Ayer s D, S poon D,
phocyt e, prefere ntially inducing proliferation, cy to-
T ricot G : E xte nde d s urv ival in advance d and re -fractory m ultiple m ye lom a afte r sing le- ag e nt tha-subs e t. J E xp M e d 187:1885- 1892, 1998lidom ide : I de ntificat ion of prog nos tic factors in a
10) S ing hal S , Mehta J, Des ikan R, Ayer s D, Robers on
phas e 2 st udy of 169 patie nts . B lood 98:492- 494,
P , Eddlemon P, Muns hi N, Anais s ie E, W ils on C,
Dhodapkar M, Zeddis J, Bar log ie B : A ntit um or acti-
18) P ini M, Baraldi A, Pietr as anta D, Allione B, Depaoli
v ity of thalidom ide in re fractory m ultiple m y elom a
L, S alvi F : L ow dos e t halidom ide in the tre at m e ntN E ng l J M e d 341:1565- 1571, 1999of re fractory m ye lom a. H em at olog ica 85: 1111- 1112,lidom ide in m ult iple m ye lom a. Cancer T re at R eve ffe ct ive in m ultiple m ye lom a. L ance t 354:925, 1999
20) Yakoub- Ag ha I, Attal M, Dumontet C, Delannoy V,
12) Rajkumar S V, F ons eca R, Dis penzier e A, Lacy MQ,
Berthou C, Lam y T , Durv aus V, Monconduit M,
Lus t JA, W itzig T E, Kyle RA, Gert z MA, Gr eipp
Dug uet C, Duhamel A, F acon T : T halidom ide in
P R : T halidom ide in the tre at m e nt of re lapse d m ul-patie nts with advanced m ultiple m ye lom a: A s tudyt iple m ye lom a. M ayo Clin P roc 75:897- 902, 2000of 83 patie nts - report of the inte rg roupe francophone
13) Julius s on G, Cels ing F , T ur es s on I : F re quent g ooddu m ye lom a (I F M ) . H e m atolog y J 3:185- 192, 2002partial re m is sions from thalidom id e includ ing be st
21) Grov er JK, Uppal G, Raina V: T he adv ers e e ffe ct ofre spons e ev er in patie nts with adv ance d re fractoryt halidom ide in re lapse d and refractory patie nts ofand re lapse d m ye lom a. B r J H em at ol 109:89- 96,m ultiple m ye lom a. A nn Oncol 13:1636- 1640, 2002
22) Rajkumar S V, Hayman S, Ger tz MA, Dis penzier i A,
14) S am paio EP, S arno EN, Galilly R, Cohn ZA, Kaplan
Lacy MQ, Gr eipp PR, Geyer S , It ur ria N, F ons eca
G : T halid om ide se le ctive ly inhibits tum or ne cros isfact or alpha product ion by st im ulate d hum an m ono-cyt es . J E xp M e d 173:699- 670, 1991ne wly diag nose d m ye lom a. J Clin Oncol 20:4319-
15) McHug h S M, Rifkin IR, Deig hton J, W ils on AB,
Lopez C, Gonzalez M, S an Mig uel JF : T he com -he lpe r ce ll t ype 2 ( T h2) and concom it ant ly inhibit sbination of t halidom ide , cyclophos pham ide and de -T h1 cyt ok ine production in m itog e n- and antig en-xam e thasone (T haCyD e x) is fe asible and can be ans tim ulat ed hum an pe riphe ral blood m ononuclear cellculture s. Clin E xp I m m unol 99:160- 167, 1995
16) Geit z H, Handt S, Zw ing enberg er K : T halidom idem olecule s inv olve d in the adhe sion cas cad e. I m m u-
State of Connecticut Department of Consumer Protection NARCOTICS & VARIOUS OTHER CONTROLLED SUBSTANCES January 2000 Prepared by: Drug Control Agent Sharon Milton-Wilhelm Drug Control Agent Gerald J. DeStefano TABLE OF CONTENTS PAGE NUMBER Amphetamines (Methamphetamine, ICE, CAT) Marijuana (including Sinsemilla, Hash, Hash Oil) Amphetamine Variants
GENDER MEDICINE/VOL. 7, NO. 4, 2010 Commentary Sex, Gender, and Pharmaceutical Politics: From Drug Development to Marketing Jill A. Fisher, PhD1; and Lorna M. Ronald, PhD2 1Center for Biomedical Ethics & Society, Vanderbilt University, Nashville, Tennessee; and 2Interdisciplinary Studies Program, John Jay College (City University of New York), New York, New York Background
 months (range; 3.6 15.4). T hirteen patients had sta-
ble disease. Eight patients progressed.
months (range; 3.6 15.4). T hirteen patients had sta-
ble disease. Eight patients progressed.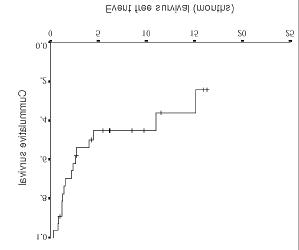
 Do Ye un Kim : Thalidomide in Multiple Mye loma
anti- multiple myeloma cells effect. T he median time to
res ponse w as rapid similar to other study. Even
though we did not observe bone marrow angiogenesis
after thalidomide, there were no statistically significant
in pos ttreatment microvessel dens ity.10)
From these tw o points of observations, possible other
mechanis ms of thalidomide except angiogenesis are
immunomodulary agents such as potent inhibitor of
T - cell proliferation15) and secretion of interferon-
In addition, it may modulates the expression of cell
surface adhesion molecules16) that allow myeloma cells
Fig. 2. Kaplan- Meier es timate of event fre e s urviva l.
Do Ye un Kim : Thalidomide in Multiple Mye loma
anti- multiple myeloma cells effect. T he median time to
res ponse w as rapid similar to other study. Even
though we did not observe bone marrow angiogenesis
after thalidomide, there were no statistically significant
in pos ttreatment microvessel dens ity.10)
From these tw o points of observations, possible other
mechanis ms of thalidomide except angiogenesis are
immunomodulary agents such as potent inhibitor of
T - cell proliferation15) and secretion of interferon-
In addition, it may modulates the expression of cell
surface adhesion molecules16) that allow myeloma cells
Fig. 2. Kaplan- Meier es timate of event fre e s urviva l.